
Abstract
Bullous pemphigoid is a rare chronic autoimmune dermatologic blistering disease that usually affects elderly patients. Mucosal lesions are present in about 10%–35% of cases and affects most frequently the mucous membranes of the eye or the mouth. Esophageal involvement is possible but is rare (4% of cases). It could be asymptomatic, or presents with dysphagia, odynophagia, chest pain, or upper gastro-intestinal bleeding. We report the case of a recently diagnosed bullous pemphigoid in a 73-years-old female with normochromic normocytic anemia due to vitamin B12 deficiency who was referred to our unity for esophagogastroduodenoscopy. Our endoscopic examination revealed two bullae filled with blood at upper esophagus with linear ulcerations and membrane detachment upon withdrawal of the endoscope. Although bullous pemphigoid is mainly a skin disease, invasion of esophagus needs to be considered especially when symptoms are present or when no cause was found for blood loss or anemia.
Keywords
Introduction
Bullous pemphigoid (BP) is an autoimmune chronic disorder characterized by the presence of autoantibodies targeting basement membrane (BM) zone antigens, leading to the development of vesicles measuring 1–3 cm beneath the epidermis. BP can involve any area of the skin, and 10%–30% of patients have oral involvement; nasal, ocular, pharyngeal, and esophageal mucosa are rarely involved. Esophageal lesions typically do not cause symptoms but may present with dysphagia, odynophagia, or significant bleeding. The standard treatment involves administering systemic steroids, while more aggressive interventions are necessary if major organs such as the esophagus or larynx are involved, as complications can potentially be fatal in rare instances.
Case presentation
We report the case of a 73-year-old female patient with a 7-year history of dementia. She was admitted to the hospital due to a pruritic vesiculobullous rash that had been developing for 7 months. Initially, the rash was limited to the upper limbs but gradually spread to the trunk, back, and lower limbs. Upon questioning, there was no history of medication use, similar cases in the family, fever, or other associated symptoms except for chronic constipation.
During the clinical examination upon admission, the patient appeared dehydrated, with no fever, and had pale skin. Dermatological examination revealed tense bullae and erosions on urticarial plaques present on all four limbs (figure 1-2), neck, trunk, and back. Some of the lesions contained clear or serohematic fluid, while others appeared cloudy. Nikolsky’s sign 1 was negative, and no oral cavity lesions were observed.

Image of ruptured bullae in the lower limbs.

Image of ruptured bullae of the upper limbs.
The laboratory tests showed macrocytic anemia with vitamin B12 deficiency (with a level of 170 pg/ml), lymphopenia (800 elements/mm3), mild hypereosinophilia (500 elements/mm3), hypoalbuminemia (22 g/l), no electrolyte imbalances, and preserved kidney function. An osteomedullary biopsy was performed to investigate the anemia but showed no abnormalities. Viral serologies for hepatitis B, hepatitis C, and HIV were negative. Anti-BM antibodies were detected using indirect immunofluorescence with a level >1280. A skin biopsy was performed and identified subepidermal blisters with numerous eosinophils and lymphocytes. The diagnosis of BP was subsequently made.
The patient was referred to our unit for esophagogastroduodenal endoscopy to investigate her vitamin B12 deficiency anemia. The endoscopic examination did not reveal any abnormalities in the stomach, duodenum, or bulbus. However, upon removal of the endoscope, a 3 cm hiatal hernia was discovered along with grade-C esophagitis according to the Los Angeles classification. 2 In the upper two-thirds of the esophagus, two hemorrhagic bullae (figure 3-4) with linear ulcerations (figure 5) and an appearance of sloughing mucosa (figure 6) (after esophageal biopsies were taken) were observed, suggesting BP involvement of the upper digestive tract.
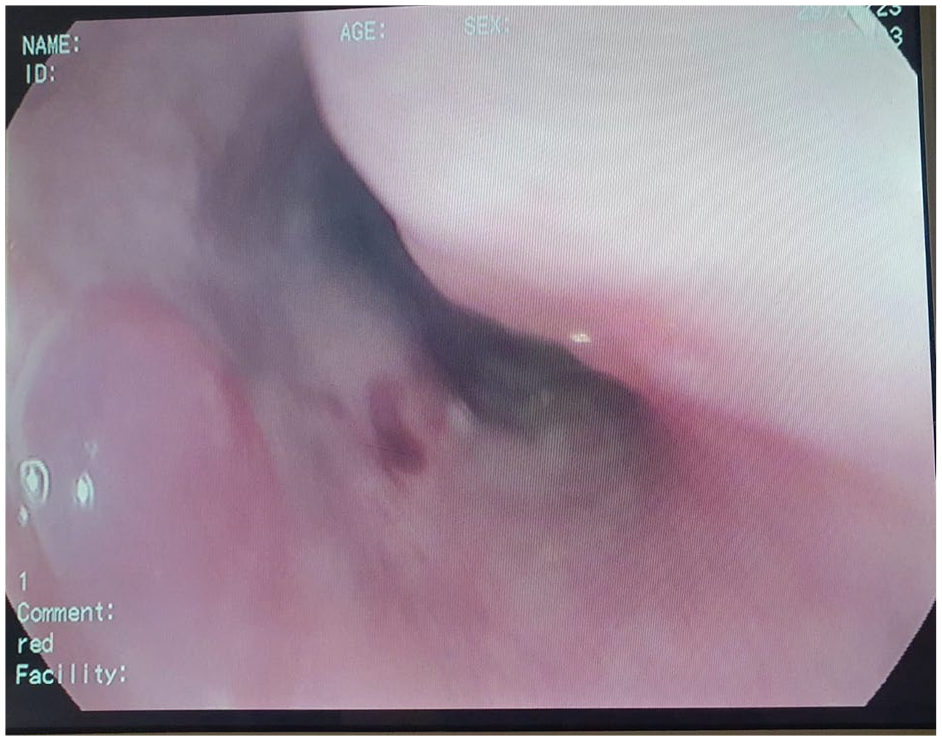
Blood blisters on the upper esophagus seen on withdrawal.

