
Abstract
Objective:
The thumb is very exposed to trauma due to its position and function. Fractures of the base of the first metacarpal bone are very frequent in hand traumatology. Most Bennett’s fractures are treated surgically. However, the optimal surgical approach is controversial. The aim of this study is to compare the results of closed reduction and percutaneous pinning in the treatment of Bennett’s fracture of the base of firsthand metacarpal in fractures with both small and large fragments.
Methods:
We studied retrospectively the data of 40 patients treated for a Bennett’s fracture in the department of orthopaedic and traumatologic surgery between January 2016 and December 2018. The purpose of this study was to compare the functional (pain, grip strength, first web space opening and thumb opposition) and radiological (quality of reduction and arthritic changes) results of the Iselin’s technique for the treatment of Bennett’s fractures in two groups of patients with large and small bone fragments according to the size of articular surface detached with the antero-medial fragment (superior or inferior to 25%).
Results:
The average age of the patients was 34 (range = 19–66) years. Males were by far the most affected (90%). We noted 24 cases of large fragment fractures (60%) and 16 cases of small fragment fracture (40%). An excellent overall functional result was found in 68.8% of cases of small fragment fractures versus 50% of cases of large fragment fractures. Radiological results were roughly similar.
Conclusion:
All surgical techniques aim to restore the articular congruence to the best, maintain the opening of the first web space and obtain a stable and painless trapezo-metacarpal joint. The Iselin’s technique is simple, inexpensive and easy to perform even by inexperienced surgeons. It yields satisfactory results in most cases of Bennett’s fracture regardless of the size of the fragment.
Keywords
Introduction
Due to its function and situation, the thumb is very exposed to trauma. Fractures of the base of the first metacarpal bone are very common and Bennett’s fracture is the most encountered one.
This fracture had been described for the first time in 1882 by the Irish surgeon Edward H. Bennett. 1 It is in an articular fracture of the base of the first metacarpal bone separating an antero-medial fragment of various sizes and resulting in subluxation of the trapezo-metacarpal joint.1,2
When neglected or mistreated, it can affect the articular surface and compromise the thumb function by the means of malunion, arthrosis and first web space contracture.2,3
The treatment options are still debatable. Closed reduction and cast immobilization without osteosynthesis are usually unstable because of the deforming forces (abductor pollicis brevis, flexor pollicis brevis, adductor pollicis flex distally and abductor pollicis longus extend proximally); therefore, most Bennett’s fractures are treated surgically since conservative management is only indicated in undisplaced fractures. 4
Surgical fixation techniques include various closed reduction and percutaneous pinning (CRPP) methods, open reduction and internal fixation (ORIF) and arthroscopically assisted fixation. The optimal treatment remains debatable among orthopaedic surgeons.
Classically, ORIF has been recommended when the fracture fragment is greater than 25% of the articular surface and when the joint line cannot be reduced to less than 2 mm of displacement with closed reduction.5 –9
Many studies have shown unsatisfactory reduction using closed methods.5,6 Guss et al. 10 in 2016 proposed a treatment algorithm where large fragment Bennett’s fracture is a straightforward indication for ORIF.
In our institution, all displaced Bennett’s fractures are treated with CRPP regardless of the fracture pattern (large or small fragments). Considering that less perfect joint surface reduction is achieved by closed methods as suggested by many authors, the likelihood of having bad functional results with arthritic changes would be higher in fractures with large articular involvement (i.e. large fragment fractures) treated with closed methods.
Our hypothesis is that percutaneous pinning would then result in inferior functional and radiologic results when applied to fractures with large fragment.
The purpose of our study is to compare radiologic and functional results of CRPP using the Iselin’s technique in the treatment of Bennett’s fractures with large and small fragments.
Materials and methods
Between January 2016 and December 2018, the register of the Hand Trauma Unit patients was reviewed. Inclusion criteria were all patients treated surgically for a Bennett’s fracture regardless of age and associated lesions.
In this period, 50 patients were hospitalized and treated for a Bennett’s fracture in the department of Orthopaedic and Traumatologic surgery. All surgeries were done by various senior registrars at the Hand Trauma Unit.
