
Abstract
Epithelioid sarcoma is a rare soft-tissue sarcoma typically presenting itself as a subcutaneous or deep dermal mass in distal portions of the extremities of adolescents and young adults. They are frequently mistaken for ulcers, abscesses, or infected warts resistant to standard medical treatment. Patients often develop multiple local recurrences with subsequent metastases. We report a case of a 66-year-old patient with chronic leg ulcer who died of generalization of an epithelioid sarcoma.
Introduction
Epithelioid sarcoma (ES), a rare soft-tissue tumor, described by Enzinger 1 evincing an incidence of 0.02 per 100,000 in Europe 2 is divided into two clinicopathological subtypes: classic ES (or distal type) and proximal ES. Distal-type ES (DES) is a rare slow-growing soft-tissue sarcoma typically involving distal extremities of young adults, with a strong propensity for local recurrence and, ultimately, metastasis. 3 Because of its rarity (like other malignant tumors), it is often overlooked as a cause of chronic leg or foot ulcers. Most chronic leg ulcers have, of course, a vascular etiology. Venous insufficiency being the most common cause, followed by combined arterial and venous insufficiency and arterial insufficiency alone. Other causes are vasculitis, pyoderma gangrenosum, infectious diseases, calciphylaxis, drug reactions, and neoplasms. 4 The prevalence of malignancy in chronic leg ulcers in the literature ranges from 2.0% to 2.8% in retrospective analyses4,5 and from 4% to 10.4% in prospective studies.6,7 The three most common types of ulcerating skin tumors are basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and melanoma.8,9 In addition to ES, there are case reports of other rarer skin cancer types imitating chronic leg ulcers, like cutaneous lymphoma, 10 Kaposi’s sarcoma, 11 and eccrine porocarcinoma. 12 Due to the lack of consistent clinical practice guidelines on diagnostics of non-healing ulcers, initial misdiagnoses of malignant tumors could lead to a delay in appropriate management, which can contribute to worsened patients prognosis. The interval between the manifestation of malignant ulceration and the date of initial diagnosis for all tumor types was found to be 44 months, with a range of 4 to 240 months. 9
The authors describe a case report of a patient with chronic leg ischemia who died of generalization of a DES.
Case report
Our patient was a 66-year-old smoker with arterial hypertension and hypercholesterolemia. In 2002, the patient underwent an aorto-bifemoral bypass for critical leg ischemia and superficial ulcer on the right calf. For the next 14 years, the ulcer did not heal and it even expanded (Figure 1). In July 2016, angiography was performed for worsening pain in the right calf, proving occlusion of the right superficial femoral artery (Figure 2).

Ischemic ulcer on the right calf.

Computed tomography angiogram shows patent aorto-bifemoral bypass with occlusion of the right superficial femoral artery.
In October 2016, insertion of a femoro-popliteal bypass and the ablation of chronic granulation in the right calf were performed. Pseudoepitheliomatous hyperplasia was detected by microscopic examination at the edges of the ulceration. Malignant tumor structures of spindle and epithelioid-like cells were found at the base of the ulceration (Figure 3(a)), with focal necrosis and secondary vascular thrombosis. Tumor cells larger in places with centrally located nucleoli, powder chromatin, and conspicuous central nucleoli. In some places, spindle-shaped suggestive rhythmic structures in the desmoplastic stroma predominated (Figure 3(b)). In some areas of the epithelioid appearance, there were sections imitating rhabdoid structures (Figure 3(c)). Geographical necrosis and some sections of pseudogranulomatous appearance accompanied by mixed inflammatory cellulitis were detected in the tumor structures (Figure 3(d)). These areas alternated with sections of pseudoangiomatoid appearance. The number of mitoses reached 8/10 high-power fields (HPF). Grade 3 was determined using soft-tissue sarcoma grading according to French Federation of Cancer Centers Sarcoma Group (FNCLCC). Immunohistochemistry showed diffuse positivity for and cytokeratins (CK AE1-3) and early growth response protein 1 (ERG-1) whereas markers of vascular of differentiation (CD 31, CD 34) and staining on desmin were negative. With integrase interactor 1 (INI1), also known as sarcoma with retained INI1 (SMARCB1), there was no evidence of loss of expression (Figure 3(e)–(i)). Another immunohistochemical finding as cyclin D1 was diffusely positive, and BerEp4, calretinin, and HHV8 were negative.

