
Abstract
Flexor tenosynovitis is rare in young children. This case report describes that of a 10-year-old boy with diffuse swelling of the left index finger, pain when catching a ball, and progressive inability for full flexing of the finger 2 months after starting baseball play. Magnetic resonance imaging showed a defined lesion with iso-signal intensity to muscle on T1-weighted imaging, and with high signal intensity to muscle on T2-weighted imaging. It was enhanced in T1-weighted fat suppression imaging with gadolinium enhancement. Surgical excision relieved the symptom. Histopathological findings mainly indicated proliferation of synoviocytes and plasma cell and lymphocyte infiltration. We speculated that the physical impact of the ball on the left index finger of his gloved hand during catching activated some immunological mechanism and thereby caused nonspecific tenosynovitis in this young baseball player. Awareness of this pathophysiology might raise confidence in proper diagnosis for assessing the swelling of fingers in young baseball players.
Introduction
Flexor tenosynovitis of the hand is a common inflammatory condition. Most cases of flexor tenosynovitis result from infection of the flexor tendon sheath, 1 chronic irritation from overuse, 2 diabetes, 3 and collagen diseases such as rheumatoid arthritis 4 and crystalline arthropathies. 5 Proliferative flexor tenosynovitis causes diffuse swelling of the fingers, increased bulk of synovial tissue, and consequent limitation of the active joint range of motion occurring by the restriction of tendon motion. Although flexor tenosynovitis is apparently a common pathological condition in adults, it is rare in young children. Gloved hands of baseball players are exposed repeatedly to potentially destructive loads with each swing of a bat or impact of a ball into a glove.6,7 We describe the case of a 10-year-old boy with proliferative flexor tenosynovitis of the left index finger 2 months after starting to play baseball.
Case report
A 10-year-old right-hand-dominant baseball player presented with gradual swelling and worsening pain of the left index finger when catching a ball. After the symptom onset at 2 months after starting to play baseball, the boy noted progressive inability for full flexing of the left index finger. Before onset of the index finger symptom, he had experienced no trauma history. Moreover, he had no history of collagen disease such as juvenile idiopathic arthritis (JIA). He and his parents consulted a first-visit doctor, who practiced conservative therapy such as instruction on reducing the frequency and duration of baseball practice, along with a brief suspension of practice sessions, but the symptoms did not improve. The patient, whom the doctor suspected of having a soft tissue tumor of the left index finger, was referred to our hospital for evaluation of the symptom 9 months after the symptom onset. The left index finger showed diffuse soft tissue swelling without local heat and redness, or tenderness (Figure 1(a)). He experienced pain in the left index finger, but only when catching the ball. The active range of motion of the left index finger was 0° to 48° for the distal interphalangeal (DIP) joint, 0° to 72° for the proximal interphalangeal (PIP) joint, and 0° to 70° for the metacarpophalangeal (MP) joint. The circumferential diameter of the left index finger at the base of the finger was 6.8 cm, whereas that of the unaffected index finger was 5.8 cm (Figure 1(b)). Radiographs of the left index finger showed swelling of soft tissue without bone involvement (Figure 2(a) and (b)). Preoperative magnetic resonance showed the defined lesion in the synovial sheath of the flexor tendons, which had iso-signal intensity to muscle on a T1-weighted sagittal image (Figure 3(a)) and which had high signal intensity to muscle on a T2-weighted sagittal image (Figure 3(b)). It was enhanced in T1-weighted fat suppression with gadolinium enhancement (Figure 3(c)). Examinations revealed the following about the patient: red blood cell (RBC) count 4.41 × 1012/L (normal 4.30–5.70 × 1012/L); hemoglobin count 12.3 g/dL (normal 13.5–17.5 g/dL); white blood cell (WBC) count 6100/µL (normal 4000–8500/µL); erythrocyte sedimentation rate (ESR) 8 mm/h (normal < 15 mm/h); C-reactive protein (CRP), 0.00 mg/dL (normal 0.1 mg/dL); rheumatoid factor (RF) < 10 IU (normal < 40 IU); anticyclic citrullinated peptide antibody < 0.6 U/mL (normal < 4.5 U/mL); matrix metalloproteinase-3 (MMP-3) 12.3 ng/mL (normal 36.9–121 ng/mL); and antinuclear antibody, negative. No increase was found in inflammatory responses such as CRP, ESR, MMP-3, or positive RF and anti-cyclic citrullinated peptide (anti-CCP) antibody responses in JIA. Clinical findings led to our diagnosis of proliferative flexor tenosynovitis, which might have resulted from repeated loading with each swing of the bat or impact of the ball into the glove during baseball play and practice. He was treated with extensive flexor tenosynovectomy under general anesthesia. Brunner incision was made on the affected ring finger in the standard manner. The tenosynovium was found in the flexor tendon sheath from the level of the DIP joint to the distal palmar crease (Figure 4(a) and (b)). After the flexor tendon sheath was released, complete flexor tenosynovectomy was performed (Figure 4(c)). The collected samples were negative for Gram stain, Grocott’s stain, Ziehl–Neelsen stain, and all cultures of resected tenosynovial tissues (aerobic, anaerobic, fungal, and mycobacterial). Histologic staining confirmed the absence of microorganisms.