After applying the exclusion criteria that were pathological and open fractures, surgical techniques other than the Iselin’s method, incomplete records and follow-up period of less than 6 months, the records of 40 patients were enrolled and reviewed retrospectively and epidemiological, clinical, histological and therapeutic data were collected.
Written informed consent for the surgical procedure was obtained from all patients prior to surgery. Telephonic verbal consent to include personal records in the study was taken from all participants.
Classification
In 1933, Mc Nealy and Lichtenstein classified first metacrpal bone fractures in five types, 10 two of them are Bennett’s fractures (Figure 1):
Bennett’s fracture with large fragment: separation of an antero-medial fragment larger than the third of the articular surface.
Bennett’s fracture with small fragment: separation of a fragment smaller than the third of the articular surface.

Bennett fractures with large (a) and small (b) fragments.
Surgical technique
All our patients were operated according to the Iselin’s technique 10 : after general or locoregional anaesthesia, a double percutaneous pinning is made using two 12 or 15/10th pins (Figure 2). A small cutaneous approach enables to identify and protect thin sensory cutaneous nervous branches. The reduction will be maintained briefly by a metallic cup placed by the assistant in the first web (Figure 1(a)).

Closed reduction is achieved by axial traction and pressure on the base of the first metacarpal (M) and maintained by placing a cup in the first web space (a). Insertion of the M2M1 pin (b) and the M1M2 pin (c). Pins are curved and cut outside the skin (c).
The first K-wire is introduced from the second metacarpal’s neck (M2) to the first one without trespassing the lateral cortical bone of the first metacarpal (M1) and permits to maintain the opening of the first web space (Figure 1(b)). The second and more proximal K-wire is introduced in a divergent way relative to the first one without crossing the medial cortical bone of M2 (Figure 1(c)). It maintains the reduction of the fracture in a better way. The pinning is made under fluoroscopic control. Wires are then bended outside the skin and cut (Figure 1(d)). Dressing is then hitched around the pins’ openings. Pin removal when bone is consolidated is much easier this way. A thumb spica plint is then applied and kept till the consolidation.
Radiologic assessment
The control X-rays were reviewed by a senior hand surgery consultant at the outpatient clinic.
The quality of the reduction is judged on specific radiographs of the thumb according to Kapandji, 12 by studying the presence or not of an articular step-off and its importance. In this way, the reduction is
Good if it’s an anatomical reduction or if the articular step-off is lesser than 1 mm.
Fair if the articular step-off is between 1 and 2 mm.
Poor if the articular step-off is greater than 2 mm.
Radiologic results were evaluated at the latest follow-up by studying the joint space: normal (Figure 3), malunion with articular step-off (Figure 4), subluxation and post-traumatic arthritis.

Small fragment Bennett fracture of the right thumb (a), treated with CRPP with Iselin’s technique (b). Last follow-up X-ray with excellent radiologic result (c).

Displaced large fragment fracture (a) treated with CRPP with final X-ray showing malunion with an articular step-off greater than 2 mm (b).
Functional assessment
We have evaluated our functional results on the base of four criteria used by most authors.13,14 It includes two subjective criteria, namely, pain and grip strength, and two objective criteria, namely, thumb opposition and first web opening.
Pain: It is rated in four levels according to Brazier: 13
Level 0: absence of pain
Level 1: pain during effort
Level 2: pain during daily activities (screwing, wearing clothes . . .)
Level 3: pain even at rest
Grip strength: It is subjectively evaluated based on the force of squeezing the examinator’s hand. Compared with the contralateral hand, this force was classified into four groups according to Nonnenmacher: 15
Excellent: normal strength
Good: discreet deficiency up to 20% in comparison with the contralateral hand
Average: deficiency between 50%and 80%
Poor: deficiency > 50% in comparison with contralateral hand.
