
Abstract
Mesentero-axial gastric volvulus is a rare presentation to a surgical casualty unit with sinister complications and significant mortality and morbidity. Clinical assessment should be done with high suspicion in the case of an associated anatomical defect. Accurate diagnosis and timely intervention would drastically reduce morbidity and mortality. The present patient is a 63-year-old male with an acute and chronic presentation of a secondary mesentero-axial gastric volvulus with a large hiatal hernia who underwent open surgical repair with unremarkable postop recovery.
Introduction
Gastric volvulus (GV) is characterized by rotation of the stomach along its long or short axis leading to ischaemic and gastric perforation. There are several classifications of GV; it is classified based on its axis of rotation, organo-axial or mesentero-axial. In organo-axial GV, the stomach antrum rotates anterosuperiorly and the fundus rotates posteroinferiorly, and in mesentero-axial gastric volvulus (MAGV), the stomach rotates around the short axis where the antrum is above the gastroesophageal junction. MAGV is an uncommon subtype of GV. 1 Most present with abdominal or lower chest pain with severe vomiting and are often missed due to its rarity. More than 70% of patients present with Borchardt’s triad which includes abdominal pain, vomiting and the inability to pass a nasogastric tube.2,3 If there is a complete obstruction of the gastric outlet, it will lead to ischaemia, strangulation followed by necrosis, perforation and intra-abdominal sepsis. 1 Therefore, higher rates of morbidity and mortality can occur with delaying diagnosis. 2 The available literature is mostly limited to a few case reports; its rarity makes a prospective evaluation difficult.
Case presentation