Histopathology of the tumor. (a) Structures of spindle and epithelioid-like cells (original magnification × 100). (b) Spindle-shaped suggestive rhythmic structures in the myxoid stroma (original magnification × 400). (c) Sections imitating rhabdoid structures (original magnification × 400). (d) Sections of pseudogranulomatous appearance (original magnification × 40). (e) Expression of cytokeratins(CK AE 1-3 in tumor cells (original magnification × 40). (f) Immunoreactivity with Early Growth Response Protein (ERG-1) in tumor cells (original magnification × 200). (g) Negative staining on cluster of differentiation (CD 31) in tumor cells. Positive control in small vessels (original magnification × 100). (h) Negative staining on desmin in tumor cells (original magnification × 200). (i) Retained expression of integrase interactor 1 (INI1) in tumor cells (original magnification × 400).
Results of the molecular DNA next-generation sequencing (NGS) analysis showed only one class 4/5 (likely pathogenic or pathogenic) mutation, nonsense variant in cyclin-dependent kinase inhibitor 2A gene (CDKN2A; NM_000077.4:c.238C>T, p.(Arg80*); mutant allele frequency 42 %). 13
Copy number analysis of the DNA target regions did not reveal any homo- or heterozygous deletion or duplication (including SMARCB1 area, where homozygous deletion was detected in 87.5 % of the Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT) Epithelioid Sarcoma samples). 14 DNA did not show instability in the microsatellite areas, and tumor mutation burden (TMB) was 0 mutations per megabase. RNA NGS analysis of the 247 fusion-targeted genes did not reveal any fusion transcript as well and showed the preserved SMARCB1 expression on the mRNA level.
Subsequent computed tomography revealed a large pathological formation of 65x55 mm in the middle third of the right leg, infiltrating the skin, subcutaneous tissue, destroying the fibula and numerous satellite deposits in its close proximity—all with significantly increased accumulation of 18F-fluorodeoxyglucose (FDG) (Figure 4(a)–(d)). Enlarged lymph nodes with increased accumulation of 18F-FDG were detected in the right popliteal fossa, in the right groin, parailically, and in the retroperitoneum. Magnetic resonance imaging (MRI) of the primary tumor was not indicated since after the positron emission tomography/computed tomography (PET/CT) and biopsy, it would not have brought any more diagnostic information by that time. Performing an MRI due to the extent of the tumor (fibula destruction) + the presence of satellite foci around would not lead to any change in treatment.
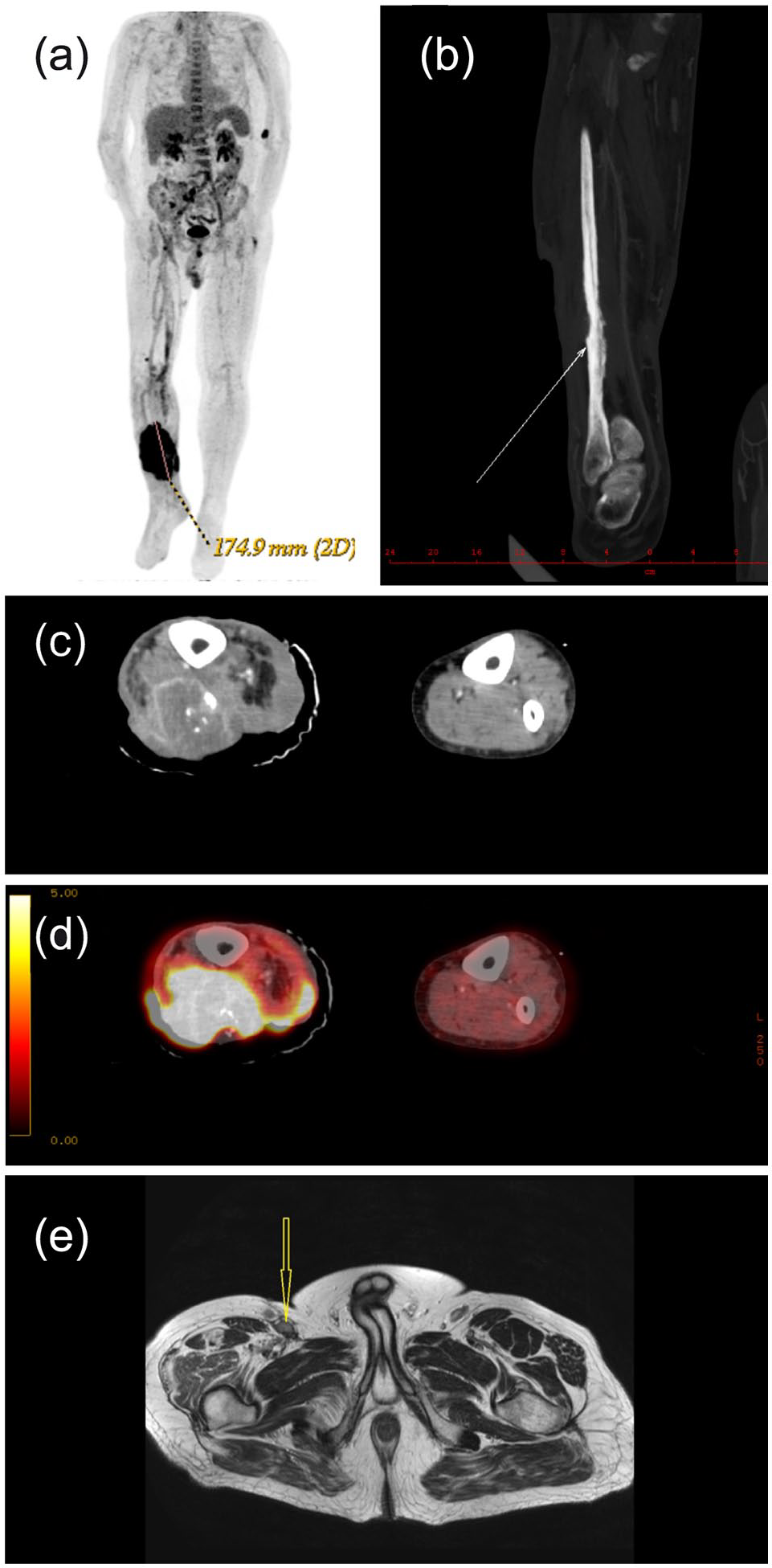
Imaging studies. (a) CT frontal image with 175 mm large black spot corresponding with tumor region. (b) CT frontal image of the right calf. The white arrow shows destruction of the fibula. (c) CT axial image of the middle third of the right calf with tumor infiltrating the skin, subcutaneous tissue, and destruction of the fibula. (d) CT axial image of the middle third of the right calf with tumor infiltrating the skin with 18F-fluorodeoxyglucose (FDG) PET/CT uptake by the tumor. (e) MRI on T2-weighted (T2W) axial image with enlarged lymph nodes in the right groin (yellow arrow).
