
Abstract
Bullous pemphigoid is an acquired autoimmune blistering dermatosis that is commonly associated with high morbidity and mortality. New-onset bullous pemphigoid following vaccinations has rarely been reported in the literature. We report two cases of new-onset bullous pemphigoid after COVID-19 vaccination followed by a brief literature review. Twenty-six cases were included in our analysis. Our cases support that new-onset bullous pemphigoid may develop following COVID-19 vaccinations. Entering a period of clinical remission before subsequent COVID-19 vaccinations in addition to close follow-up should be considered to lessen the risk of recurrences or exacerbations.
Introduction
Bullous pemphigoid is an acquired autoimmune dermatosis characterized by subepidermal bullae and pruritus. 1 It is typically defined by the presence of IgG autoantibodies and C3 complement proteins against hemidesmosomal proteins, BP 180 and BP 230, at the dermal–epidermal junction. The exact pathogenesis is not well understood but various vaccines have rarely been identified as a potential trigger. 2
This raises potential concern amid the global vaccination campaign during the current COVID-19 pandemic. Most reports of adverse cutaneous reactions to COVID-19 vaccination have been minor. 3 However, incidences of autoimmune bullous conditions, such as bullous pemphigoid, have been documented.4–15
Here, we present two cases of new-onset bullous pemphigoid secondary to COVID-19 vaccination followed by a brief literature review. We believe that this is the first report to date of new-onset bullous pemphigoid in patients who have received three doses of COVID-19 vaccine. Written informed consent was obtained for the publication of case details.
Case series
Case 1
A 50-year-old female with asthma and hypertension presented with a 3-month history of a generalized pruritic rash that began after her second dose of BNT162b2 COVID-19 vaccine. Her rash and pruritus intensified with bullae across her torso and extremities following her third COVID-19 vaccination (mRNA-1263 0.5 cc (full dose)) (Table 1). Her medications included monteleukast, rabeprazole, cetirizine, fluticasone/salmeterol, glycopyrronium bromide, ciclesonide, reslizumab infusion, amlodipine, prednisone, and hydroxyzine. Physical examination revealed pink plaques with both non-hemorrhagic and hemorrhagic bullae scattered on the extremities, neck, chin, and torso (Figure 1(a)). Mucosal involvement (oral cavity and genital region) was also noted.
Summary: patient COVID-19 vaccinations.


Case 1 – Erosions and tense non-hemorrhagic vesicles and bullae on the left thigh (a). Incisional biopsy for routine haematoxylin and eosin staining (100× magnification) with epidermal spongiosis, subepidermal clefting, and increased dermal eosinophils (b). Direct immunofluorescence studies (200× magnification) from perilesional skin demonstrate IgG (c) and C3 (d) deposition along the dermal–epidermal junction with increased intensity of C3 deposition.
Incisional biopsies were obtained for routine histopathology and direct immunofluorescence (DIF) studies. Pathology revealed spongiosis of the epidermis with perivascular lymphoeosinophilic infiltrate in the superficial dermis (Figure 1(b)). Papillary edema and subepidermal clefting with eosinophils at the dermal–epidermal junction were also present. DIF showed a linear deposition of IgG and C3 along the dermal–epidermal junction (Figure 1(c)–(d)). Findings were compatible with a diagnosis of bullous pemphigoid.
The patient was started on a short tapering course of prednisone (from 50 to 5 mg PO once daily) for 4 weeks as methotrexate (15 mg PO once weekly) was initiated. Her condition flared once her prednisone was reduced to 20 mg PO once daily. This led to an increase of her methotrexate to 25 mg PO once weekly while her prednisone was increased back to 50 mg PO once daily with a slower taper. At her 16-week follow-up appointment, she was not developing any new bullae. Her methotrexate was held at 25 mg PO once weekly and her prednisone was discontinued.
Case 2
An 82-year-old male with hypertension and hypercholesterolemia presented with a 2-month history of a pruritic rash on his right forearm and legs that developed 3 days after his second BNT162b2 COVID-19 vaccine (Table 1). Similar skin lesions developed 10 days after his first dose of BNT162b2 COVID-19 vaccination that resolved spontaneously within 2 months. Medications at the time of presentation included bisoprolol, rosuvastatin, acetylsalicylic acid (ASA), ramipril, and clopidogrel. On physical exam, non-hemorrhagic and hemorrhagic bullae were observed on the right forearm (Figure 2(a)) with smaller vesicles noted on his calves.
