
Abstract
We present a case of ptosis secondary to metastatic lobular carcinoma of the breast which was initially diagnosed as involutional ptosis. A 67-year-old woman previously diagnosed with lobular carcinoma of the breast presented to our clinic with mild restriction of lateral gaze and persistent droopiness of her right eyelid (associated with decreased levator function) despite recent repair of a suspected involutional ptosis. Orbital magnetic resonance imaging revealed a mass in the right orbit which was biopsied and diagnosed as lobular carcinoma of the breast. Poor levator function is rarely present in involutional ptosis. Especially in conjunction with abnormal extraocular motility, other etiologies of acquired ptosis must be considered. This case highlights the importance of patient history and ocular examination in identifying the underlying etiology of ptosis. A review of the literature to evaluate the incidence of signs and symptoms associated with metastatic breast cancer to the orbit is included.
Introduction
Breast cancer is a common source of orbital metastasis in women. 1 Orbital metastasis can present with ptosis, proptosis, periorbital edema, diplopia, among other signs. 2 Motility deficits can also be present when metastatic lesions involve the extraocular muscles, manifesting as ‘bumpy muscles’ on imaging. At times, the periocular presentation associated with an orbital metastasis may be subtle. Furthermore, the associated clinical manifestations can evolve with time; what manifests for one clinician at a given point in time may be different for the next. Herein, we present the case of a patient who presented to our clinic with persistent ptosis despite prior surgical repair for involutional ptosis. Given the history of breast cancer, ptosis manifesting with poor levator function, and restrictive lateral gaze, orbital imaging was undertaken and a neoplastic etiology was identified. With atypical cases, the patient history, clinical signs, and judicious use of orbital imaging may guide the clinician to the most likely diagnosis. 2 In addition to our case, a review of the literature evaluating the incidence of the signs and symptoms, location, and histologic features of orbital breast cancer metastasis is provided.
Case report
A 67-year-old woman diagnosed with breast cancer in 2017 was referred to our clinic for persistent right upper eyelid ptosis. She was previously treated by an ophthalmologist, who diagnosed an involutional ptosis. Upon presentation, her visual acuity (VA) was 20/200 in the right eye (OD), 20/40 with eyelid elevation, and 20/40 in the left eye (OS). There was a slight decrease in abduction OD. The margin reflex distance 1 (MRD 1) was −2 mm OD and 2 mm OS (Figure 1). The margin reflex distance 2 (MRD 2) was normal in both eyes (OU). Levator function was 2 mm OD and 10 mm OS. There was fullness in the right superior sulcus relative to left; the right superior sulcus was non-tender and firm upon palpation. The remainder of the eye examination was normal.
