
Abstract
Arthroscopic surgery is a standard technique for removal of loose bodies in large joints. By contrast, there were a few reports of arthroscopic surgery for loose bodies in small joints. We herein report a case of a 70-year-old woman with an inextensible metacarpophalangeal joint in the right middle finger due to an intra-articular loose body that developed after osteoarthritis. Surgery proceeded under vertical traction using traction tower. Two portals were developed at dorsal aspect on the metacarpophalangeal joints. The loose body was removed under arthroscopy with a small incision of both skin and sagittal band, thereby resolving clinical symptoms, including pain and limitations to metacarpophalangeal joint motion.
Introduction
Osteoarthritis in the proximal interphalangeal (PIP) joint or distal interphalangeal (DIP) joint is commonly known as Heberden’s node or Bouchard’s node, respectively. Conversely, osteoarthritis of the metacarpophalangeal (MCP) joint is relatively rare.1–3 Radiographic characteristics of this condition include the presence of osteophytes, subchondral sclerosis, and joint-space narrowing. The first line of treatment consists of conservative therapy, such as activity modification, oral anti-inflammatory medication, and intra-articular injection of corticosteroid, with result in sufficient improvement in most of patients. When these conservative therapies fail to provide pain relief, surgical intervention is considered, including arthrodesis and arthroplasty with implants,3,4 especially for severe condition on imaging study.
Furthermore, intra-articular loose bodies originate from degenerative osteoarthritis as well as the other disorders including osteochondral fracture, osteochondritis dissecans, and synovial chondromatosis. 5 The loose bodies could cause serious symptoms including pain and inability of joint motion, regardless of mild condition on imaging studies without large osteophyte and narrowing of joint-space. Arthroscopy is a useful tool for resection of the loose body with small incision. In fact, the intra-articular loose bodies were reported to be effectively treated using arthroscopy in the large joints.6–8 By contrast, there were few reports of symptomatic loose body in finger MCP joints.9,10 Finger joints could have been also treated with arthroscopy for loose body, although there was no report regarding arthroscopic removal of loose body in finger joint.
In this report, we describe a patient who underwent minimally invasive surgery using an arthroscope to treat the inextensible condition at the MCP joint of the middle finger due to a loose body growing during follow-up.
Case report