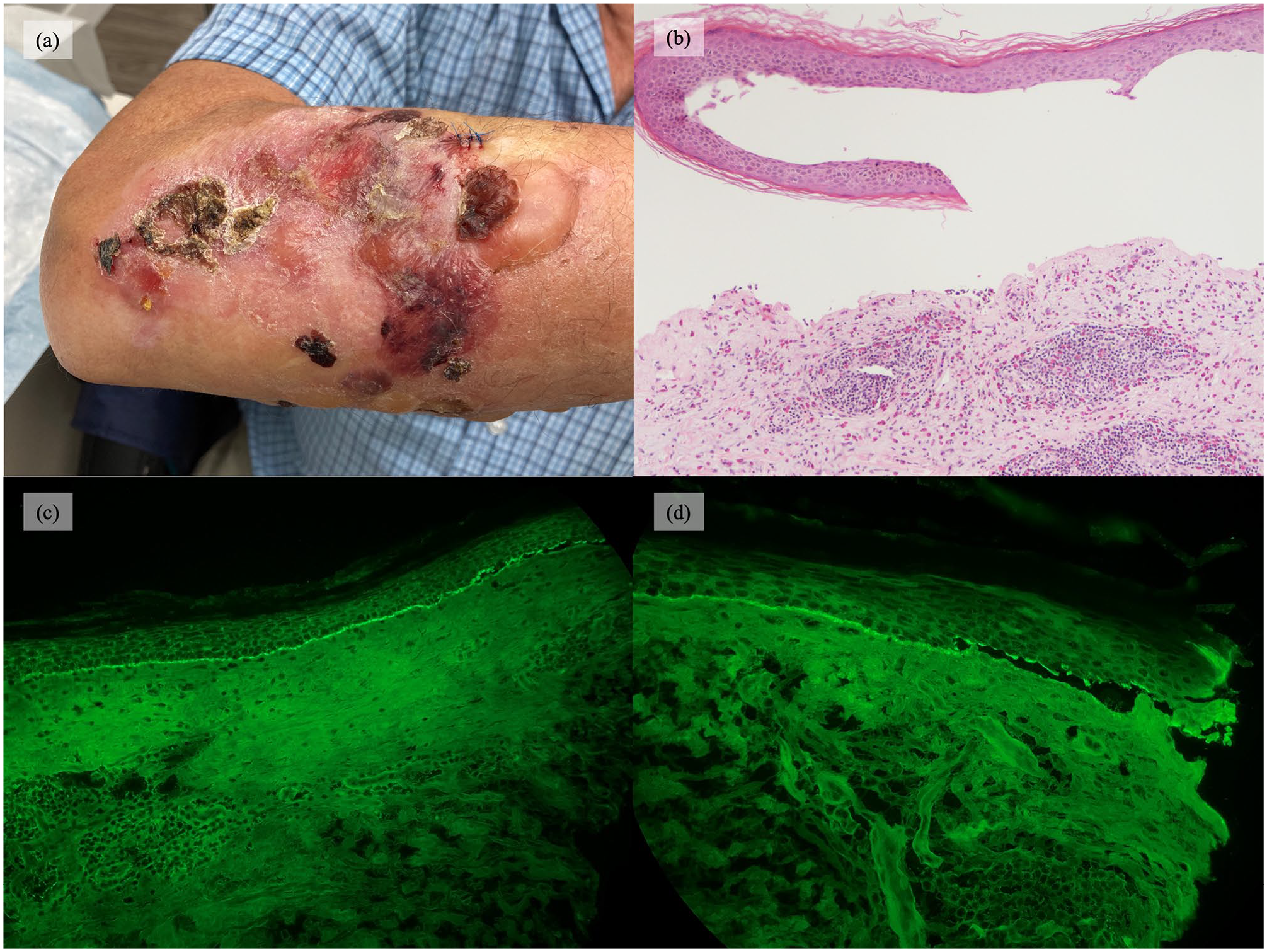
Case 2 – Erosions and hemorrhagic and non-hemorrhagic bullae on the right dorsal forearm (a). Incisional biopsy for routine haematoxylin and eosin staining (100× magnification) with subepidermal separation, papillary dermal festooning, and brisk dermal lymphoeosinophilic inflammation (b). Direct immunofluorescence studies (200× magnification) from perilesional skin demonstrate IgG (c) and C3 (d) deposition along the dermal junction with preferential staining of the roof of the epidermal split.
