
Abstract
Tuberculosis is a leading cause of death worldwide, especially in developing countries. It can affect any site in the body and have a myriad of presentations making diagnosis challenging. Tuberculous lymphadenitis in the abdomen is rare. We present a case of a 42-year-old man who presented with non-specific abdominal symptoms and was found to have an intraabdominal abscess on computed tomography scan of the abdomen. Endoscopic ultrasound-guided aspiration was performed, and tuberculosis was confirmed. This case highlights the importance of having a high clinical suspicion of tuberculosis even with vague symptoms in tuberculosis endemic countries. This would prevent unnecessary surgery as tuberculosis is responsive to anti-tuberculosis drugs.
Introduction
Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis. Around a quarter of the world’s population is thought to be infected with TB. An estimated 10.6 million acquired the disease in 2022 with an incidence of 133 per 100,000 population. The majority of people who developed TB in 2022 were from South-East Asia (46%) with India accounting for the highest number of cases (27%). 1 The WHO estimated incidence of TB in Sri Lanka to be 62 per 100,000 population. 2 Prior to the COVID-19 pandemic, TB was the leading cause of death from a single infectious agent. 1.3 million deaths were reported globally in 2022, of which 81% were in African and South-East Asian countries with India accounting for 29% of deaths. 1 If left untreated, the case fatality from TB is approximately 70% at 10 years. 3 Therefore, it is important to identify and treat TB promptly even in sites outside the lung.
Case
A 42-year-old male with a past history of bronchial asthma presented with upper abdominal pain for 2 months associated with regurgitation of liquids and belching. In addition, he had a loss of appetite with a weight loss of 10 kg over 1 month. He complained of dark urine for 2 days. He did not complain of evening pyrexia or night sweats. He did not have a past or contact history of TB. He had received the bacille Calmette-Guérin (BCG) vaccine during childhood. He had no history of diabetes, HIV, or immunosuppressive drugs. He had no recent travel history or consumption of unpasteurised milk. He was on budesonide/formoterol metered-dose inhaler for bronchial asthma.
On examination, he was afebrile, not pale but had a tinge of icterus. The BCG scar was present, and he had no palpable lymph nodes. Abdominal examination revealed only epigastric tenderness with no palpable masses or organomegaly. Pulmonary examinations were unremarkable. His cardiovascular and nervous system examinations were normal.
His initial investigations are summarised in Table 1.
Investigations.

Urine full report was normal with no pus cells or red blood cells. Urine and blood cultures were normal. An ultrasound scan of the abdomen revealed an increased echogenic area in the epigastric region with a dilated common bile duct raising suspicions of a malignancy. Contrast-enhanced CT scan of the abdomen showed an abscess immediately anterior to the diaphragmatic cruses between the liver and stomach with the left gastric artery traversing through the lesion. There were multiple necrotic lymph nodes in the porta hepatis and portocaval region (Figure 1).
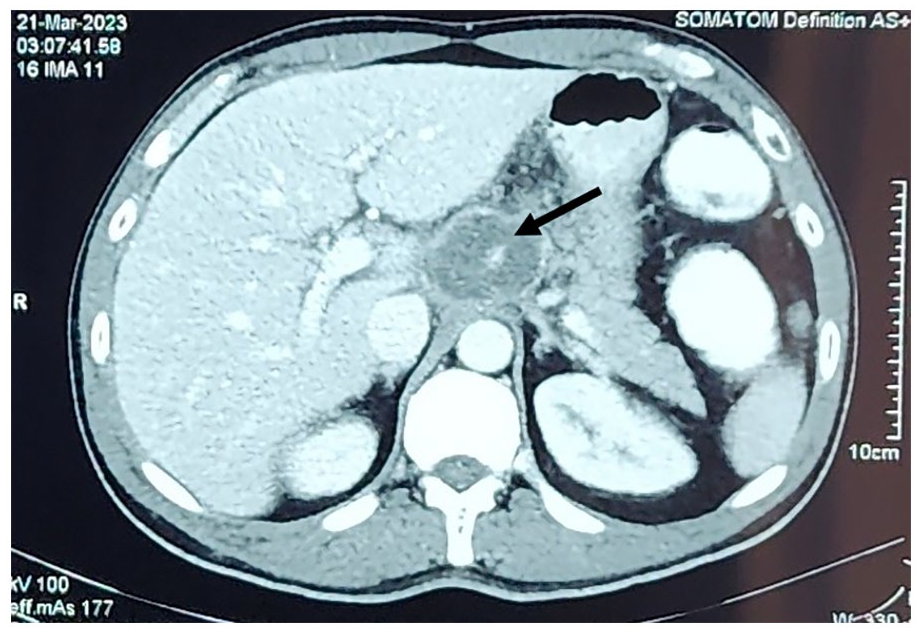
Contrast-enhanced CT scan of the abdomen.