Blood blisters on the upper esophagus seen on withdrawal.

Linear ulceration of the upper third of esophagus.

Endoscopic view of mucosal sloughing after performing biopsies.
Discussion
BP is the most common autoimmune bullous skin disease, characterized by the presence of autoantibodies directed against hemidesmosomal proteins (structures connecting basal keratinocytes with the BM) of the skin and mucous membranes. 3 It affects mainly the elderly with onset usually in the late 1970s and occurs rarely in individuals younger than 50 years. 4 BP presents, usually, with a generalized pruritic bullous skin eruption and is potentially associated with significant morbidity. 3 Clinical presentation can be quite polymorphic. In the prodromal phase, nonspecific signs and symptoms can be present, dominated by pruritus alone or in association with eczematous or urticarial lesions. In the bullous stage of the disease, bullous and vesiculas lesions develop and occur mainly on erythematous skin together with urticarial papules. The blisters share same features. They affect mostly the flexural aspects of the limbs and the lower trunk and are typically tense, up to 1–4 cm in diameter, filled with clear liquid, and end in eroded and crusted areas. Oral cavity is involved in about 10%–30% of cases.4–7 Esophageal, nasal, conjunctival, pharyngeal, and anogenital mucosae are very rarely affected. The old age has been identified as the most important risk factor for the occurrence of BP,8–10 followed by neurologic and psychiatric disorders11,12 especially degenerative neurological diseases (including dementia (Alzheimer), Parkinson’s disease). Furthermore, at least 50 drugs have been suspected to be responsible for the development of BP, including analgesics, antibiotics (e.g. ciprofloxacin, amoxicillin), diuretics (e.g. spironolactone, furosemide), D-penicillamine, tumor necrosis factor inhibitors, potassium iodide, and, more recently, the antidiabetic dipeptidyl peptidase-4 inhibitors (gliptins).13,14 The association of BP with malignancies was suspected but has never been confirmed.
The diagnosis of BP is based on a combination of clinical criteria, positive direct immunofluorescence microscopy of a perilesional specimen, and the detection of specific anti-BM autoantibodies by either enzyme-linked immunosorbent assay or by indirect IF microscopy studies.
The initial assessment of patients should involve conducting a thorough physical examination, identifying potential risk factors, and, whenever feasible, evaluating the initial level of damage and the extent of BP using tools like the BP Disease Activity Index (BPDAI)15,16 or by tracking the daily blister count.17,18
Esophageal involvement in BP is extremely rare, with only a few reported cases in the literature. 19 Esophageal manifestations of BP often lack specificity, and patients may present with melena, hematemesis, dysphagia, anemia, or hemodynamic instability caused by significant upper gastrointestinal bleeding. Performing esophagogastroduodenoscopy in BP patients can be challenging due to the presence of bullae formation and mucosal sloughing, which occur even with minimal contact between the esophageal mucosa and the endoscope. To minimize complications such as hemorrhagic bullae formation, bleeding, or perforation, it is recommended to gently advance and withdraw the endoscope.
The management of BP usually varies based on the severity of the symptoms, and the treatment approach typically involves a progression from topical steroids to oral antibiotics, systemic steroids, and immunosuppression therapy. If there is significant gastrointestinal bleeding or hemodynamic instability, therapeutic endoscopy can be employed to achieve hemostasis. Treatment and follow-up in our case could unfortunately not be detailed because the patient was lost to follow-up, which may be a major limitation of our study.
Conclusion
Esophageal involvement in BP is rare but can be serious. It should be considered in all BP patients presenting with upper digestive symptoms such as dysphagia, odynophagia, upper digestive hemorrhage, or even anemia without externalized bleeding. Care must be taken while performing an esophagogastroduodenal endoscopy (EGD), with gentle insertion and withdrawal of the endoscope, to prevent mucosal injury and bullae formation.
New research and studies on BP, diagnostic methods, therapeutic means, and management of its various forms are needed to better approach these cases.
Footnotes
Acknowledgements
I would like to express my gratitude to my professors and all the colleagues who participated in the completion of this work.
Author contributions
S.Z. contributed to conception and design, collection, assembly and analysis of data, drafting of the text, sourcing and editing of clinical images; N.B. contributed to collection of data, sourcing of clinical images; M.S. contributed to data analysis and interpretation, conception and design; F.B. contributed to data analysis and interpretation; M.A. contributed to conception and design; I.S. contributed to collection of data; N.K. contributed to conception and design, supervised the preparation of the manuscript, review and editing; All authors approved the final of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Guarantor of submission
The corresponding author is the guarantor of submission.