First web space opening: It corresponds to the angle between the first and the second metacarpal bones measured according to Kapandji in the position of maximum thumb abduction and retropulsion. 11 This angle is compared with the opposite side. It normally ranges from 60° to 70° and decreases with age. This parameter is classified by Surzur et al. 14 in three groups:
Normal: same as contralateral upper extremity
Decreased: angle decreased by 10° to 25° in comparison with the other hand
Very decreased: angle decreased by more than 25°
Thumb opposition: It is rated by Kapandji 16 from 1 to 10 taking into consideration the route made by the thumb fingertip from its neutral position to other fingertips and the volar aspect of the fifth finger until the distal palmar fold. According to the importance of thumb opposition, Surzur et al. 14 named three levels:
Very good results: Kapandji score from 9 to 10
Good results: Kapandji score from 7 to 8
Insufficient results: Kapandji score ⩽ 6
A global result is then evaluated combining all four clinical criteria with the radiologic result. This global result was ‘Excellent’ when an excellent result is achieved in all four criteria (no pain, normal grip strength, normal first web space opening and very good opposition of the thumb) with normal joint space on X-ray; on the contrary, a ‘Bad’ global result is applicable to patients with unacceptable results in all four criteria (pain at rest, diminished grip strength, limited web space opening and insufficient Kapandji opposition score) associated with radiological abnormalities. All other associations were classified as ‘Good and Fair’ global results.
Statistical analysis
All the data entry was done as a multi-parametric database using Excel 2010®. The analytic and descriptive statistical studies were performed using SPSS® version 25.
The variables gathered are first described by the usual parameters: number (n) and percentage (%) for categorical variables, and average, standard deviation and extreme values for continuous variables.
The non-parametric Mann–Whitney U test was used to examine the difference between the two groups as the data were not normally distributed as well as to compare the quantitative variables of the two groups. The comparison of the qualitative variables between the two groups was made using either the ‘Chi-square Test’ or the ‘Fisher’s Exact Test’ according to the distribution of the variable.
A p value < 0.05 was considered statistically significant.
Results
During the study period, 50 patients were hospitalized and treated for Bennett’s fracture, an average of 17 cases per year. Forty patients met the inclusion and exclusion criteria and were enrolled in the study. The average age of the patients was 34 (range = 17–66) years. Males were by far the most affected (90%). The left side was involved in 22 patients and the right side in 18 patients. Domestic accidents were the most common aetiology observed in 24 patients (60%), followed by road traffic accidents in 10 patients (25%). About 90% of the patients had their fractures by non-direct mechanism from falls on the thumb with the hand in hyperextension and abduction. About 75% of the patients presented to emergency department the same day of the trauma.
In our series, we noted 24 cases of large fragment fractures (60%) and 16 cases of small fragment fractures (40%), all of them closed.
The two groups were similar in age, gender, affected side, mechanism of injury and follow-up with p values > 0.05 (Table 1).
Demographics of the two groups.

All our patients had surgical treatment by closed reduction and percutaneous inter-metacarpal skewering according to Iselin. 17 The removal of the pins and the commissural splint was carried out at consolidation. The cast was maintained for an average of 5.5 (range = 3–8) weeks.
Functional results
The average follow-up was 12.5 (range = 8–18) months. An ‘Excellent’ global result was noted in 68.8% of cases of small fragment fractures versus 50% of cases of large fragment fractures (p = 0.485).
On the contrary, a ‘satisfactory’ result (encompassing ‘excellent’ and ‘good’ results) was recorded in all the patients with a small fragment fracture and in 91.7% of cases of large fragment fractures (p values of 0.240 and 0.505 respectively).
Bennett’s small fragment fracture has been found to produce less residual pain. In fact, 75% of patients did not experience any pain, whereas for the large fragment fracture, half of the patients had residual pain of different intensity at their latest follow-up. The difference was not statistically significant though (Table 2).
Residual pain depending on the type of fracture (p = 0.3).

For the small fragment fractures, the grip strength was excellent in 81.3% of the cases, good for the rest and no bad results were noted. The result was less good for the large fragment fractures where only 41.7% had excellent grip strength. The difference was found to be statistically significant with regard to excellent grip strength results with a p value of 0.013 (Table 3).
Grip strength depending on the type of fracture.

The opening of the first web space was normal in all the patients with small fragment Bennett’s fractures. This parameter was equal to 75% for the large fragment fractures (Table 4).
First web opening depending on fracture type (p value = 0.092).

