
Abstract
Hepatocellular carcinoma is an increasingly frequent cause of cancer-related death. The majority of patients with hepatocellular carcinoma are asymptomatic. In rare cases, patients may present with symptoms of extrahepatic metastases. Early identification can lead to timely treatment and prevent poor outcomes. We report three cases of patients with hepatocellular carcinoma with unusual sites of metastasis, including clival, mandible, and cardiac involvement.
Keywords
Introduction
Liver cancer is the fifth most common cancer with hepatocellular carcinoma (HCC) being the most common type. 1 Median survival is 9–20 months. 2 The incidence of HCC has tripled since the 1980s, making it the fastest-rising cause of cancer-related death. 3 Risk factors for HCC include cirrhosis, chronic hepatitis B and C, alcohol-related liver disease, and nonalcoholic steatohepatitis.
Treatment options for HCC include surgical resection, liver transplant, transarterial chemoembolization, and radioembolization. The landscape of advanced HCC has changed recently with the approval of immunotherapy and several new first and second-line agents. The most common sites of metastasis are the lungs (55%), lymph nodes (53%), bone (28%), and adrenal gland (11%). 4 However, in rare cases, HCC can metastasize to other sites. We present three cases of HCC with unusual sites of metastasis.
Cases
Case 1
A 63-year-old woman presented for neurosurgical evaluation after endorsing dysphagia for 3 months and was found to have a skull base mass on computerized tomography (CT) of the head. Magnetic resonance imaging (MRI) of the head revealed a 5.4 cm × 2.9 cm × 3.6 cm mass in the clivus, which was deemed as the cause of dysphagia secondary to mass effect (Figure 1(a)). The patient subsequently underwent resection and biopsy of the clival mass which revealed a hepatoid carcinoma, concerning for metastatic HCC. Labs revealed alkaline phosphatase (ALP) 177 IU/ml, alanine transaminase (ALT) 49 IU/ml, aspartate transaminase (AST) 101 IU/ml, alpha-fetoprotein (AFP) of 56,344 ng/mL, CA-125 of 376 ng/mL, and normal beta-hCG (human chorionic gonadotropin), and carcinoembryonic antigen (CEA). A triple-phase CT scan of the liver revealed two LI-RADS five lesions measuring 8.6 cm × 6.9 cm, and 8.7 cm × 4.2 cm, consistent with HCC. The patient had multiple admissions for failure to thrive and opted for hospice care and passed shortly thereafter.
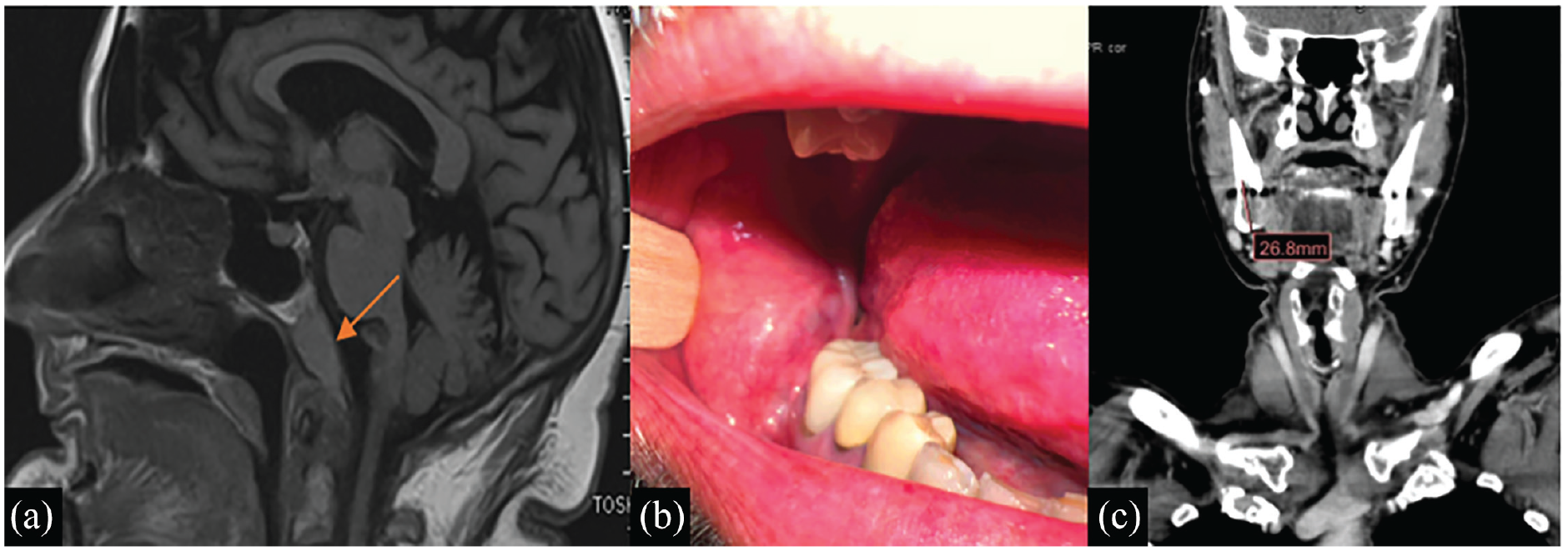
(a) Case 1: Sagittal view of magnetic resonance imaging of the brain revealing clivus mass (red arrow). (b) Case 2: Oral examination revealing a mass on the right jaw. (c) Case 2: computerized tomography of the soft tissue neck demonstrating 3.0 cm × 1.5 cm × 2.6 cm encompassing the right mandible.
