
Abstract
Complex dislocation of the metacarpophalangeal joint of the index finger is rare and often requires surgical intervention. Here, we present a case of an index finger metacarpophalangeal joint dislocation requiring open reduction due to obstruction by a displaced volar plate and the intra-articular entrapment of a sesamoid bone. Surgical approach was performed dorsally, allowing easy visualization of the volar plate and sesamoid bone as well as minimizing risk to the radial digital nerve to the index finger. Postoperatively, the patient reported good functional return despite the delay in definitive management.
Introduction
Dislocation of the metacarpophalangeal (MCP) joint is a rare injury. The mechanism of this injury is typically hyperextension of the joint following a fall onto an outstretched hand. The index finger is most frequently involved, followed by the thumb. Dorsal dislocations are more frequent than volar dislocations. 1 Dislocations are considered simple if they can be reduced without open surgical procedures and complex when open reduction is necessary. Complex dislocations of the MCP joint are rare. 2
Sesamoid bones are a common finding in MCP joints. The prevalence of sesamoids in the MCP joint of the thumb is >99%.3,4 Less commonly, a single sesamoid is found in approximately 40% to 60% of index finger MCP joints with variation in prevalence between different populations and ethnic groups.3,4
We present a case of a patient who sustained an index finger MCP joint dislocation which required open reduction due to obstruction by a displaced volar plate further complicated by the entrapment of a sesamoid within the joint. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Case report
A 26-year-old previously healthy male presented to the emergency department after falling on his left index finger while playing recreational sports. Multiple attempts at closed reduction were made at an outside hospital prior to this presentation. The left index finger was swollen and tender to palpation. Radiographs demonstrated dorsal dislocation of the first MCP joint (Figure 1(a) and (b)). The dislocation was irreducible due to the operator’s subjective feeling of a “block” during manipulation. Further imaging such as computed tomography (CT) or magnetic resonance imaging (MRI) was not obtained given that several attempts at closed reduction proved unsuccessful and the decision for operative management as the best next step was made. The patient was taken to the operating room for open reduction under a supraclavicular anesthetic block. Intraoperative fluoroscopy confirmed dorsal translation of the proximal phalanx proximally to the metacarpal head (Figure 2(a)). The MCP joint was exposed via a dorsal approach, and incision and dissection revealed healthy articular surface of the proximal phalanx as well as the volar plate and the sesamoid bone, which were preventing proper closed reduction. After splitting the volar plate, the joint and the sesamoid bone were manipulated in a manner allowing reduction with gentle dorsal to volar pressure on the proximal phalanx, confirmed by fluoroscopy (Figure 2(b) and (c)). After thorough irrigation and appropriate multilayer closure, a sterile dressing and dorsal blocking splint were placed. There were no perioperative complications, and the patient went home after recovering in the postanesthesia care unit.

Radiographs obtained in the emergency department upon presentation: (a) posteroanterior view demonstrating widening of the index finger metacarpophalangeal joint and (b) lateral view demonstrating index finger metacarpophalangeal joint dorsal dislocation with small joint space opacity representing possible accessory ossicle.
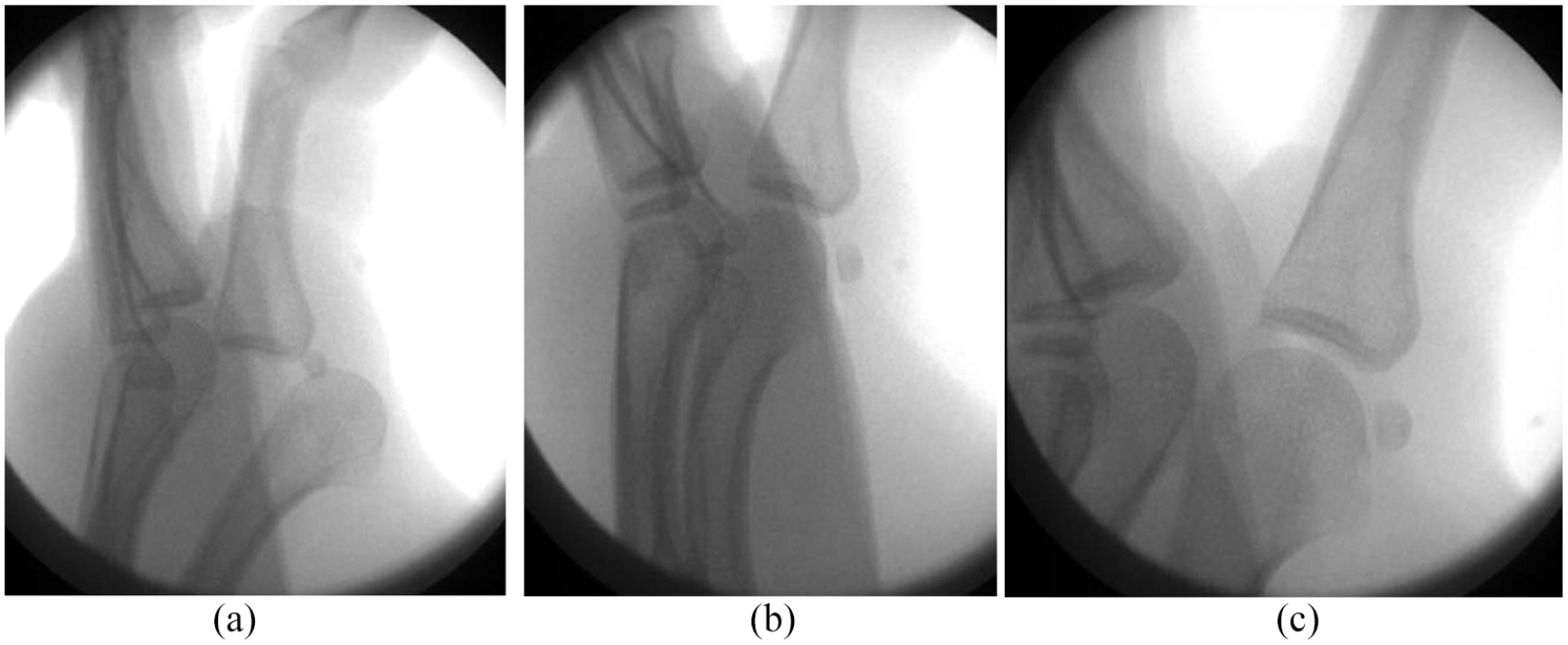
Intraoperative fluoroscopy: (a) prereduction lateral view, (b) postreduction lateral view, and (c) close up lateral image highlighting presence of sesamoid bone within the joint.
On postoperative day 5, the patient had no complaints and radiographs demonstrated maintained reduction of the left index MCP joint (Figure 3(a) and (b)). He began occupational hand therapy at that time. The postoperative splint was removed and replaced with a custom dorsal blocking orthotic with slight MCP joint flexion. The patient underwent education and demonstration with subsequent understanding of clinically appropriate composite digital flexion and extension exercises to continue at home with the goal to return to his prior level of function. He returned to clinic on postoperative day 19 for suture removal and continued hand therapy. He was doing well with no sensory deficits and was able to form a loose composite fist and extend his fingers to neutral (Figure 4(a) and (b)). He was instructed by the hand therapist to continue the home exercise program and maintain the splint ad lib in order to prevent joint and soft tissue contractures and skin breakdown. The patient returned to clinic 1 month later and the joint was well aligned; he was discharged with instructions to bear weight as tolerated while continuing the home therapy regimen to optimize range of motion and strength.

