
Abstract
Bullous pemphigoid is the most common autoimmune subepidermal blistering disease, which typically presents in the elderly. Localized bullous pemphigoid is a rare variant of bullous pemphigoid, with only about 100 cases reported up to date. In this report, we describe a 32-year-old healthy male patient with bilateral hemorrhagic bullae and erosive lesions limited to the lower extremities. A biopsy for hematoxylin and eosin stain and direct immunofluorescence established the diagnosis of bullous pemphigoid. The blistering responded well to oral and topical steroids. The exact etiology of this rare variant of bullous pemphigoid remains unknown, leading to ongoing debates and numerous suggested hypotheses.
Introduction
Bullous pemphigoid (BP) is the most common autoimmune subepidermal blistering disease, which typically presents in elderly. Its pathogenesis includes the deposition of immunoglobulin G (IgG) antibodies on the hemidesmosomes of the basement membrane. 1 BP is associated with malignancies especially in the elderly. Rarely, BP has been associated with autoimmune disorders such as inflammatory bowel disease, rheumatoid arthritis, lupus erythematosus, and so on. There has also been a significant association with neurological disorders, such as Parkinson disease, and stroke.1,2 Localized BP is very rare, with only about 100 cases reported. So here, a case of bilateral, localized BP in a young adult patient is presented.
Case
A 32-year-old male patient with no past medical or drug history presented with manipulated hemorrhagic bullae and erosive lesions with a sharply circumscribed margin on both of his lower extremities (Figure 1). The patient mentioned that he had suffered from erosive bullae in the same location 3 years ago. Upon examination, numerous tender, hemorrhagic, and erosive bullae were found limited to the right and left lower extremities—not extending beyond the ankles. The findings for the rest of the skin and mucosal sites examination were unremarkable. The workup that was done included viral and bacterial cultures to exclude any infectious etiology of the bullous lesions. Cicatricial pemphigoid, epidermolysis bullosa acquisita, pseudoepitheliomatous hyperplasia, chronic dermatitis, and lichen simplex chronicus were considered in the clinical differential diagnosis. A punch biopsy showed subepidermal bullae with eosinophils. Microscopic descriptions showed a skin tissue with separation of the denuded epidermis from the underlying dermis and mixed dermal infiltration composed of predominantly eosinophils, some lymphocytes, and neutrophils with dilated vessels and superficial fibrosis (Figure 2). Direct immunofluorescence found linear deposition of IgG antibodies in the basement membrane (Figure 3). Enzyme-linked immunosorbent assay (ELISA) for both BP230 and BP180 antibodies were negative at 10 and 1 RU/ml, respectively (normal). The patient was hospitalized and treated with oral prednisolone 50 mg daily, topical eosin 2% solution twice a day, topical mupirocin twice a day, and intravenous cefazolin 2 g three times a day leading to rapid improvement.

Bilateral erythematous plaques with hemorrhagic and erosive lesions on the lower extremities of the patient (the bright red color is due to the usage of eosin solution).
