
Abstract
Melena neonatorum is not uncommon; it presents as bloody stool in newborns and is caused by ingestion of maternal blood. This case presents an infant who had multiple episodes of copious amount of blood in his stool starting at 10 min of life, which raised multiple concerns requiring further investigation. The alkali denaturation test confirmed that the blood was maternal; however, due to the amount of bloody stool and the time required for the alkali denaturation test to result, further workups such as abdominal radiograph and hemoglobin/hematocrit were completed to ensure nothing was overlooked. Our infant remained clinically stable under the newborn nursery care, and did not require a higher level of care. He was discharged with his mother at 52 Hours of Life with a follow-up appointment the next day with the Primary Care Physician.
Introduction
Causes of bloody stool in neonates can range from benign, such as swallowed maternal blood, milk protein allergies, or anal fissures,1–3 to life-threatening, such as sepsis, gastrointestinal malformations, infectious colitis, necrotizing enterocolitis (NEC), arteriovenous malformations, and thrombocytopenia.2,3 Although insufficient on their own, history and physical examination (PE) are important in distinguishing benign from life-threatening conditions. 4 Maternal blood ingestion usually occurs perinatally, and it typically presents as maroon/coffee-ground emesis, maroon-colored blood in meconium, blood-streaked stools or melena.1–4 The alkali denaturation (Apt) test 5 is the most appropriate test to determine if blood in stool is a swallowed maternal blood; however, this test is time-consuming and some hospitals do not even offer it in their labs. In these cases, the test must be sent out to another lab to perform it.
We present the case of a large amount of bloody meconium in a newborn as presentation of swallowed maternal blood, which is not well-described in the literature.
Case
This case involves a 37 weeks gestational age (GA) male newborn delivered via spontaneous vaginal delivery to a 23-year-old mother gravida 1 para 1 whose blood type is O positive, Rh positive. This was a monochorionic, diamniotic twin pregnancy with twin B fetal demise at 9 weeks GA.
Pregnancy was also complicated by adequately treated syphilis diagnosed at 21 weeks GA with an appropriate response of fourfold drop in rapid plasma reagin (RPR) titers. Antenatally, labor was complicated by adequately treated Group B streptococcus agalactiae (GBS) colonization.
The placenta had a 3-centimeter sac-like structure attached to the lateral aspect of the placenta near cord insertion, which was described as a membranous sac with viable fetal organs (pancreas, bowel, and lymphoid tissue). Considering the patient’s history, imaging studies, and histomorphology, the findings are consistent with twin reversed arterial perfusion (TRAP sequence). There were no signs of placental abruption.
Infant’s APGAR scores were 8 and 9 at minutes 1 and 5, respectively, 6 but at 10 min of life, the infant had a significant amount of grossly bloody meconium, which covered large parts of three baby-blankets.
Clinically, infant was well appearing and hemodynamically stable. Vital signs were reassuring: temperature 98.6°F, heart rate 130 per minute, blood pressure 55/30 mm Hg, oxygen saturation 99%, and weight 2890 grams. PE was normal.
Arterial cord gas: pH 7.04 and base excess −15.9 mmol/L which were consistent of in-utero acidosis. Capillary blood gas collected from the infant at 1 Hour of Life (HOL) resulted in spontaneous improvement in the acidosis: pH 7.31 and base excess −5.8 mmol/L. Hemoglobin and hematocrit (Hb & Hct) were 15 g/dL and 47%, respectively. Infant’s blood type was A positive, Rh positive with positive Coombs reactivity. Reticulocytes count was 5%.
Infant’s Early Onset Sepsis (EOS) risk was low, it was calculated using the sepsis risk calculator (SRC), 7 and he was tested positive for Treponemal Pallidum Antibodies (TPA) with non-reactive RPR.
The infant received 1 mg intramuscular vitamin K as a standard newborn care. Due to the significant amount of bright bloody meconium, abdominal radiograph was ordered and showed no obstructive gas patterns, no pneumatosis, and no concerns for volvulus.
Hb & Hct were repeated and were stable: 15.7 g/dL and 46.1%, respectively. Apt test, 5 which resulted at 12 HOL confirmed that the blood in the infant’s stool was maternal which indicates swallowed maternal blood. At 20 HOL, serum bilirubin was 9.0 mg/dL, which was a high-intermediate level per American Academy of Pediatrics (AAP), 8 and phototherapy management was indicated and initiated.
For the first 24 HOL, infant had two more large episodes of bloody meconium filling two diapers like the one shown in Figure 1, and he had no emesis. He urinated four times, and he continued to be well appearing with unchanged PE and stable vital signs. He was exclusively breastfed with good latch.