An endoscopic ultrasound was performed which also showed a 47 mm hyperechoic mass superior to the coeliac artery encasing the left gastric artery. Very thick, blood-stained fluid was aspirated from the lesion. Gram stain and bacterial culture were normal. Acid Fast bacilli were not seen on the Ziehl-Neelsen stain. M. tuberculosis was detected from the aspirate by polymerase chain reaction (PCR) using GeneXpert Ultra MTB/RIF. Rifampicin resistance was not detected. Culture for Mycobacteria on the Löwenstein–Jensen medium was negative. Mantoux test was also positive (15 mm). Melioidosis antibodies were negative. His chest x-ray was normal.
He was started on antituberculosis therapy, namely rifampicin, isoniazid, pyrazinamide, and ethambutol for 2 months followed by rifampicin and isoniazid for a further 4 months. The patient’s symptoms responded to therapy and follow-up ultrasound scans of the abdomen in 1 month and 6 months showed resolution of the abscess.
Discussion
TB primarily affects the lungs (Pulmonary TB) but can involve any site in the body (Extrapulmonary TB). Commonly involved sites are the lymph nodes, pleura and osteoarticular areas. 4
Abdominal TB makes up 12% of extrapulmonary TB and can involve the peritoneum, lymph nodes, gastrointestinal tract or solid viscera. 5 It has a female predominance and is common in the ages of 25–45 years. 6 Patients most commonly present with ascites. Other clinical features include weight loss, weakness, abdominal mass, abdominal pain, abdominal distension, anorexia and night sweats. 5 However, isolated abdominal lymphadenitis can be the only manifestation of abdominal TB as was seen in our patient. 7 According to a case series by Sinan et al., among TB patients with abdominal lymph node involvement, 26% had mesenteric, 13% had peripancreatic/portal and 13% had para-aortic node involvement. 47.8% had diffuse lymph node involvement throughout the abdomen. 8 Such patients present with nonspecific symptoms such as abdominal pain, nausea, weight loss and fever, similar to our patient, making diagnosis difficult. 9 Furthermore, isolated coeliac lymph node TB can mimic pancreatic neoplasms, lymphoma or metastatic cancer both clinically and radiologically.9,10 TB at other sites or a contact history of TB can aid in arriving at a diagnosis but this is present in less than 30% of patients. 5 In addition, the chest x-ray shows evidence of pulmonary TB in only 10%–68.5%. 6 The chest x-ray of our patient too was normal.
Tubercle bacilli can reach the abdominal lymph nodes through ingestion, haematogenous spread or direct spread from adjacent structures. 11 The commonly involved nodes are the mesenteric root, coeliac and peripancreatic lymph nodes. 6
Ultrasonographic findings in abdominal TB are also nonspecific and include ascites, lymphadenopathy, bowel wall thickening, omental mass, focal lesions in the liver and spleen and psoas abscess. 12 Contrast-enhanced CT in intra-abdominal lymph node abscess shows a multiseptated, peripherally enhanced, hypodense mass with a regular shape and multiple, rim-enhanced, enlarged lymph nodes beside the mass. 6 Contrast-enhanced MRI can also be used to identify tuberculous lymphadenitis in the abdomen based on the anatomical distribution of the nodes and the peripheral enhancement patterns. 11 However, imaging may not be able to differentiate tuberculous coeliac lymphadenitis and abscesses from bacterial abscesses or malignancies. 9
Endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) is useful to obtain tissue for cytology and histology in addition to microbiological tests like TB PCR and culture, from sites inaccessible to other modes of tissue sampling, as in our case. 13 EUS-FNA aided us in making an early definitive diagnosis of TB in our patient. It is efficient in obtaining samples to confirm TB, especially from nodes in the coeliac axis with the diagnostic accuracy reaching 92.2%. 13 In addition to aiding in early diagnosis, EUS helps in the drainage of collections and prompt treatment of abdominal TB while avoiding unnecessary surgery.14,15
18F-FDG PET–CT imaging can be used for diagnosing abdominal lymph node TB with atypical symptoms when a biopsy is impossible. In addition, it can be used to monitor response to treatment and identify recurrence. 10 However, it is not widely available, especially in resource-limited settings as in our country.
The treatment of newly diagnosed patients with TB includes an intensive phase of 2 months with isoniazid, rifampicin, pyrazinamide and ethambutol and a continuation phase of 4 months with isoniazid and rifampicin. 16
Conclusions
Abdominal tuberculous lymph node abscesses can present with nonspecific symptoms. A high index of suspicion with the use of imaging and endoscopic ultrasound-guided aspiration of the abscess aids in prompt diagnosis and treatment. This can prevent unnecessary surgical exploration.
Footnotes
Acknowledgements
Not applicable.
Author contributions
All authors were involved in managing the patient. A.G. contributed to writing the original draft and editing. M.N. contributed to writing, reviewing, and editing. N.F. contributed to writing, reviewing, and editing. T.M. contributed to writing, reviewing, and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.