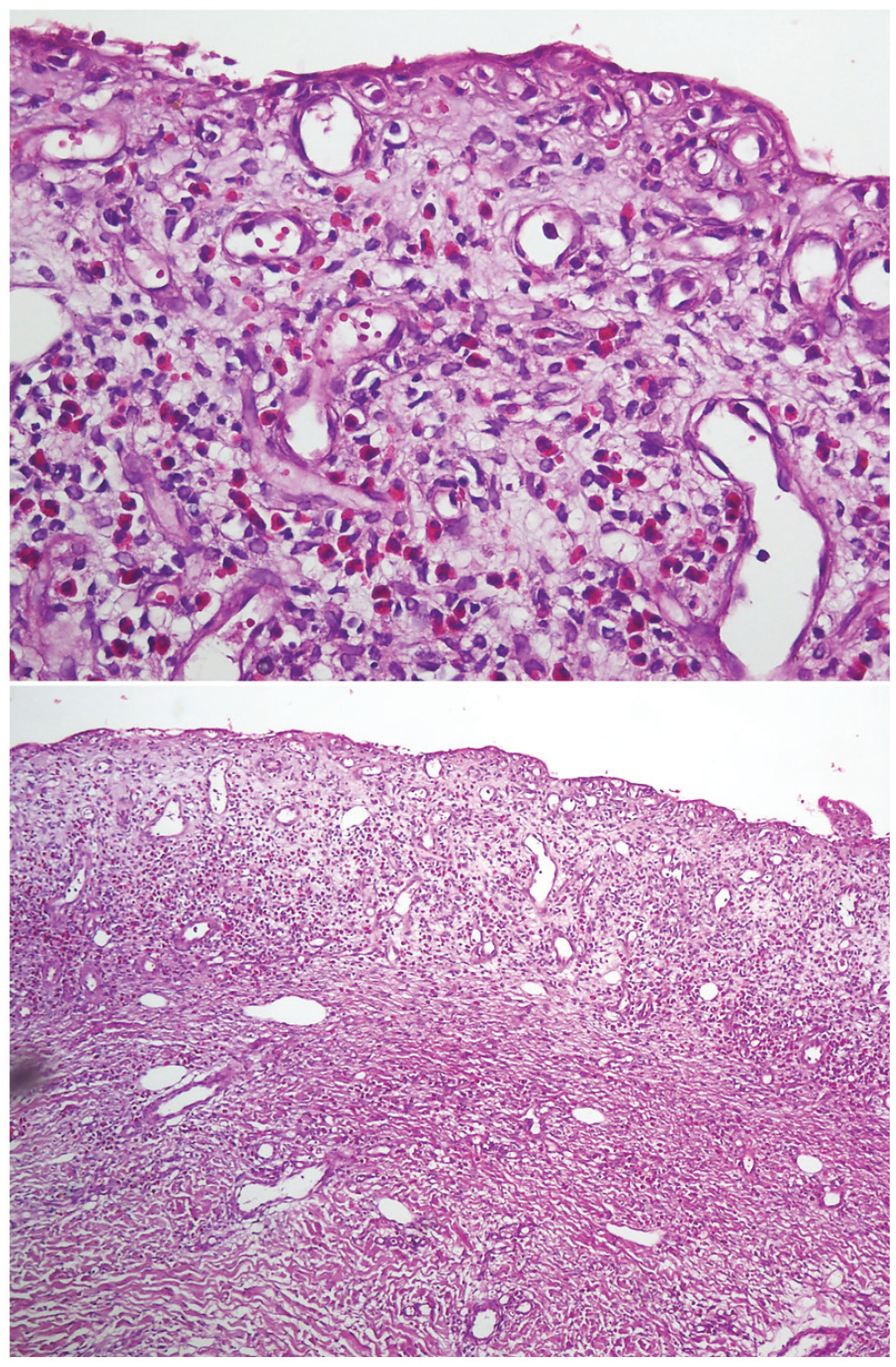
Biopsy specimen from a lesional bulla. Denuded skin without the epidermis and superficial dermal inflammatory infiltrate composed of lymphocytes and eosinophils (original magnification (a): ×40, (b): ×10).

Direct immunofluorescence of the perilesional skin showing continuous linear deposition of IgG and C3 along the dermo-epidermal junction.
Discussion
In this case, a young male patient was reported with localized BP on both lower extremities, where the results of ELISA were negative for both BP230 and BP180 antibodies. A diagnosis for BP was possible from the results of immunofluorescence having linear deposition of IgG antibodies in the basement membrane, and histopathology showing the presence of many eosinophils. In Table 1, a few case reports were summarized to compare their settings with our presented case. In the case reported by Shi et al. 3 the authors explained the cause to be related to the transient inflammatory process that takes place in locations of infection and stasis which in turn exposes the BP antigens (BPAGs). Also, Sean Dreyer et al. 4 reported a case in which they assumed that the immune dysfunction in the hemiplegic side may be causative, possibly owing to local alteration in neurotransmitter concentrations and neuropeptide balances. Truss et al. 5 related what happened to the concept of tissue damage interfering with local immune and cutaneous processes, leaving the potential for secondary disorders such as BP to develop. Tomita et al. 6 assumed that the loss of toenails with atrophic scars in their case was a symptom of localized pemphigoid because the lesions appeared only on the left foot in which the bullous disease developed.
Summary of previous case reports.