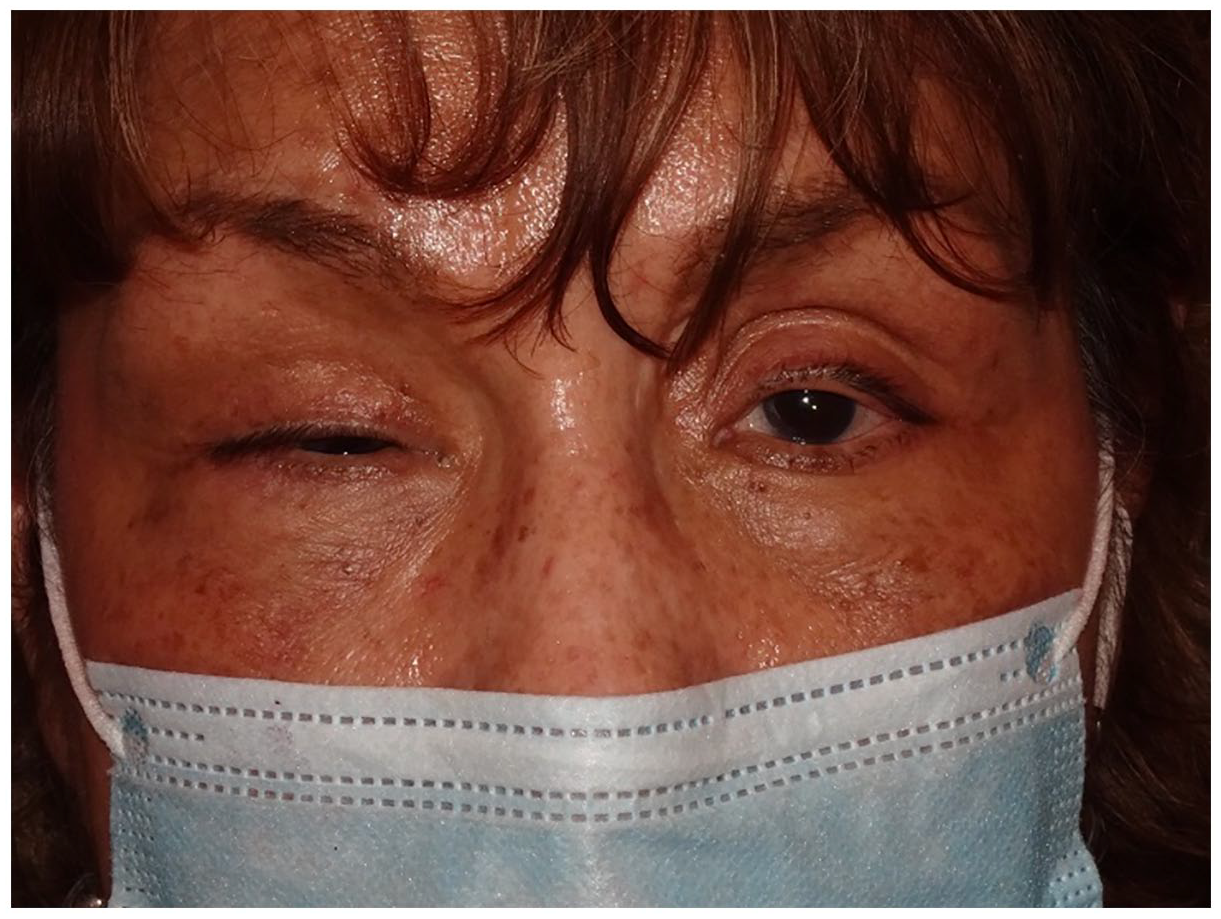
External photo demonstrating margin reflex distance 1 (MRD 1) of −2 mm in the right eye and 2 mm in the left. Note the asymmetry of the superior sulcus.
Magnetic resonance imaging (MRI) of the orbit with and without contrast demonstrated an infiltrating enhancing soft tissue mass throughout the intraconal and extraconal space with extension to the orbital apex (Figure 2). Abutment of the superior, medial, and inferior recti with associated encasement of the optic nerve was noted (Figure 2). This likely contributed to the restriction of the right eye in lateral gaze. Within a week of presentation, a right anterior orbitotomy with biopsy via a lower lid transconjunctival approach was performed. A gray-white mass was visualized intraoperatively and biopsied. The biopsy demonstrated lobular carcinoma (Figure 3). Our patient was referred to oncology and radiation therapy for further management and treatment.

Coronal T1 image demonstrating infiltrating soft tissue throughout the right orbit with abutment of the inferior, medial, and superior recti (a). Encasement of the optic nerve is demonstrated on both the coronal T1 and axial T1 images (a and b). Post-surgical changes from prior maxillary sinus surgery is present in panel a.

Hematoxylin and eosin stain (40× magnification) with immunoperoxidase stain for GATA-3, transcription factor, expressed in breast carcinoma.
Methods
A comprehensive review of the literature was performed using PubMed and Google Scholar. The search phrase ‘breast cancer metastasis to the orbit’, ‘metastatic breast cancer to orbit’, and ‘orbital metastasis from breast cancer’ identified 101 cases.3–95 Articles were researched for age, gender, and laterality of metastasis, ocular signs and symptoms, location of metastasis, and histologic features of breast cancer.
Results
A total of 101 cases and 116 eyes were identified. Increased incidence of orbital metastasis was noted in women younger than 50 years of age (n = 65, 64.4%) relative to patients older than 50 (n = 36, 35.6%). The right and left orbit were equally affected (Table 1). The most frequent symptoms experienced were blurred vision (37.9%), double vision (34.5%), eye pain (32.8%), bulging eye (16.4%), and droopy eyelid (10.3%). Ophthalmic examination most commonly demonstrated gaze deficits (50.9%), decreased VA (48.3%), exophthalmos (28.5%), ptosis (20.7%), and enophthalmos (14.7%). Orbital soft tissue was a frequent site of metastasis (47.4%), followed by extraocular muscle (43.1%), optic nerve (30.2%), orbital bone (20.1%), and lacrimal gland (3.5%). Invasive lobular carcinoma (33.7%) had the highest incidence of orbital metastasis followed by invasive ductal carcinoma (28.7%) (Table 2).
Frequency of age, gender and laterality of orbital metastasis.

15 cases were bilateral.
Frequency of signs, symptoms, location of orbital metastases, and histology of breast cancer.