Radiographs obtained on postoperative day 5: (a) posteroanterior view demonstrating return to normal metacarpophalangeal joint space (blue arrow) after reduction as well as minimal lateral deformity of the metacarpal head possibly reflecting associated fracture (yellow arrow) and (b) lateral view.

Physical examination on postoperative day 19: (a) loose composite fist and (b) extension with minimal extensor lag.
Discussion
We present a case of a patient who sustained a complex MCP joint dislocation of the index finger that was successfully reduced via open reduction after four prior closed reduction attempts were hindered by an intra-articular sesamoid bone.
Multiple structures can interfere with the reduction of complex MCP joint dislocations, particularly the volar plate and typically through dorsal displacement into the MCP joint.1,2,5,6 Hyperextension of the finger during injury leads to avulsion of the volar plate from the metacarpal neck. This occurs at the weakest point of the attachment, where the proximal membranous portion of the volar plate attaches to the metacarpal metaphysis and periosteum. While the metacarpal head displaces toward the palm, the volar plate attached to the proximal phalanx displaces into the MCP joint. The interposed volar plate, which is held in place by deep transverse metacarpal ligaments, prevents reduction. 7
This can be further complicated by the entrapment of a sesamoid bone within the joint. The prevalence of a single sesamoid in the index finger MCP joint is a relatively common finding.3,4,8 However, entrapment of a sesamoid in a dislocated index MCP joint is rare and can further complicate an already difficult reduction. 9 There have been few prior studies reporting index finger MCP dislocation complicated by sesamoid entrapment; in all cases, open reduction was required.7–11 An early study considered the presence of a sesamoid in the joint in preoperative radiographs to be a pathognomonic sign of entrapment of the volar plate and therefore a sign of irreducibility. 8 Joint space widening is also indicative of an interposed volar plate. 1
Prior work has suggested that intra-articular sesamoid entrapment may make extraction of the volar plate challenging via the palmar approach. 7 In our case, the dorsal approach allowed easy access to the involved joint as well as visualization of the volar plate and sesamoid within the joint capsule. Aside from the extensor tendon, which may be easily visualized and protected during a meticulous dissection, there are no vital structures such as vessels or nerves dorsally. A dorsal approach both avoids injury to such structures and allows for easy access to the involved structures surrounding the joint. A subsequent longitudinal incision in the middle of the volar plate allowed the metacarpal head and sesamoid to be easily relocated, supporting prior applications of this technique. 1
Conclusion
In cases of MCP joint dislocation, recognition of radiographic signs indicating volar plate and sesamoid entrapment can indicate that open reduction may be necessary to restore joint anatomy. Our case report demonstrates that with proper surgical management, patients can have good functional and anatomic results even with delay to treatment. Routine evaluation for sesamoid bones within the joint space in the clinical context of an MCP joint dislocation could prevent unnecessary closed reduction attempts and expedite surgical intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.