The left index finger (a, b) showed diffuse soft tissue swelling without local heat, redness, or tenderness (arrow).

Radiographs of the left index (a, b) showed swelling of soft tissue without bone involvement.
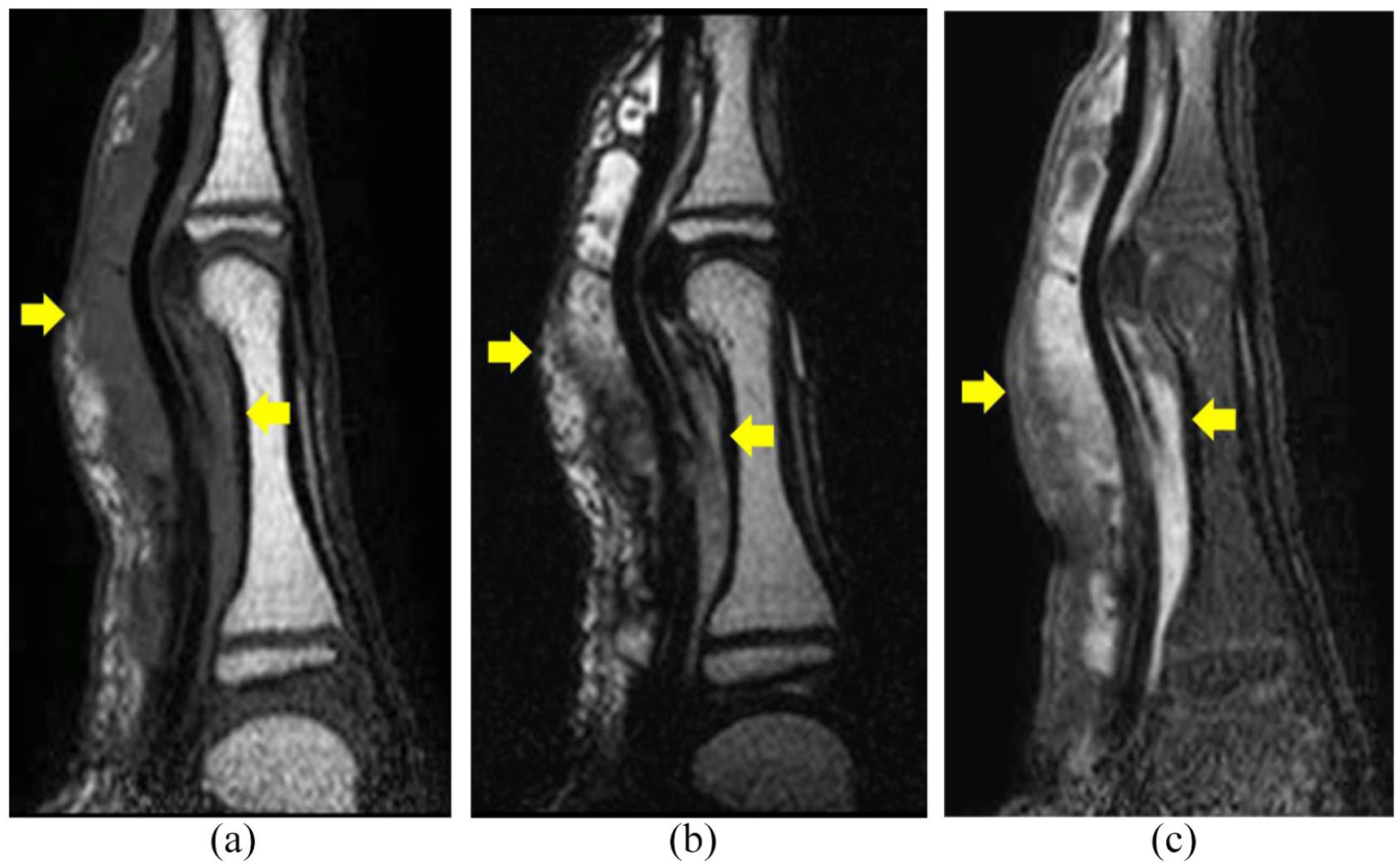
Preoperative magnetic resonance showed a defined lesion (arrow) in the synovial sheath of the flexor tendons with iso-signal intensity to muscle on a T1-weighted sagittal image (a), and with high signal intensity to muscle on T2-weighted sagittal image (b). It was enhanced in T1-weighted fat suppression with gadolinium enhancement (c).