A 63-year-old male presented with a 2-week history of gradual onset upper abdominal pain and distention with non-bilious profuse vomiting following meals worsening over 3 days. There was no haematemesis or associated dyspeptic symptoms. The patient had normal bowel habits with normal urine output, and there was no prior history of thoracic or abdominal surgeries. On general examination, the patient was afebrile with stable vital signs, and the abdomen was distended with mild tenderness over the epigastric region and no features suggestive of peritonitis.
The initial investigation only showed mild neutrophilic leucocytosis (white blood cell (WBC) = 11 × 103/L) and hypokalaemia (3.0 mmol/L). An erect chest X-ray showed a double air-fluid level. The Ultrasound scan of the abdomen showed a distended stomach with fluid. A contrast-enhanced computed tomography (CECT) of the abdomen revealed a grossly distended stomach with antropyloric junction superior and anterior to the gastroesophageal junction with a large hiatal hernia without any evidence of perforation or perigastric fluid collection which confirmed MAGV (Figures 1 and 2).

Contrast-enhanced CT image showing the mesentero-axial gastric volvulus.
Gastric volvulus before reduction.
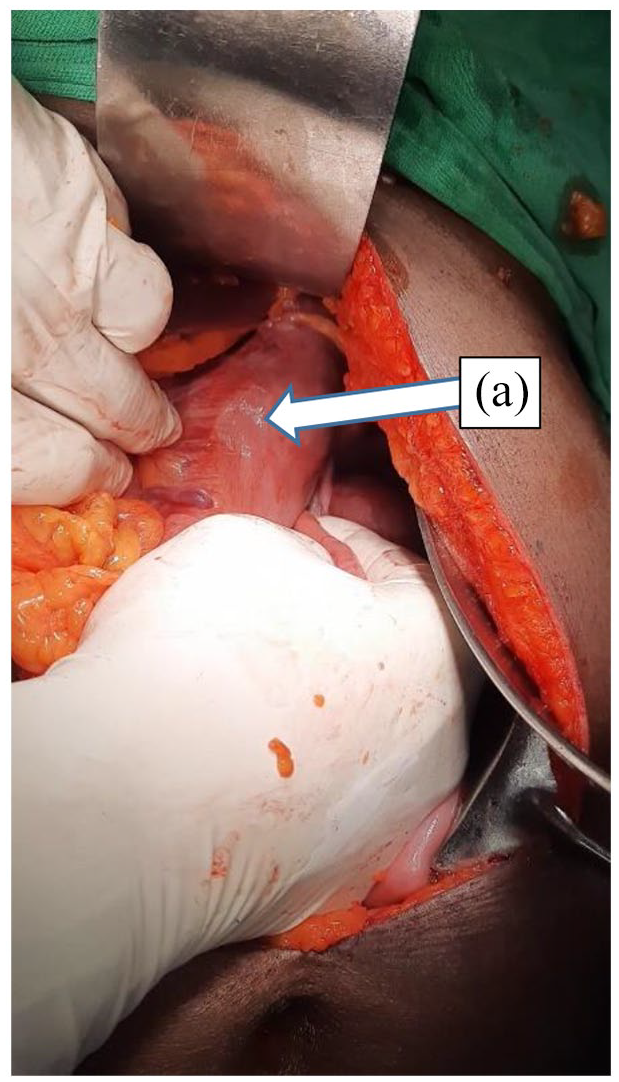
A nasogastric tube was inserted subsequently which had a continuous drain of clear, non-bilious fluid. After initial symptomatic management 72 h later, a laparotomy was performed, and GV was identified (Figure 3) where reduction of the stomach from the hernia and derotation of the stomach was performed (Figure 4). There were no gastric perforations or necrosis noted during the surgery. A 4 cm × 4 cm size defect was identified in the diaphragm (Figure 4). The diaphragmatic defect was repaired by closing the defect in the hiatus with 1/0 nylon suture without mesh repair. Gastropexy was done where the anterior wall of the stomach was attached to the anterior abdominal wall using 2/0 polyglactin. The patient had an uneventful recovery following surgery with a total postoperative hospital stay of 3 days.

Gastric volvulus after reduction (a) the antrum of the stomach and (b) the fundus of the stomach.
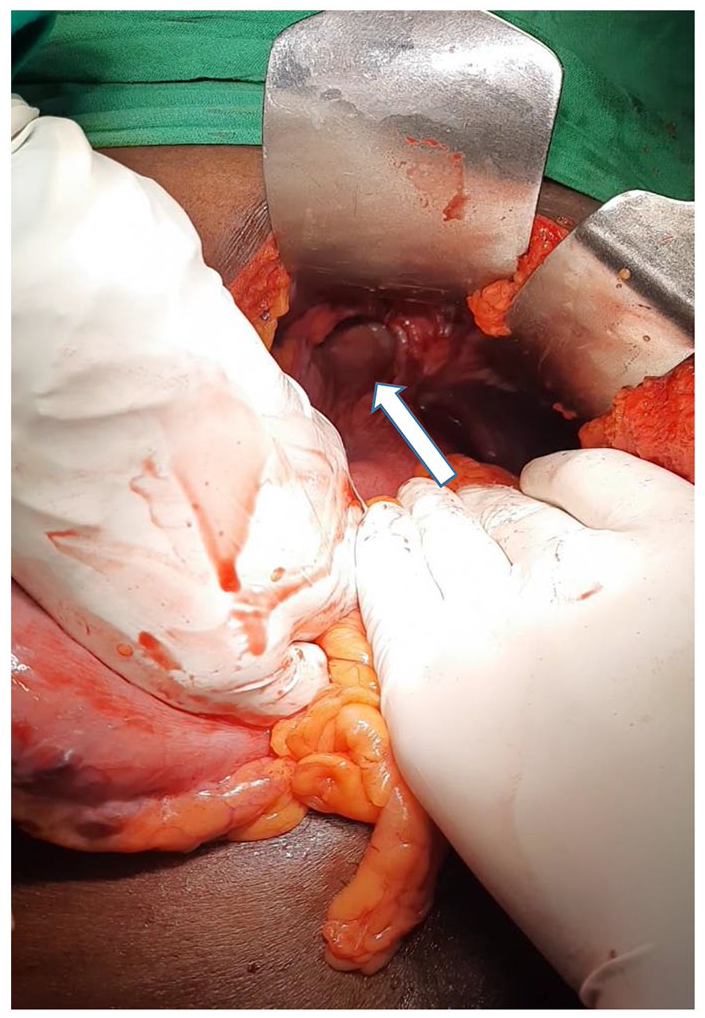
The diaphragmatic hiatus.