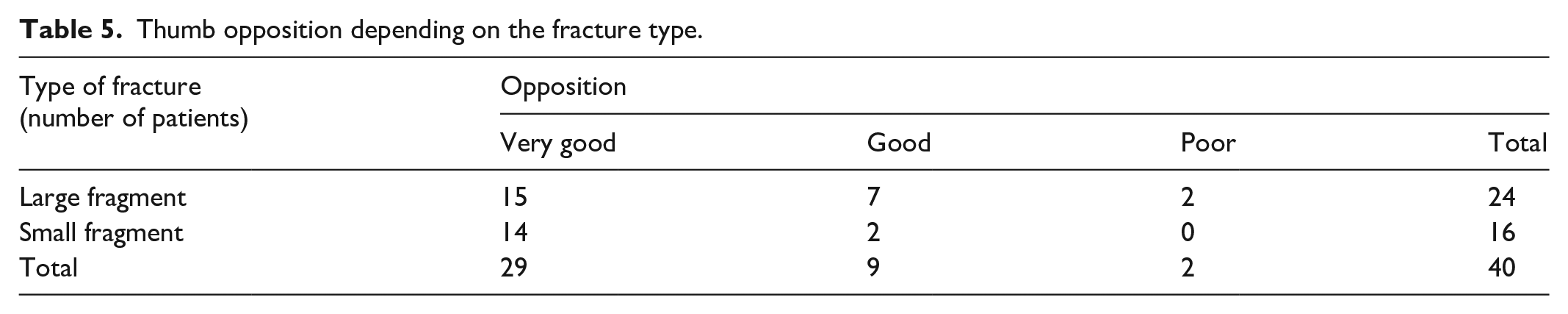
Very good thumb opposition was found in 87.5% of patients with small fragment Bennett’s fractures and 62.5% of large fragment fractures (Table 5).
Thumb opposition depending on the fracture type.
Radiological results
Radiological check-up showed normal joint line spacing in 81.3% of small-fragment Bennett’s fracture cases. This same result was noted in 54.2% of large fragment fractures (p = 0.079).
Discussion
Bennett’s fracture is a trapezo-metacarpal fracture dislocation or rather a two-fragment separation-luxation fracture. It is similar to pure trapezo-metacarpal dislocation. It differs from it by the presence of a fracture line of variable size, always clear, which separates two fragments. The first fragment, the smallest, includes the antero-medial angle of the base of the first metacarpal, which remains in place, attached to the trapezium, because the medial postero-oblique ligament is inserted there. The second fragment carrying the rest of the first metacarpal undergoes a double displacement, first a trapezo-metacarpal posterolateral dislocation, under the effect of the abductor longus of the thumb, and then in adduction, closing the first web space, under the effect of the internal thenar muscles: short adductor of the thumb and first palmar interosseous muscle. 18
Since 1882, many therapeutic methods have been proposed to treat Bennett’s fractures. Definitive treatment recommendations are difficult to make because of limited follow-up and lack of prospective randomized studies. 10
The common goals of all these methods are 14 to restore the articular congruence to the best, to maintain the opening of the first web space and to obtain a stable and painless trapezo-metacarpal joint.
The inter-metacarpal double pinning according to Iselin 17 is our preferred technique. Its advantages are the following:
Simplicity: It is a simple inter-metacarpal pinning that doesn’t require much manipulation or experience. Indeed, it is often carried out by young surgeons in training.
It is a closed method of fixation minimizing septic risk.
Pinning is done at a distance from the joints and the fractured hearth.
The protection of the web space opening as long as the principles of convergence of the pins and not crossing the far metacarpal cortex are respected.
However, some authors have pointed out some drawbacks: Foucher 19 criticizes Iselin’s technique for being imprecise in joint reduction which could be a factor of osteoarthritis. In addition, there is a risk of injury of the extensor tendon of the index finger in case of laborious passage. The complications cited by Sedel 20 are pseudo-arthrosis, sensory disorders, neurosis and hypoesthesia. These complications are rare. Indeed, pseudo-arthrosis is exceptional given the richness of the vascular supply to the base of the first metacarpal which is an anastomotic type. It is rather due to the gapping of the fracture. All authors reported satisfactory results in more than 85% of Bennett’s fractures treated with inter-metacarpal double-skewering according to Iselin. Bennani et al. 21 reported 90.5% satisfactory results. He considered inter-metacarpal double pinning to be the method of choice in treating Bennett’s fractures. It allows a stable support and guarantees a good reduction of the thumb by keeping open the first web space.