Case 2
A 70-year-old man with a remote history of hepatitis C status posttreatment presented to clinic after a recent diagnosis of HCC. Labs revealed ALP 155 IU/ml, ALT 47 IU/ml, AST 39 IU/ml, and total bilirubin (T-bili) of 0.4 mg/dl. AFP was elevated at 1147 ng/ml, increased from 101.2 ng/ml 6 months prior. The patient had received two cycles of atezolizumab and bevacizumab and developed new onset severe pulsatile pain in the right jaw associated with numbness and radiation throughout the right face. Physical examination revealed a large lower buccal mass (Figure 1(b)). MRI of the abdomen revealed progression of HCC with the appearance of multiple new LI-RADS 5 hepatic lesions. A CT of the neck demonstrated a lesion involving the right angle of the mandible and adjacent soft tissue measuring 3.0 cm × 1.5 cm × 2.6 cm (Figure 1(c)). Biopsy of the mass, including immunohistochemical positivity for glypican 3 and Hep Par 1 revealed the diagnosis of HCC metastasis. The patient was referred for palliative radiation of the mandibular metastasis and is currently continuing systemic therapy.
Case 3
A 63-year-old man with a history of alcohol misuse disorder presented with jaundice, altered mental status, and coffee-ground emesis. Physical examination revealed scleral icterus, distended abdomen with shifting dullness, and 2+ lower extremity pitting edema. Labs showed a hemoglobin of 6.7 mg/dl, normal white blood cell count, platelets of 213 × 103/uL, ALT 52 IU/ml, AST 145 IU/ml, AFP 8200 ng/ml, and T-bili10.6 mg/dl. Due to concern for cardiac dysfunction in the setting of fluid overload, an echocardiogram was performed, which revealed a hypoechoic mass measuring 2.8 cm × 4.9 cm with irregular borders attached to the posterior atrial wall. Given the elevated AFP, a triphasic liver CT scan was obtained and demonstrated a 20 cm infiltrative mass with a tumor thrombus occluding both portal veins and extending into the hepatic vein, inferior vena cava (IVC), and right atrium (Figure 2(a) and (b)). Multidisciplinary discussions between surgery, oncology, and hepatology agreed on the futility of treatment, given the tumor burden and degree of hepatic dysfunction. The patient was transitioned to comfort care and discharged home with hospice.

(a) Coronal view of the computerized tomography (CT) scan showing tumor thrombus invading into the right atrium (b) Axial view of the CT scan showing tumor thrombus in the right atrium.
Discussion
Early HCC is often asymptomatic and difficult to diagnose outside of targeted surveillance programs. Advanced cases can present with extrahepatic metastases via hematogenous spread, lymphatic spread, or direct invasion of the surrounding tissue. 5 Our case series shows that in rare cases, HCC can spread to unusual sites and can be the initial presenting feature.
Central nervous system (CNS) metastases are rare, with the vertebral body and spinal epidural area being the most frequently affected. 6 Metastases to the brain comprise 0.26%–2.2% of cases, and the skull base is the most rarely affected anatomical site. 7 DeConde et al. analyzed 47 cases of metastatic clival masses mimicking clival chordoma and found that clival mass is the initial presenting sign of the primary malignancy in 36% of the cases, of which 10.6% of cases were HCC. Although lesions in the clivus commonly cause cranial nerve VI palsy, diplopia, and seizures, our patient had initial symptoms of dysphagia likely due to compression effect. Furthermore, patients with CNS or vertebral body metastasis generally have metastatic sites in lungs, lymph nodes, or bone which was not seen in our patient.
HCC can also spread to the oral cavity, which can be the initial presentation in over two-third of cases. 8 Our patient, however, developed oral metastasis of HCC after diagnosis of the primary liver lesion and two rounds of immunotherapy. A study of 10 patients by Hong et al. found oral metastasis from HCC to signify a poor prognosis. 9 In their study, 8 out of 10 patients had mandibular involvement. The predilection of metastatic deposits for bone marrow spaces and extensive blood supply may explain the mechanism for mandibular metastasis. 10
Tumor thrombus formation can be seen with HCC and signifies a poor prognosis. Most commonly, tumor thrombus extends into the portal and hepatic veins. HCC can rarely extend into IVC and the right atrium, with an incidence of 0.67%–4.1%.11–13 Some case reports have documented optimal management of HCC with extensive tumor thrombus burden by radical hepatic resection and removal of the intracardiac mass, however, many patients with HCC are poor surgical candidates due to overall functional decline.14,15 Given the rarity of primary cardiac tumors, the extrahepatic origin of cardiac masses should be considered, especially in patients with advanced liver disease.
Conclusion
Our case series emphasizes the need to diligently evaluate abnormal masses in patients with chronic liver disease, as they can signify underlying malignancy. As the incidence of HCC is rising, clinicians are likely to see unusual manifestations of HCC with increasing frequency. Given the high morbidity and mortality associated with HCC, early recognition of extrahepatic manifestations can lead to prompt diagnosis and initiation of life-saving treatment.
Footnotes
Acknowledgements
None.
Author contributions
H.C., A.S. and H.I. reviewed the literature, drafted the article, revised it for important intellectual content and were involved in the final approval of the version to be published. U.C. and M.R. revised the article for important intellectual content and were involved in the final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from patient in Case 2 for their anonymized information to be published in this article and written informed consent was obtained from patient’s legally authorized representatives in Cases 1 and 3 for their anonymized information to be published in this article.