Discussion
GV is quite an elusive diagnosis due to its rarity. It commonly occurs in the adult population, where the incidence peaks in the fifth decade. 4 However, there are a few factors predisposing such as diaphragmatic abnormalities, phrenic nerve paralysis and other gastrointestinal anatomical abnormalities, and kyphoscoliosis. 1 There are several classifications of GV depending on the axis of rotation as in the index case of MAGV. Depending on the aetiology of the rotation, GV is classified as primary or secondary. 2 Primary GV arises due to an abnormality in gastric ligaments. 3 This can be caused by adhesions, skeletal deformities such as kyphoscoliosis and neoplasia. However, GV in a majority is secondary due to other anatomical abnormalities such as paraesophageal or diaphragmatic hernia, diaphragmatic eventration, paralysis of the phrenic nerve and anatomical abnormalities of other organs such as the spleen.5,6 The aetiology for the present case is likely to be secondary due to a diaphragmatic abnormality which was further confirmed by cross-sectional imaging finding of a hiatus hernia.
GV can be classified depending on the onset of symptoms as acute or chronic. The Borchardt’s triad is demonstrated in a majority of the patients with acute GV. They present with acute onset upper abdominal pain. The symptoms depend on the degree of gastric outlet obstruction depending on the degree of rotation. 6 Some can present with haematemesis due to repeated vomiting and mucosal ischaemia. The traction on surrounding structures causing omental ischaemia, omental avulsion and splenic rupture contribute to the pain. Dilation of the stomach with fluid will result in upper abdominal distention as in the present case. However, chronic GV can result in a subclinical presentation like in this patient with gradual onset abdominal discomfort, bloating and non-bilious vomiting. Chronic volvulus can result in low-level bleeding due to gastric ulceration and chronic anaemia. 7 However, patients with chronic volvulus can present with acute symptoms like in the present case where the onset of symptoms is over a duration of several weeks with acute worsening of the state over 3 days.
Higher suspicion is imperative when investigating these individuals due to the rare incidence. The basic laboratory investigations in this patient demonstrate hypokalaemia caused by recurrent vomiting and gastric outlet obstruction. The classic finding in an abdominal plain X-ray is a large gastric air bubble at an air-fluid level with reduced air in distal bowel loops. 8 MAGV will demonstrate two air-fluid levels in erect films. CECT of the abdomen is the best modality of imaging with the added advantage of demonstrating the abnormalities of the surrounding structures in the case of secondary volvulus. It would be shown as an abnormally positioned dilated stomach with a swirl sign which involves the stomach and the oesophagus rotating around each other in a transverse plane. 9 Air trapped in the stomach wall with free air and fluid outside the gastric wall, and lack of contrast enhancement of the gastric wall would suggest gastric necrosis and need urgent surgical intervention.
If a patient with GV presents with unstable haemodynamic, the approach to treatment should prioritize initial resuscitation with fluid and electrolytes. Those with gastric ischaemia or perforation may require broad-spectrum antibiotics on suspicion. 10 Initial management involves gastric decompression; however, the inability of decompression, gastric perforation, refractory haemodynamic instability or shock and severe sepsis warrants urgent surgery. 10 Secondary GV involves the repair of the anatomical defect, the diaphragmatic defect in the present case. This reduces the risk of future recurrences. Repair includes reduction and derotation of the stomach, gastrectomy in instances with perforation or gastric ischaemia, and gastric fixation in some patients following repair of the anatomical defect. 11 Although surgery is traditionally performed as an open procedure, laparoscopic repair is becoming an increasingly popular option due to its advantages such as its less invasive nature, shorter hospital stays, and reduced morbidity. 12
Conclusion
MAGV is a rare surgical emergency which needs a high index of suspicion due to its life-threatening nature and the significant mortality and morbidity associated. The association of underlying anatomical defects makes patients more susceptible. The definitive surgical management should be performed the earliest to minimize complications.
Footnotes
Acknowledgements
The author sincerely thanks the patient and his family members for taking part in the study.
Author contributions
P.G.N.D. and R.J. contributed to concept and design of study, acquisition of data, analysis, interpretation of data, drafting the article and final approval of the version to be published and contributed to concept and design of study, revising it critically for important intellectual content and final approval of the version to be published.
Availability of data and materials
The data used in the above analysis will be available on reasonable request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.