
Abstract
Mycobacterium tuberculosis is one of the oldest and most studied infections, yet it remains one of the most common causes of infection-related death worldwide. The majority concern pulmonary tuberculosis. Therefore, extrapulmonary cases are rare and are often neglected in the differential diagnosis, especially in chronic musculoskeletal complaints. Nevertheless, osteoarticular manifestation of tuberculosis can cause disabling destruction of bone, cartilage, and surrounding soft tissues which may be exacerbated by a delay in diagnosis. This case report documents a case of primary osteoarticular tuberculosis causing septic arthritis of the wrist and carpus. In our case, the patient had no pulmonary burden of tuberculosis, which further delayed diagnosis and lead to irreversible damage to the wrist as well as carpus. This case illustrates the need to consider this diagnosis in at risk populations in order to prevent a delay in diagnosis and treatment.
Introduction
Mycobacterium tuberculosis has been documented as far back as ancient Egyptian times. 1 Despite advances in global healthcare and drastic decreases in disease burden in North America, this disease remains as one of the top 10 causes of death worldwide having caused 1.4 million estimated deaths in 2019. 2 In addition, 23% of the world’s population are estimated to have latent tuberculosis (TB) and are at risk of developing active disease over their lifetime. 2 Transmitted through aerosolized bacteria, M. tuberculosis infections primarily present with indolent pulmonary manifestations.2,3 Rarely, inoculation with M. tuberculosis via hematogenous spread can affect the musculoskeletal system. Previous data suggest that only 3%–5% of M. tuberculosis cases have documented musculoskeletal manifestations.2–4 Osteoarticular TB predominately involves the large weight bearing joints, with the most common site being the lumbar vertebral bodies, followed by the hips, and then knees.3,5 Osteoarticular TB involving the hand and wrist is exceedingly unusual, and a few cases have been reported in the literature.3–14 Identification of osteoarticular TB presents a diagnostic challenge given the rare occurrence, insidious onset of disease, and lack of specific clinical hallmarks. Below, we report a case of osteoarticular arthritis of the wrist caused by TB, which occurred without evidence of pulmonary manifestations.
Case report
A 31-year-old right-hand-dominant male presented to the emergency department with acute right wrist pain after lifting a box for an upcoming move. The patient was originally from Afghanistan and 7 years prior to presentation had moved to the United States. The patient was diagnosed with a right wrist ligamentous sprain and discharged from the emergency department with anti-inflammatories per patient report. The patient moved from Florida to Canada and continued to have right wrist pain. One month later, the patient presented to an emergency department in Canada with continued right wrist pain. At that visit, he was diagnosed with primary osteoarthritis, instructed to continue anti-inflammatories, follow up as an outpatient with his family provider, and was again discharged from the emergency department. The patient moved back to the United States and subsequently reported to our emergency department with continued right wrist pain for greater than 3 months and new onset fluctuance at the volar aspect of the right wrist. Laboratory tests and vital signs were obtained, as shown in Figure 1.

Admission vitals and laboratory values.
The emergency department provider obtained radiographs of the right wrist (Figure 2). X-rays revealed diffuse destruction and osteopenia of the proximal as well as distal carpal rows with scattered cystic changes of the distal radius, ulna, and carpal bones. Orthopedics was subsequently consulted for evaluation and treatment.

Initial right wrist anteroposterior (AP) radiograph demonstrating significant osteopenia and degenerative changes across the joints of the wrist and carpus.
On physical examination, there was an area of fluctuance appreciated on the volar aspect of the right wrist. It was erythematous and had developed desquamation of the skin around the lesion (Figure 3).

Clinical photograph of the right wrist from the volar side (a) and the radial side (b). Images demonstrate erythematous area of fluctuance with overlying skin desquamation.
The patient had pain with small arcs of motion of the right wrist and held his wrist in a guarded position. The patient appeared to be hyper reflexive in his upper extremities, but otherwise was neurovascularly intact about his entire right upper extremity with no other upper motor neuron signs. At this time, the differential diagnosis included infectious arthropathy of the wrist and carpus (bacterial: aggressive vs indolent, or fungal), non-infectious inflammatory arthropathy, neuropathic joint, or neoplastic process. Further testing was performed to rule out potential diagnoses in our differential.
A magnetic resonance image (MRI) with intravenous (IV) contrast was obtained to further characterize the lesion and its involvement (Figure 4). Enhancement was noted diffusely about the wrist and carpus on T2-weighted imaging with a subcutaneous fluid collection communicating with the radiocarpal joint.

T2 MRI of the right wrist demonstrating signal change in the distal radius and carpal bones (a) as well as a fluid collection (b).