Surgical findings were significant of extensive synovitis (arrow) affecting both superficial and deep flexor tendons (a, b). Complete flexor tenosynovectomy was performed (c).
Histopathological evaluation of the resected tissue by hematoxylin–eosin staining showed mainly proliferation of synoviocytes and plasma cell and lymphocyte infiltration: Figure 5(a), low magnification; and Figure 5(b), high magnification. No sign of recurrence was identifiable after 8 months of operation. The patient has recovered full range of motion of the affected digits (Figure 6(a) and (b)). He returned to baseball activities.

Resected tissue by hematoxylin–eosin staining showing, mainly, proliferation of synoviocytes and plasma cell and lymphocyte infiltration: (a) low magnification and (b) high magnification.

(a) After 8 months of operation, no sign of recurrence had been identified. (b) The patient has recovered the capability of full-range motion of the affected digit.
Discussion
The 10-year-old boy described in this report presented with proliferative flexor tenosynovitis of the left index finger in the gloved hand, which began to occur 2 months after starting to play baseball. Baseball players are exposed to repetitive loading to the hand with each catch of a ball or swing of a bat. Lowrey et al., after studying baseball catchers, reported less vascular change, in addition to hypertrophy and thickening associated with ischemia in the index finger because of repeated impact. 6 Ginn et al. reported a significantly higher prevalence of impaired circulation and hypertrophy of the index finger of the gloved hand in minor league catchers. 7 Our patient, a baseball beginner, was not a catcher. The repetitive load on his gloved hand might therefore have been slight. Nevertheless, because of his immature catching technique, the impact of the ball on his gloved hand, especially on the index finger, might have been concentrated. Microvascular changes of the left index finger might have engendered local tissue inflammation and edema and proliferative flexor tenosynovitis. The patient examined in our case was catching the ball with all fingers in the glove before the onset of the disease. To reduce the burden on the index finger in the gloved hand when catching the ball, we taught him to take his index finger out of the glove. Coaches should teach adequate catching skills, but it is expected that a glove for beginners should be developed that does not strain the index finger when catching a ball.
In our case, some pathological hand conditions were differentiated during the diagnosis. JIA, the most common inflammatory rheumatic condition of childhood, is associated with synovitis, joint effusion, and pain, swelling, and stiffness of joints. Results of laboratory tests including complete blood count, ESR, CRP level, RF, antinuclear antibody, and anticyclic citrullinated peptide are commonly abnormal. However, patients might occasionally have normal serologic results and have no primary complaint of joint involvement. 8 Nabet et al. 9 reported a seronegative case of JIA with proliferative flexor tenosynovitis, but without joint involvement. The patient in our case had normal serologic results and no joint involvement. However, the histologic findings of the tenosynovium showed mainly proliferation of synoviocytes and plasma cell and lymphocyte infiltration resembling those of early stage JIA. Immunological mechanisms might have been activated by the stress of baseball catching, thereby causing proliferative flexor tenosynovitis.
Second, microgeodic disease, first reported by Maroteaux, causes spindle-shaped swelling and redness in the finger or toe in children. 10 Reportedly, it is a transient disturbance of the peripheral circulation caused by cold stimulation. 11 Typical radiographic findings from patients with this disease reveal a small, round radiolucency at the edge of the metaphysis; Magnetic Resonance (MR) images show lesions with abnormal signal intensity in the affected area. 12 The patient in our case had clinical symptoms resembling those of microgeodic disease. However, the imaging findings obtained in our case were different from those of microgeodic disease.
Third, earlier reports have described that viral infection might cause flexor tenosynovitis. 13 A virally induced transient synovitis might actually occur symptomatically in tenosynovium, just as it does for articular synovium in the hip joint. However, the patient in our case had no history of viral infection before the onset of flexor tenosynovitis.
Fourth, pyogenic flexor tenosynovitis is an infectious condition of the flexor tendon sheath of the hand, which implies the four cardinal signs described initially by Kanavel. 14 The patient in our case had two signs (symmetric swelling of the entire digit, a digit with a semiflexed posture) of the Kanavel signs. However, laboratory studies yielded no inflammatory finding; bacterial culture of the resected synovium was negative. It is apparently very important to rule out similar pathological conditions when diagnosing sterile and nonspecific flexor tenosynovitis. 15
Conclusion
This report described a 10-year-old boy who had developed proliferative flexor tenosynovitis of the left index finger in his gloved hand 2 months after starting to play baseball. His immature catching technique might have led to greater impact of the ball on the index finger of the gloved hand. Findings suggest that some immunological mechanism might have been activated by baseball catching stress. Coaches and parents should devote due attention to repetitive hand trauma affecting young baseball beginners.
Footnotes
Author contributions
T.T. gathered information and wrote the manuscript; T.Y. supervised the treatment; T.T., K.S., Y.T., Y.H., and T.K. treated the patient and gathered information; T.T. and K.S. analyzed the data and contributed to discussion of the research; J.H. performed the histological examination; H.C. supervised the research. All authors have read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient’s legally authorized representative for their anonymized information to be published in this article.