BP is an autoimmune, subepidermal blistering condition associated with immune pathological reactivity against the BP180 or BP230 hemidesmosome components of the basement membrane. 7 Localized BP is a rare subgroup, affecting 16–29% of the cases. 8 Currently, the reason why some patients develop the localized form of the disease remains ambiguous. As it can be noticed, almost all the cases reported previously had a probable inducing factor such as ultraviolet A (UVA)-light, 9 postsurgical procedures, 5 post cerebrovascular accident, 4 and venous stasis, 3 while our case occurred in a healthy young male with no previous medical or drug history, and no trauma or burn affecting his lower extremities. However, venous insufficiency which in turn can cause venous stasis and lesions on lower extremities, may be the initial culprit. The same was seen in the case report by Shi et al. where BP occurred in the setting of venous stasis. In the case reported by Tomita et al. and Truss et al., the patients probably had long periods of immobility and minimal physical activity due to their surgical operations and previous diseases. Moreover, in the case report by Sean Dreyer et al. bullous pemphigus occurred in the setting of hemiplegia, and lesions were only seen to appear on the hemiplegic side of the body in which these sides are nonfunctional and immobile.
The “Brunsting and Perry” form of localized BP was described in 1957 where lesions appeared on trauma sites (i.e., surgery scars due to amputation or colostomy, or lesions that were confined to the lower limbs without being associated with trauma 10 ). Moreover, some localized forms of traumas, which may appear insignificant, can also provoke the development of localized BP, such as the pressure of a sock elastic band. 11 Taking into consideration that our patient never mentioned any specific trauma, our case could be related to these forms of localized BP. An interesting review article published by Ruocco et al. 12 proposed the concept of immunocompromised district, in which he attempts to unify the pathogenesis of three pathological conditions (regional chronic lymphoedema, herpes-infected sites, and otherwise damaged areas). All of which can damage and immunologically mark a cutaneous region rendering it vulnerable to subsequent disorders where a secondary disease may develop after an extremely variable period of time. In this article, BP was categorized as an immunity-related disorder arising in lymphoedema, in sites of ionizing or ultraviolet radiation, burns (including sunburns), and in sites of trauma. 12 Also, more immunological tests are necessary to differentiate BP from other pemphigoid and blistering diseases such as EBA, as milia can appear both in BP and EBA according to a case reported by Tsuruta et al. 13
In addition, BP180 and BP230 antibodies were negative in most of the cases mentioned in Table 1, which is not in favor of a generalized autoimmune process as within the generalized form of BP, while in some cases3,6 only BP230 was positive. The presence of serum autoantibodies to BP230 has been shown to have an even greater association with localized BP than generalized BP. 14 This can probably imply that the localized variant has different pathophysiology than the generalized one. As for the reason behind why the localized form lacks autoantibodies against BP230 and BP180 this can be explained by the 7.8% of sera from patients with new BP reacting to regions of BP180 exclusively outside NC16A, and thus, would not be identified using currently available BP180 ELISA. 15
Follow-up is an important part of managing the disease and its complications; however, the patient in our study did not show up for the future scheduled appointments and the team lost contact with him. It was one of our limitations. Furthermore, in our department an indirect immunofluorescence salt split on specimens was unavailable.
Conclusion
As a conclusion, we can deduce that maybe immobility after hemiplegia makes the limbs prone to micro traumas and causes some sort of insufficient or decreased blood flow throughout the extremities, and venous stasis induces a local inflammatory process that, in its entity, exposes BPAGs and causes local BP lesions. Furthermore, it can be speculated that the localized form of BP is more likely to be associated with negative BP180 ELISA. To prove whether this theory is valid or not, more studies with a larger sample size are needed. Reporting similar cases is important since providing additional clues and data can be helpful to understand the etiology of localized BP.
Footnotes
Author contributions
P.N. contributed to editing, revising, and proof reading. M.A. contributed to writing the article, reviewing literature, and following up the patient. A.G. contributed to histopathology examination and reporting. A.A.P. contributed to gathering lab data, patient pictures, and pathology report. F.S. is contributed to gathering data and patient’s inform consent. M.K-F. contributed to aricle preparation and revision. All of the authors reviewed the article and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.