The patient underwent aspiration of the right wrist. The fluid appeared grossly purulent and was sent to the lab for cytology, gram stain, culture, and crystal analysis.
Supplemental imaging obtained included a chest radiograph for concern of possible pulmonary M. tuberculosis and MRI of the cervical spine to rule out a syrinx which could have caused a neuropathic joint and accounted for his hyperreflexia. The chest radiograph was negative for any acute or indolent pulmonary disease and the MRI of the cervical spine did not show a syrinx.
Given the work-up obtained in conjunction with his history, our differential was narrowed to infectious arthropathy of the wrist and carpus likely secondary to an indolent bacteria or fungi. The patient was admitted to the hospital for septic arthritis of the wrist and carpus and was taken to the operating room for an irrigation and debridement (I&D) of his right wrist. During the I&D extensive purulent material, synovitis, severe bony erosion, and significant cartilage loss were encountered. No “rice bodies” were found. Specimens were obtained and sent to pathology for further analysis. A need for future debridement was evident and as such the patient was packed open and sent to the floor on broad spectrum IV antibiotics (vancomycin, cefepime, and metronidazole). Following the first I&D, the whole blood QuantiFERON TB gold test returned as positive and preliminary pathology showed for caseating granulomas (Figure 5). Of note, genetic analysis was not performed on the pathology specimens obtained.
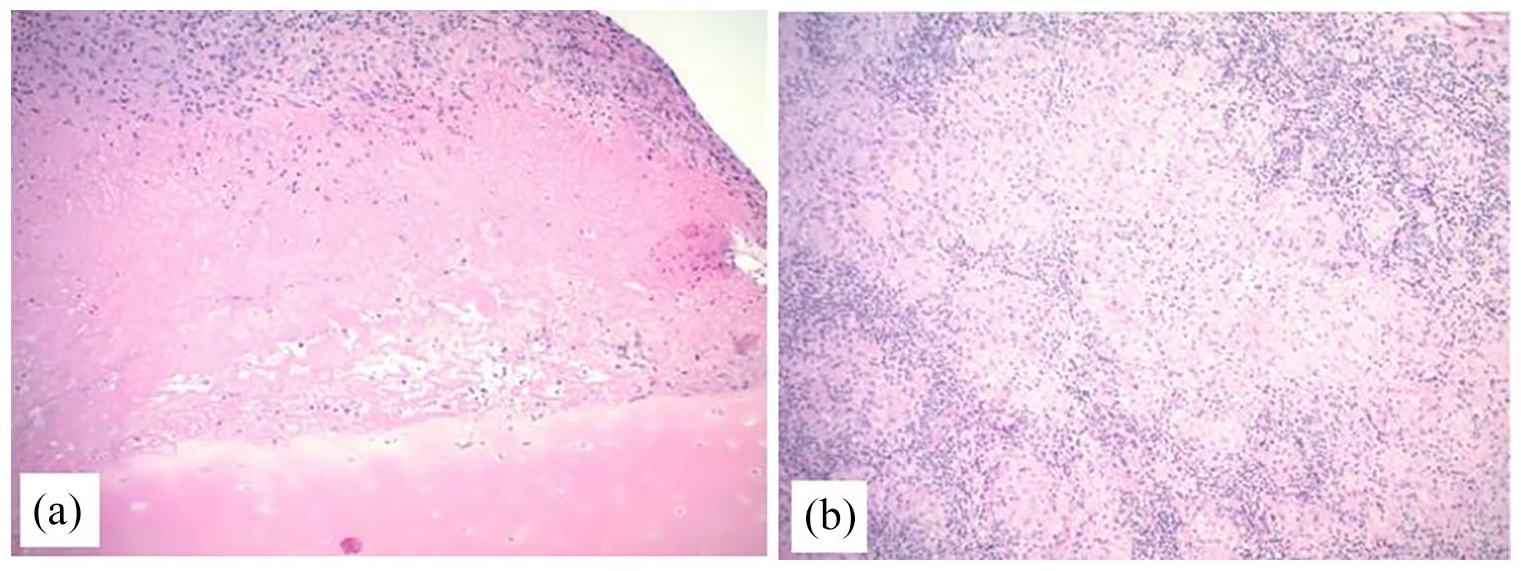
Surgical pathology (a) and (b), demonstrating caseating granulomas.