Based on the biopsy and computed tomography findings, the patients right leg was amputated at thigh the same month. There was a skin defect in the base with granulations present in the amputate of the right lower limb. A whitish necrotic solid tumor mass with the appearance of fish meat measuring 150 mm × 55 mm × 30 mm was found in the base and edges of the defect. After right leg amputation, pelvic MRI was performed, which showed enlarged lymph nodes in the right groin and along the iliac vessels (Figure 4(e)). Chemotherapy (epirubicin first, dacarbazine, and pazopanib later) was administered repeatedly; however, the malignant cells had spread into the right lung. The patient died of pulmonary embolism within 15 months.
Discussion
DES is a rare high-grade malignancy that represents the most common primary soft-tissue sarcoma of the legs. Because of its epithelial and mesenchymal differentiation, this tumor is often mistaken for chronic inflammatory processes, necrotizing granulomas, and various fibrohistiocytic tumors. 15 Based on the morphology and the result of the immunohistochemical examination, the diagnosis of ES was determined. The tumor showed mainly structures of the classic (distal) type of sarcoma, but also pseudoangiomatous and myxoid sections, which are more frequently described in the proximal type of sarcoma. Table 1 provides an overview of the most common tumors, whose morphology can be identical.16–18 Pseudomyogenic hemangioendothelioma and epithelioid angiosarcoma are the most probable in differential diagnosis. However, both of these tumors and other vasculoendothelial tumors demonstrated a constant positivity with markers of differentiation (CD31, CD34), which is clearly negative in our case (Figure 3(g)). Furthermore, angiomatoid fibrous histiocytoma and malignant epithelioid rhabdoid tumor (MERT) may have a similar morphology within the differential dg., these tumors occur predominantly in childhood and both tumors show positivity with desmin. The tumor demonstrated by us shows negativity with desmin (Figure 3(h)). However, the distinction between aggressive malignant epithelial rhabdoid tumor and ES is not completely resolved at that time and in some places subjective. ERG1 is not directly specific for ES, but the immunophenotype ERG1+/FLI1+/D2-40+/FVIII-/CD31-/CD34- is not sufficient for the diagnosis of anogiosarcoma, including the epithelioid form either. 19 A similar epithelioid morphology occurs in malignant peripheral nerve sheath tumor (MPNST), only with diffuse expression of S100 protein subtypes. 20 Expression of S100 protein in our tumor was not present. The tumor demonstrated by us is polyphenotypic, expressing not only cytokeratin, vimentin but also vascular markers and with a relatively diverse morphology ranging from pseudoangiomatous structures to myxoid sections, but without loss of INI1 expression. The tumor originated in a terrain of long-lasting ulcer and focal chronic edema; its histological appearance could be modified due to this fact.