For Saadi et al., 22 inter-metacarpal double-skewering is a technique of choice in the surgical treatment of Bennett’s fracture. It allows a good reduction in closed focus and satisfactory functional results.
For Surzur et al., 14 Iselin’s inter-metacarpal double-pinning technique is simple, relatively easy to perform even by inexperienced surgeons. It works well despite the fact that young surgeons sometimes obtain a rough reduction. He concluded that a small imperfection of the reduction is less pejorative than the non-respect of the web space opening.
Obry et al. 23 consider the Iselin’s technique to be simple and respectful towards the commissural opening, leaving free the trapezo-metacarpal joint which makes it suitable for all types of fractures.
Classically, ORIF has been recommended when the fracture fragment is greater than 25% of the articular surface and when the articular surface cannot be reduced to less than 2 mm of displacement with closed methods.5 –9 The literature is unclear regarding what is an acceptable articular reduction and whether a small articular step-off (<2 mm) will have long-term clinical effects, even with evidence of radiographic arthritis. Leclere et al. 24 could not find a correlation between ‘accuracy of the fracture reduction (<2 mm gap or step-off) and development of arthritis’.
In 2003, Lutz et al. 25 compared 15 patients treated with ORIF and 17 with CRPP with mean follow-up of 7 years. Clinical and radiographic arthritic outcomes were comparable in the two groups, but there was a significantly higher incidence of adduction deformity with pinning.
Residual pain was less common in patients with small fragment fractures than in patients with large fragment fractures. According to Zine et al., 26 it is the joint cartilage contusion caused by the fracture that causes the pain.
As far as the grip force is concerned, the result was similar to that observed for residual pain.
The same is true for the opening of the first web space and the opposition of the thumb in which the best results were observed for small fragment Bennett’s fractures.
It is thought that this can be explained by the better reduction of small fragment fracture compared with large fragment fracture.
In total, the analysis of these criteria according to the type of fracture showed us that the Bennett’s fracture with small fragment gives a better result than that of large fragment fractures.
This same finding was noted by several authors such as Surzur et al. 14 and Ettoumi. 27 However, the differences between the two groups were not statically significant in our study except for the grip strength.
Radiologically, small fragment Bennett fractures were found to have the best anatomical results. But treatment of large fragment fractures with the same percutaneous pinning method has also been quite successful.
This study shows that, unlike the general belief, large fragment Bennett’s fractures can be treated with closed reduction and percutaneous pinning (CRPP) with reasonably good results comparable with those of small fragment fractures. Furthermore, it is yet to be determined whether the benefits of ORIF outweigh the risks when compared with CRPP in order to prevent potentially clinically insignificant radiographic changes of the CMC joint. 10
The shortcomings of this retrospective study are the small sample size as well as the lack of statistical calculation methods for the sample size of the study. The short follow-up period not sufficient for osteoarthritic changes to appear in a non-weight-bearing joint such as the CMC joint of the thumb is another limitation of this study.
Randomized prospective studies with long-term follow-up results comparing ORIF and CRPP in Bennett’s fracture would help us understand the difference between the clinical outcomes of the two treatments. 10
Conclusion
The optimal treatment of Bennett’s fractures remains debatable. In the absence of randomized long-term studies, no clear treatment algorithm can be maintained. In our hands, the inter-metacarpal double-pinning technique according to Iselin is a simple, inexpensive and easy technique to perform even by young, inexperienced surgeons. If technical measures are applied, good results can be obtained both in large and small fragment Bennett fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval
Ethical approval for the study as well as the method of obtaining informed consent (written informed consent before surgery and verbal telephonic consent for the use of personal records) was granted from the Medical Ethical Committee at the MTM Hospital, Nabeul, Tunisia (Ethics Approval Number: CE31/2021).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written Informed consent for the surgical procedure was obtained from all individual participants. Because it’s a retrospective series, it was impossible to obtain written consent from all patients to use personal records for the study for obvious economical and practical reasons (patients living far and unwilling to pay the travel charges to sign consent). Instead, telephonic verbal consent to include personal records in the study was taken from all participants. This was approved by the Medical Ethical Committee at the MTM Hospital (Ref: CE31/2021).