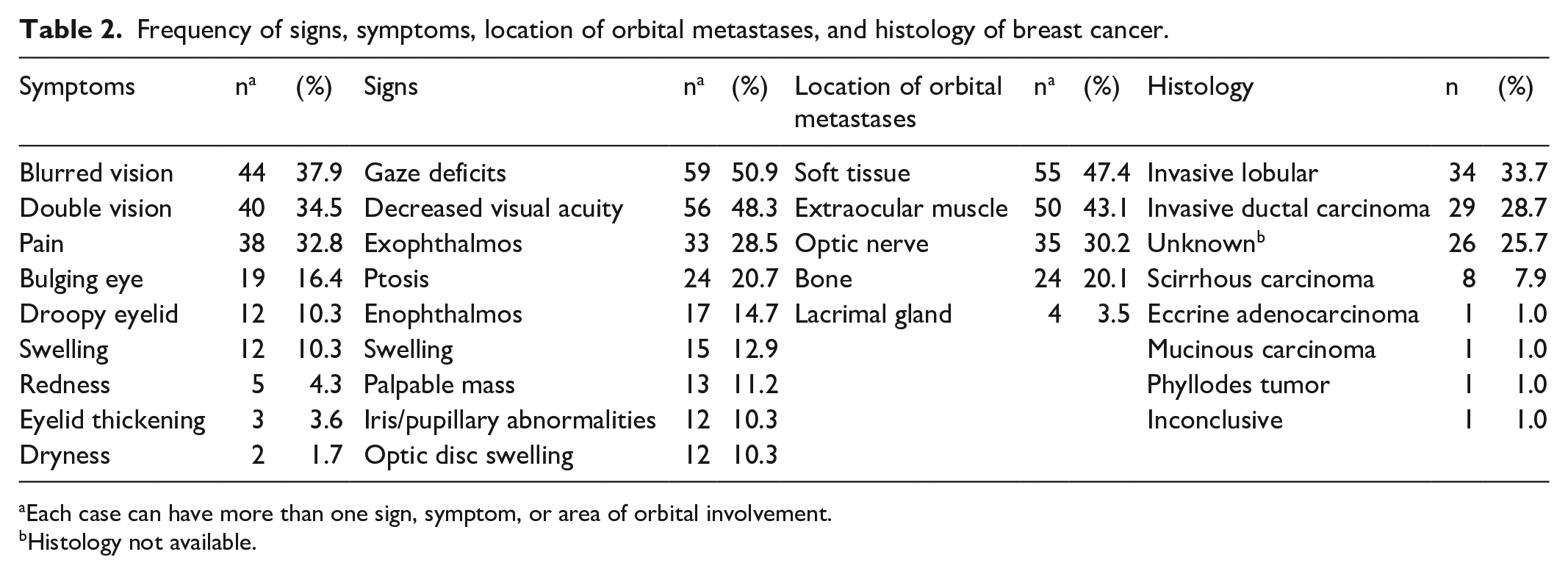
Each case can have more than one sign, symptom, or area of orbital involvement.
Histology not available.
Discussion
Routine involutional ptosis presents with normal levator function. The presence of decreased levator function as well as double vision or other newly acquired neurologic signs should alert the clinician that the patient may not have a routine involutional ptosis. A sinister and potentially life-threatening condition such as an intraorbital or intracranial tumor may exist. 96 Additionally, the patient should be queried regarding a history of thyroid eye disease, diabetes, and myasthenia gravis. These conditions can also lead to ptosis with decreased levator function.
Consistent with our review, our patient presented with complaints of a persistent droopy eyelid and was found to have abnormal extraocular movements and ptosis on examination, symptoms and signs which can frequently be seen in association with metastatic breast cancer to the orbit. Metastasis to the orbital soft tissue, extraocular muscle, and optic nerve are the most common sites of orbital metastasis from breast cancer. This is likely due to the rich blood supply these structures possess which allows for hematogenous seeding. Our patient demonstrated involvement of all three structures.
Evaluation of the orbit is best achieved with MRI which allows for enhanced visualization of soft tissues without the radiation exposure of computed tomography (CT) which provides greater bony rather than soft tissue details. 88 The MRI of this patient demonstrated the presence of an intraorbital mass. This was biopsied and diagnosed as invasive lobular carcinoma of the breast. Orbital metastasis occurs via the hematogenous route. The finding of orbital metastasis is suggestive of malignant seeding to other organs as well. A multidisciplinary team, including an oncologist, radiation oncologist, pain specialist, ophthalmologist, and ancillary services, should take a holistic approach focusing on prolonging survival and the palliation of symptoms. Hormone therapy, chemotherapy, immunotherapy, and radiation treatment are options available in the management of patients with orbital metastasis. 88
Conclusion
We present a case of acquired ptosis with poor levator function and abduction deficit associated with metastatic lobular carcinoma of the orbit. In atypical ptosis cases, a thorough history and physical examination with close follow-up is needed. MRI is the imaging modality of choice when an intraorbital and/or intracranial neoplastic process is suspected. Management requires a multidisciplinary team and approach.
Footnotes
Acknowledgements
We would like to extend our gratitude to the Highland Hospital medical librarian, Laurie Bagley, who was of great assistance to our study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the California Pacific Medical Center, San Francisco, CA.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.