Culture and sensitivity results of the aspiration returned positive for M. tuberculosis, and the antibiotic regimen was revised to rifampin, isoniazid, pyrazinamide, and ethambutol (RIPE) per sensitivities. The patient was reported to the Department of Health for directly observed therapy per protocol. Subsequently, the patient required two more open I&Ds. At the time of the third debridement, it was felt that the infection was resolving and that there was appropriate tension on the skin to attempt partial closure. The large volar fluctuance had created a sizable soft tissue defect that was not amenable to primary closure (Figure 6).

Clinical photograph of soft tissue defect (measuring approximately 2 cm × 6 cm) following final irrigation and debridement.
The patient’s final procedure was a full-thickness skin grafting of the described defect. The graft was harvested from the proximal aspect of the patient’s right upper extremity and primarily closed. The patient continued with follow-up care as an outpatient and was seen 2 months post-operatively. The skin graft was noted to have healed well and he was continuing RIPE therapy. Radiographs obtained from that follow-up appointment demonstrated severe degeneration of the right wrist and carpus with continued osteopenia (Figure 7). He continued to have substantial pain, decreased range of motion of the right wrist, and difficulty with completing activities of daily living. Ultimately, he was lost to follow-up approximately 2 months after discharge.

Two-month follow-up radiographs demonstrating diffuse osteopenia about right wrist and hand with advanced degenerative changes.
Discussion
Primary osteoarticular TB involving the hand and wrist is rare, and a few cases have been reported in the literature (Supplemental Tables S1–S4).3–14
Anti-TB medications are the centerpiece of treatment of primary osteoarticular TB. All of the cases described in the literature, including ours, aimed to utilize antibiotics for approximately 12 months. Kumar et al. 15 discussed their use of anti-TB treatment for 18 months. Their patient presented with 1-month of left wrist pain. Radiographs of the wrist demonstrated a lytic lesion of the lunate and diagnosis was confirmed promptly with a core needle biopsy. The patient was started on RIPE therapy that was continued for 18 months which lead to complete resolution of their symptoms and consolidation of the lytic lesion within the lunate. This article demonstrates that a timely diagnosis of osteoarticular TB can be successfully treated with medical management alone. However, I&D may also be required. Prakash et al. and Visuthikos et al. described patients who improved with debridement due to the severe nature of their infections. In this case, the patient demonstrated signs of septic arthritis of the wrist with a large, painful volar fluctuance that would have been undertreated with antibiotics alone. In the face of septic arthritis of the wrist, delay of surgical debridement by as few as 8 h, even with indolent organisms can lead to further irreversible destruction of the articular surface.16,17 Wang et al. 14 provided details regarding an extensive debridement following diagnosis of musculoskeletal TB. Wang et al.’s patient had no history of TB and presented with 3 months of pain, swelling, and limited motion of the right palm and little finger. Hand X-rays demonstrated soft tissue swelling and the MRI indicated synovitis around the flexor tendons. Elevated laboratory markers and aspiration biopsy confirmed TB. A radical synovectomy was performed, and multiple rice bodies were noted around the flexor tendons. With post-operative anti-tubercular treatment (RIPE) pain and swelling completely resolved by 1-year follow-up. This case confirming that a thorough debridement when needed can also be effective in the treatment of TB.
When considering osteoarticular TB as a diagnosis, one usually focuses on medical history that would place a patient at high risk for development of this rare condition including immune compromise, ascites, chronic lymphadenopathy, and previous infection with pulmonary TB. 18 However, cases have been described involving patients with no significant medical risk factors for the development of this disease. Lopes et al. 19 presented a case of a Portuguese woman who did not have any relevant past medical history, but presented with pain and swelling of the left wrist as well as paresthesia of the fingers for several months. It was also noted that the patient had received the Bacillus Calmette–Guérin (BCG) vaccination at birth. In this case, radiographs at the time of presentation had already demonstrated lytic destruction of all the carpal bones and the distal radius. Biopsy confirmed the diagnosis of primary osteoarticular TB, and RIPE therapy was administered for 12 months. The patient continued to have functional impairment which was attributed to the advanced degeneration at the time of diagnosis. Therefore, a high index of suspicion must be kept for extrapulmonary TB in patients who are from or have visited areas of higher TB burden despite having no medical risk factors. In our case, the patient was of Afghanistan origin. Afghanistan is a country with a high disease burden of pulmonary TB, and it remains a major public health concern. 20
Following initial treatment of primary osteoarticular TB, management of the secondary sequela is important. These often include persistent pain, stiffness, osteopenia, and in certain cases severe osteoarthritis of the wrist and carpus. Soman et al. 21 described a case where despite a thorough debridement a wrist arthrodesis with adjuvant bone grafting was ultimately required secondary to bony destruction and pain. At 3-month follow-up, function had improved, albeit diminished from pre-infection baseline, and erythrocyte sedimentation rate (ESR) has normalized. This demonstrates that arthrodesis, bone grafting, and continued anti-TB medical treatment can be an effective salvage option in cases of severe symptomatic osteoarthritis as a consequence of osteoarticular TB following debridement and medical treatment. In our case, delayed diagnosis of primary osteoarticular TB resulted in irreversible damage to our patient’s wrist and carpus cartilage. As a result, he continued to suffer from pain and decreased function. While he did heal his skin graft, he continued to have significant functional deficits and pain that would have likely required a wrist arthrodesis of his dominant hand had he not been lost to follow-up.