Incisional biopsies were completed for routine histopathology and DIF (Figure 2(b)–(d)). The biopsy revealed subepidermal separation with the vesicle filled with serous fluid and a mixed infiltrate of eosinophils, neutrophils, and small lymphocytes. Within the dermis, there was a brisk interstitial and perivascular lymphoeosinophilic infiltrate with numerous eosinophils. DIF showed a linear deposition for IgG and C3 along the dermal–epidermal junction with preferential staining of the roof of the split. Findings were consistent with bullous pemphigoid.
The patient was treated with clobetasol propionate 0.05% ointment with complete resolution after 2 weeks. The patient did not develop a recurrence of bullous pemphigoid following his third COVID-19 vaccination with mRNA-1263 0.5 cc (full dose) 4 months later.
Discussion
The exact pathogenesis of bullous pemphigoid in the context of COVID-19 vaccination is still unknown. Immune stimulation of vaccination may be an underlying factor. For example, molecular mimicry has been proposed as a potential mechanism to vaccination-induced autoimmunity. 16 However, there are currently no known basement membrane proteins that share structural similarity with SARS-CoV-2. More recently, data have been published on reactions between SARS-CoV-2 spike protein antibodies and tissue proteins transglutaminase TGase2 and TGase3. 17 Cross-reactivity between these particles has been postulated to develop into autoimmune disorders such as bullous pemphigoid. 11
A literature search was performed on Embase, MEDLINE, and Google Scholar. Search terms included variations of ‘COVID-19’, ‘vaccine’, ‘bullous pemphigoid’, and ‘bullous skin disease’. Inclusion criteria consisted of English articles that focused on human subjects published in 2019–2021. Twenty-six cases from 12 publications met our inclusion with 15 individuals4–8,10,12–15 and 8 individuals9–11,15 developing bullous pemphigoid following their first and second COVID-19 vaccinations, respectively (Table 2).
Bullous pemphigoid in association with COVID-19 vaccination – literature review.
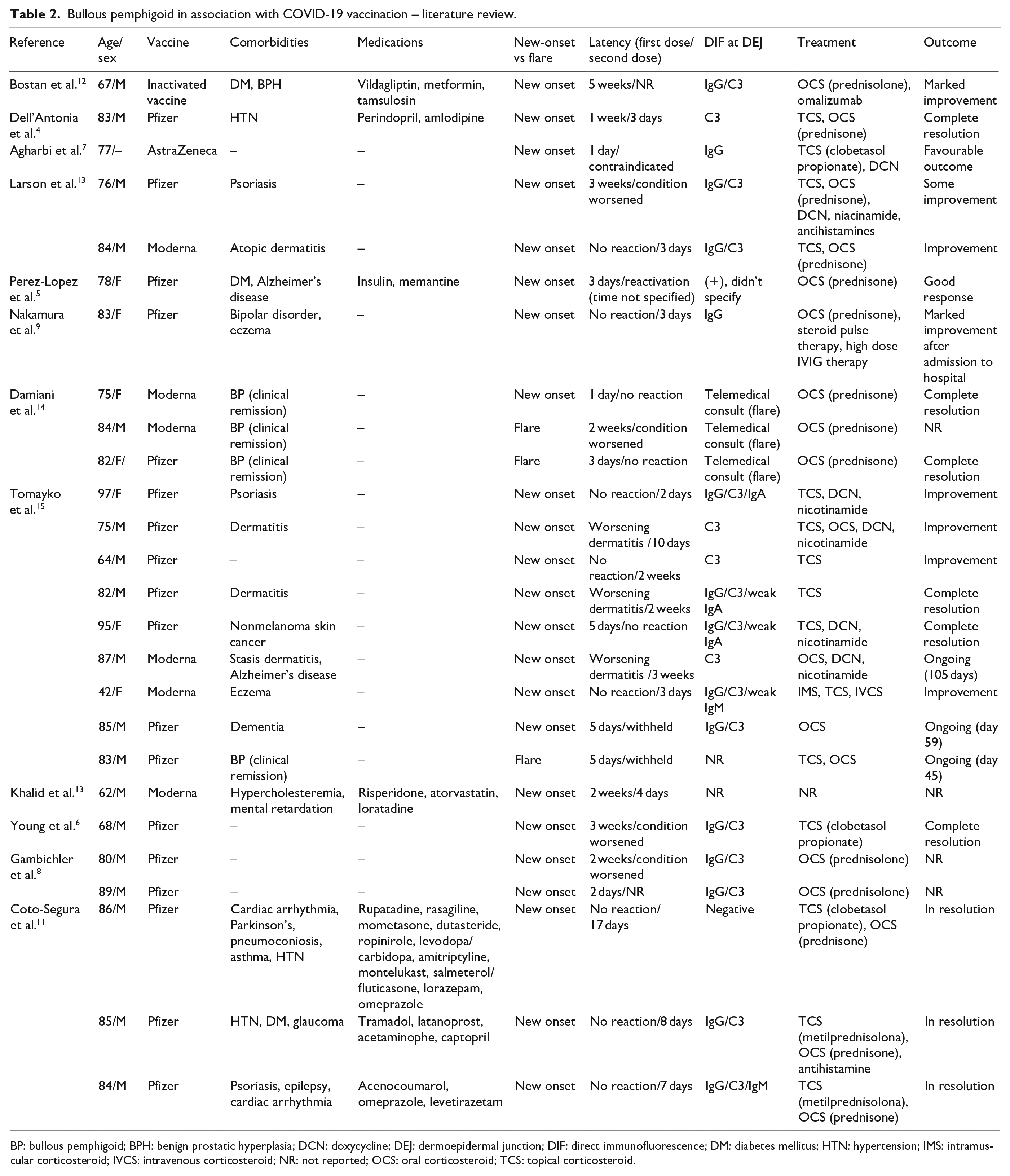