A 70-year-old woman was referred to our hospital because of complaints of pain in the MCP joint of her right middle finger over the course of the preceding year. She did not have a history of trauma, infection, or rheumatologic conditions by blood examination in which rheumatoid factor and anti-citrullinated cyclic peptide/protein antibody were 4 IU/mL and < 4.5 U/m, respectively, except for release of the tendon sheath of her middle finger due to stenosing tenosynovitis 30 years prior. Radiography of the right hand during the initial visit indicated osteoarthritis of the MCP joint of the middle finger with a slight narrowing of the joint-space and the presence of small osteophytes in both the basal phalanx and metacarpal bones; however, pathological findings were also remarkable in the index finger DIP joint (Figure 1(a)). Due to a mild complaint (DASH score, 8),11,12 the patient received anti-inflammatory drug, resulting in pain relief. Unfortunately, pain and discomfort of daily activities were worsened, with the patient receiving a 73/100 mm on the visual analogue scale (VAS) for pain and a DASH score of 49.1 at 3 years after her first visit. Upon physical examination, we observed swelling in the dorso-ulnar side of MCP joint, and a range of motion (ROM) at the MCP joint that was limited to 20–85 degrees and was inextensible. Furthermore, radiography indicated a bone tip from the ulnar side to the middle finger MCP joint and a growing osteophyte on the ulnar metacarpal head (Figure 1(c)). Radiography at 3 years after her first visit showed the presence of a small bone tip on the ulnar side of the metacarpal head (Figure 1(b)). The findings upon computed tomography (CT) and magnetic resonance imaging (MRI) also suggested that the bone tip was an intra-articular loose body, which produced the inextensible condition of her middle finger. Since the size of the loose body was large for the finger joint, we planned surgical resection under the arthroscopy. Surgery was performed under brachial plexus block and a pneumatic tourniquet was applied to the upper arm to control bleeding. The patient was placed in a supine position with her shoulder abducted and her elbow flexed to 90 degrees. A single Chinese finger trap was attached to the affected finger to apply 5 lb of longitudinal traction using a traction tower. Under the vertical traction, the MCP joint could be easily palpated and injected. Two portals were marked at radial and ulnar side to the extensor tendon. The distance between each portal and tendon was about 8 mm. A short blunt trocar and cannula system were inserted into the joint under steady gentle pressure after distension of the joint with saline and the introduction of an arthroscope with a 1.9-mm diameter (ConMed Linvatec, Largo, FL, USA) through the radial portal of the third MCP joint. Visualization was achieved and synovectomy was performed using a 2.0-mm full-radius motorized shave through the ulnar portal on the MCP joint. This maneuver allowed us to visualize and remove the loose body within the joint (Figure 2), although the origin was not apparent. Radiography after surgery indicated the disappearance of the loose body (Figure 1(d)). Postoperatively, motion was permitted without immobilization the next day after surgery, while limitations in the motion of the MCP joint soon disappeared. The motion of the MCP joint of her middle finger was able to be actively and passively hyperextended to 15 and 40 degrees, respectively, without pain at 3 years after the surgery.