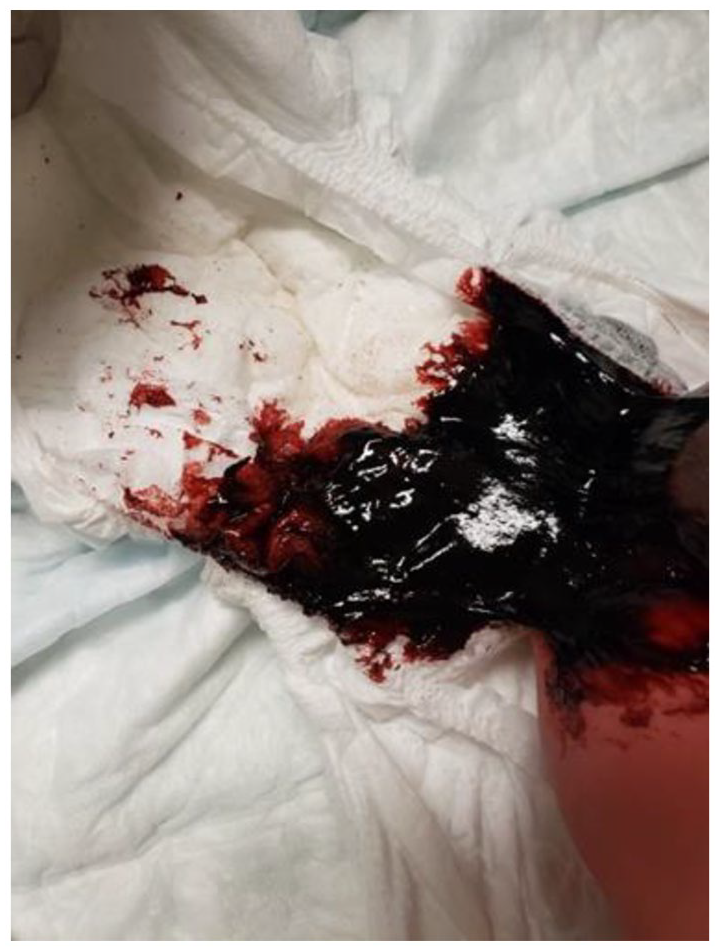
Large bloody meconium.
At 38 HOL, infant had a bowel movement consistent with melena.
Bilirubin at 52 HOL was 10.4 mg/dL which is low-intermediate level per AAP. 8 Therefore, phototherapy was discontinued and infant was discharged home in a stable condition. He had normal stool color prior to discharge from the hospital.
Discussion
We presented the case of a large amount of bloody meconium that started shortly after birth and prior to breastfeeding; therefore, milk so protein allergy and blistered maternal nipples were ruled out, also no anal fissure was visualized in the infant’s PE. Neonatal sepsis and infectious enterocolitis can also cause bloody stool in infants. 3 A positive maternal GBS, especially when accompanied with prolonged rupture of membranes (ROM), chorioamnionitis, premature GA, and inadequate GBS intrapartum antibiotics prophylaxis (IAP), increases the risk for sepsis. 7 The mother’s GBS in our case was positive; she received adequate IAP, and she did not have any associated EOS risk factors. SRC was consistent with low risk for sepsis; therefore, in addition to normal PE, an infectious process that could possibly result in gastrointestinal bleeding was less likely. Another consideration for gastrointestinal bleeding in neonates is malrotation and midgut volvulus. 3 Patients commonly present with sudden onset bilious emesis, distended abdomen, and signs of shock caused by bowel necrosis, which can be a later finding. The infant in this case had no emesis, abdominal distension, nor hemodynamic instability, in addition to negative abdominal imaging for obstruction. NEC should be considered with any bloody stool presentation.1–4,9 While NEC is typically a diagnosis of preterm infants, up to 10% of full-term infants may present with NEC.10–12 Term infants have the same presentation as premature infants: bloody stool, feeding intolerance, and abnormal abdominal exam, but, term infants typically present within the first week of life whereas preterm infants present later. 13 Although NEC can be associated with perinatal asphyxia and sepsis in term infants,5,13,14 the infant in this case was well appearing with normal exam and unremarkable abdominal radiograph. There were no concerns for perinatal asphyxia or sepsis; therefore, NEC was unlikely in this case. There were no suggestive findings of systemic coagulopathy, which may cause bloody stools.3,9 No maternal or family history of thrombocytopenia and/or coagulation disorders. PE did not reveal petechiae, ecchymosis, or hepatomegaly. Neonatal vitamin K deficiency is another common cause for hemorrhage; however, our infant received routine vitamin K injection shortly after birth. 9 While the Apt test 5 is useful in distinguishing maternal from fetal blood, limitations exist15,16; it is only useful for determining if the sampled blood is predominantly fetal (>0%) hemoglobin or maternal (<10% fetal hemoglobin). Furthermore, tarry or melena specimens can give false positive results.15,16 Modifications of the Apt test have since been made to increase the sensitivity and specificity of the test. 16 While this would be the fastest method to determine if the diagnosis for our infant is swallowed maternal blood, the test took 12 h to result. Therefore, further evaluation was warranted to rule out high risk causes.
Swallowed maternal blood was considered in our infant; however, what was concerning was the significant and frequent amount of bloody meconium that started very shortly after birth. Swallowed maternal blood is usually expected to present as black/tarry or as a small amount of bright red blood in meconium or in emesis. 9
Healthy newborns deserve to have minimal to no interventions. To accomplish this goal, more depth in neonatal conditions similar to the infant in our case should be introduced and discussed. We hope that the valuable figures in this case will provide reassurance to stop unnecessary workups for the purpose of optimal newborn outcome in the least invasive environment. Furthermore, inventing a rapid Apt test that can be obtained at bedside as a point of care would create an innovation in the neonatology world, especially when PE and vital signs are reassuring.
Conclusion
The benign melena neonatorum from swallowed maternal blood can present as massive amount of bloody meconium as early as 10 min of life. Minimal workup may suffice when the infant is stable, especially if Apt test is expedited.
Footnotes
Acknowledgements
The authors would like to acknowledge the nursing staff in our Mother-Baby Unit who were vigilant in supervising the infant in this case and saved all the belonged blankets and diapers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval/patient consent
Signed written informed consent is provided by the legally authorized representative of the infant in this case. The infant’s mother signed a written informed consent form for this case report for anonymized patient information to be published in this article. This process is sufficient in our institution for ethics approval.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.