BP: bullous pemphigoid; BPH: benign prostatic hyperplasia; DCN: doxycycline; DEJ: dermoepidermal junction; DIF: direct immunofluorescence; DM: diabetes mellitus; HTN: hypertension; IMS: intramuscular corticosteroid; IVCS: intravenous corticosteroid; NR: not reported; OCS: oral corticosteroid; TCS: topical corticosteroid.
Here, we report two cases of new-onset bullous pemphigoid after COVID-19 vaccination. Consistent with other reported cases,6,8,10,14 our first case exhibited a more robust reaction after subsequent vaccination. A possible explanation for the increase in severity is that the vaccine was not administered during a period of clinical remission. Although our second patient developed a more severe reaction after his second COVID-19 vaccine, he did not develop a recurrence after his third dose. This may be explained by the different formulations that were used for his third COVID-19 vaccine (Moderna mRNA-1263) as opposed to his previous two doses (Pfizer-BioNTech BNT162b2). Alternatively, his initial milder reaction and a period of clinical remission prior to subsequent vaccination may also be reasons for the lack of recurrence following his third vaccine dose. More extensive presentations of disease have been reported to be independently associated with higher incidence of relapse. 18
Although our second case did not develop a recurrence of bullous pemphigoid when they received a different formulation of COVID-19 vaccine, our first patient developed bullous pemphigoid after receiving Pfizer-BioNTech BNT162b2 with worsening of her condition following Moderna mRNA-1263. Furthermore, there have been reports of new-onset bullous pemphigoid from both mRNA4–6,8–11,13–15 and non-mRNA COVID-19 vaccines.7,12 These findings underscore the complicated nature of bullous pemphigoid development following vaccinations and that this cutaneous adverse effect is not a phenomena of mRNA vaccines alone.
In conclusion, new-onset bullous pemphigoid may develop following COVID-19 vaccination. After ruling out other potential triggers for bullous pemphigoid, including drugs and other vaccinations, affected individuals should be monitored closely following subsequent COVID-19 vaccinations. Entering a period of clinical remission before pursuit of subsequent vaccinations should be considered to lessen the risk of a worsening cutaneous reaction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.