The diagnosis in our patient was difficult given his mild trauma and lack of continuity of care. The patient’s warning signs included a country of origin with a higher TB burden, premature wrist degenerative changes including osteopenia on radiograph, delayed gradual development of erythema/calor, and pain with micromotion. Our patient, however, did not possess any of the previously described medical risk factors such as HIV, pleural effusions, or chronic lymphadenopathy. It is unclear what diagnostic work-up was performed at the outside facilities; however, if wrist septic arthritis is suspected, we recommend including an acid-fast culture in addition to standard aerobic, anaerobic, and fungal cultures especially in patients with risk factors for acquiring TB. As stated previously, there are reports of medical management alone successfully treating osteoarticular TB. However, I&D are considered the standard treatment for septic arthritis, and, as such, our authors recommend surgeons maintain a low threshold for operative intervention when a patient presents with this diagnosis. In conclusion, these reports universally emphasize the importance of time to diagnosis, antibiotics, and when necessary surgical debridement.14,15,19,21
Conclusion
It is prudent to consider a diagnosis of primary osteoarticular TB in patients with subacute presentation of continued unexplained joint pain who are indigenous or have traveled to areas with a higher TB burden. A negative chest X-ray and history of prior BCG vaccine do not preclude this diagnosis, as primary extrapulmonary cases of TB have been reported, although rare. Finally, this diagnosis must be kept within the differential regardless of medical risk factors that a patient may or may not demonstrate as a missed diagnosis can result in catastrophic outcomes as was seen in this patient.
Supplemental Material
sj-docx-1-sco-10.1177_2050313X221102004 – Supplemental material for Rare septic arthritis of the wrist and carpus primary osteoarticular manifestation of Mycobacterium tuberculosis: A case report
Supplemental material, sj-docx-1-sco-10.1177_2050313X221102004 for Rare septic arthritis of the wrist and carpus primary osteoarticular manifestation of Mycobacterium tuberculosis: A case report by Nathan R Angerett, Zhongming Chen, Joseph J Kromka, Anna E Muzio, Michael E Kahan, John V Ingari and Robert J Maurer in SAGE Open Medical Case Reports
Supplemental Material
sj-docx-2-sco-10.1177_2050313X221102004 – Supplemental material for Rare septic arthritis of the wrist and carpus primary osteoarticular manifestation of Mycobacterium tuberculosis: A case report
Supplemental material, sj-docx-2-sco-10.1177_2050313X221102004 for Rare septic arthritis of the wrist and carpus primary osteoarticular manifestation of Mycobacterium tuberculosis: A case report by Nathan R Angerett, Zhongming Chen, Joseph J Kromka, Anna E Muzio, Michael E Kahan, John V Ingari and Robert J Maurer in SAGE Open Medical Case Reports
Supplemental Material
sj-docx-3-sco-10.1177_2050313X221102004 – Supplemental material for Rare septic arthritis of the wrist and carpus primary osteoarticular manifestation of Mycobacterium tuberculosis: A case report
Supplemental material, sj-docx-3-sco-10.1177_2050313X221102004 for Rare septic arthritis of the wrist and carpus primary osteoarticular manifestation of Mycobacterium tuberculosis: A case report by Nathan R Angerett, Zhongming Chen, Joseph J Kromka, Anna E Muzio, Michael E Kahan, John V Ingari and Robert J Maurer in SAGE Open Medical Case Reports
Supplemental Material
sj-docx-4-sco-10.1177_2050313X221102004 – Supplemental material for Rare septic arthritis of the wrist and carpus primary osteoarticular manifestation of Mycobacterium tuberculosis: A case report
Supplemental material, sj-docx-4-sco-10.1177_2050313X221102004 for Rare septic arthritis of the wrist and carpus primary osteoarticular manifestation of Mycobacterium tuberculosis: A case report by Nathan R Angerett, Zhongming Chen, Joseph J Kromka, Anna E Muzio, Michael E Kahan, John V Ingari and Robert J Maurer in SAGE Open Medical Case Reports
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.