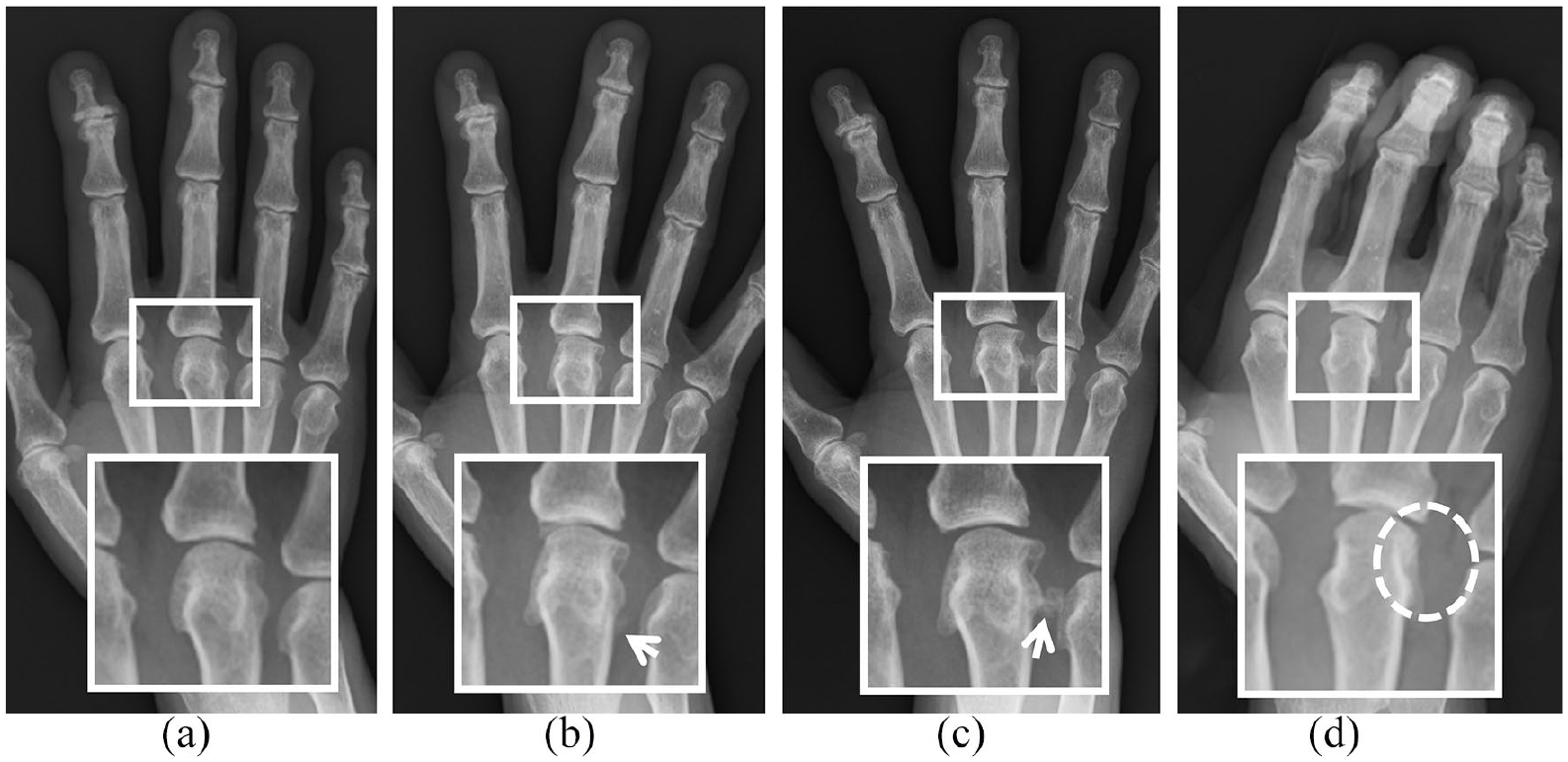
Radiographic findings. Mild osteophytes were found on the ulnar side of the basal phalanx and metacarpal head of the right middle finger during the initial visit (a). Although conservative therapy was effective, there were larger osteophytes and a small loose body (white arrow) at 3 years before surgery (b). An intra-articular loose body (c) was also observed within the inextensible metacarpophalangeal joint of the right middle finger and were removed under arthroscopy (d).

Arthroscopic findings showed a loose body (*) in the ulnar and dorsal side within the metacarpophalangeal joint.
Discussion
Hand osteoarthritis commonly affects the DIP and PIP joints of the finger and the carpometacarpal joint of the thumb. 13 In contrast, there is limited experience of patients with complaint and the surgical treatment due to osteoarthritis in the MCP joint. Only if the conservative therapy failed would surgical intervention, including open joint debridement, arthrodesis, or arthroplasty, be indicated.3,4 The patient in this case also complained of mild symptoms, which were treated with anti-inflammatory drugs during the initial visit, despite clear radiographic findings of osteoarthritis. Indeed, conservative treatment was effective in relieving pain and maintaining daily activity.
A locked MCP joint in the finger is occasionally encountered during the daily practice of hand surgeons. It is well-known that most cases of a locked MCP joint in relation with the osteoarthritis are caused by the catching by osteophytes on the anterolateral aspect of the metacarpal head.8,14 Therefore, we hesitated over preoperatively diagnosing the inextensible MCP joint since preoperative imaging studies exhibited both a large volar osteophyte and a loose body. We informed the patient and her family of the possible need of future surgery to treat the large volar osteophyte, despite symptom resolution following removal of the loose body.
Intra-articular loose bodies are frequently found in large joints, including the elbow and knee joints,6,15 and usually are caused by osteochondral fracture, osteochondritis dissecans, and degenerative osteoarthritis. It is well-known that loose bodies can be removed under arthroscopy to improve patient satisfaction. To our knowledge, this case is the first case to use arthroscopic surgery to remove a loose body on the finger MCP joint. Arthroscopic surgery may minimally injure the sagittal band with the small incisions, which would otherwise be incised during open surgery. Consequently, there was no immobilization or limitation of hand use for daily activities from the early period after the surgery in this patient. Arthroscopy is likely to be useful for removing loose bodies in the small joints, such as the finger MCP joins, as well as the large joint.
Conclusion
We report a case of an inextensible MCP joint of the middle finger due to a loose body caused by osteoarthritis. Arthroscopic removal of the loose body relieved the symptoms in this patient.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.