Comparison of immunohistochemical examinations of epithelioid sarcoma with tumors in which epithelioid morphology occurs.

++: usually; ++: often; +/−: half or less; CD31: cluster of differentiation. Platelet endothelial antigen cell adhesion molecule-1; CD34: cluster of differentiation. Human hemopoetic progenitor cell antigen; CK: cytokeratin; D2-40: podoplanin, used to show lymphatic differentiation in vascular tumors; EMA: epithelial membrane antigen; ERG: early growth response protein; FLI1: friend leukemia integration 1 transcription factor, proto-oncogene located on chromosome 11q24; FVII: factor VII related antigen; INI1: integrase interactor 1; p40: variant of a new human p53 homologue oncogene (p40/p51/p63/p73 H); S100: group of protein, cytoplasmic and nuclear marker of Schwann cells and melanocytes.
ES is a rare tumor. The morphology may overlap with a number of epithelioid-looking tumors. In > 90 % of cases, ES shows loss of INI1 / SMARCB1 expression. 21 Although loss of SMARCB1 gene expression was not demonstrated by NGS, no fusion was detected at the RNA level, which also excludes a number of diagnostically considered sarcomas. 22 Angiosarcoma was excluded by negativity in CD31, CD34, and FVIII. Undifferentiated sarcoma comes into consideration in the differential diagnosis, but pathognomonic elements were not found at the morphological level. A positive result with CKAE1-3, ERG-1, and FLI-1 and a negative result with other tests such as desmin, CD34, and CD68 do not support the diagnosis of this type of sarcoma.
Given the morphology and results of the immunohistochemical examination and NGS, we believe that this is a classic ES from a small group of <10% of tumors with preserved INI1/SMARCB1 expression. 23 The tumor like most sarcomas metastasized to the lungs after 1 year. The same epithelioid appearance and similar immunophenotype without the presence of myxoid structures were present in the metastases.
Molecular analysis of the DNA and RNA revealed nonsense variant in tumor suppressor CDKN2A gene, preserved expression of the SMARCB1 gene, which is rather rare in ES as shown by MSK-IMPACT study results and TMB = 0, which indicates very low mutation rate in analyzed lesion.
The most common administered chemotherapy regimens are single-agent anthracycline therapy or the combination of an anthracycline with ifosfamide. 24 The experience with a regimen combining gemcitabine with docetaxel is limited due to a small number of patients. 25 Recently, tazemetostat, a selective EZH2 inhibitor developed from the fact that loss of INI1 function in ES induces oncogenic dependence on transcriptional repressor EZH2, has provided a 25% objective response as a first-line treatment with few serious side effects. 26 For our patient, epirubicin chemotherapy was chosen as a drug of the first choice for the treatment of the sarcoma. For the failure of epirubicin, the next cytostatic treatment was continued by dacarbazine and pazopanib. Nevertheless, the cytostatic treatment did not prevent progression of disease.
Despite the administration of palliative chemotherapy, our patient had a poor prognosis and other patients with this generalized tumor. The reported median survival time is around 52 weeks, and the 1- and 5-year survival rates are 46% and 0%, respectively. 24 Therefore, a substantial unmet need exists to improve the medical management of ES patients by establishing novel systemic regimens and exploring novel targeted therapy.
Conclusion
The authors draw attention to the risk of developing ES in long-lasting ischemic ulcers. They point out the need to create consistent clinical practice guidelines about the diagnostics of non-healing ulcers that can contribute to improve patients prognosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Robert Holaj is supported by a project funded by Ministry of Health of the Czech Republic—DRO (General University Hospital in Prague—VFN, 00064165).
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.