
Abstract
We herein describe a case of an 83-year-old man who presented with epigastralgia, vomiting, and abdominal distention. The physical abdominal examination revealed mild tenderness. Computed tomography revealed intramural gastric gas spread throughout the stomach, intraabdominal free gas, and hepatic portal venous gas. We diagnosed gastric emphysema with intraabdominal free gas and hepatic portal venous gas. We selected a wait-and-watch approach because physical examination did not show any peritoneal signs, although the radiological examinations showed remarkable findings. As a result, he received conservative therapy with fasting, intravenous infusion of antibiotics, and gastric decompression by nasogastric intubation. The patient was relieved of the symptoms, and follow-up computed tomography showed that all the abnormal gas disappeared soon after the treatment. In conclusion, the intramural gastric gas even with both intraabdominal free gas and hepatic portal venous gas does not always require surgical intervention. In case clinicians including general surgeons and physicians encounter intraabdominal free gas with hepatic portal venous gas, gastric emphysema should be considered in the different diagnosis. Lack of knowledge may lead to misdiagnosis, which may result in unnecessary surgical intervention.
Keywords
Introduction
Pneumatosis cystoides intestinalis (PCI), which is introduced to the gastroenterologists and surgeons in the recent years, is characterized by free gas in the submucosal or subserosal layer of the gastrointestinal tract. 1 Among them, gastric emphysema presenting as band-like intramural bubbles within the wall of the stomach is clinically rare.2,3 Furthermore, though PCI or hepatic portal venous gas (HPVG) does not always mean bowel ischemia, PCI coexisting with HPVG is highly suggestive of transmural bowel infarction.4,5
Likewise, intraabdominal free gas (IFG) is demonstrated in the case of perforation of the digestive tract. In most cases with both IFG and HPVG, the mortality rate is 82% according to Wiesner et al., 4 and urgent diagnosis and management, including surgical intervention, should be considered. 6
As previously reported, some of the PCI with IFG and HPVG are not always necessary for surgical intervention. 7 Similarly, with regard to gastric emphysema, Tang et al. 8 described that HPVG may be seen in benign gastric emphysema, and patients with stable vital signs can be managed conservatively. Although there have been no reports with gastric emphysema combined with IFG and HPVG, however, gastric emphysema coexisting with IFG and HPVG simultaneously cannot be underestimated be as life-threatening factors. Thus, the patient conditions with gastric emphysema can be confusing.
We herein emphasize on the diagnosis of gastric emphysema by the gastroenterologists through the case of a patient who presented with gastric emphysema combined with IFG and HPVG. The patient was successfully treated without surgical intervention. We consider that clinical history, conditions and vital signs, and physical abdominal findings of the patient are most important to avoid misdiagnosis and unnecessary surgery.
Case report
An 83-year-old man who presented to our emergency department with acute epigastralgia, vomiting, and sense of abdominal distention, was admitted to the Department of Surgery at our institution. The patient had a past history of appendectomy and cholecystectomy. In addition, he had been treated with oral levothyroxine sodium hydrate for hypothyroidism (dosage: 75 μg per daily). Three months prior to visiting our institution, the patient began to have a stagger and slurred speech because of hypothyroid coma. The patient was rushed to the previous hospital and admitted. Impairment of consciousness was prolonged, and the patient fell into deep coma (Glasgow Coma Scale; eye opening 1, best verbal response 1, and best motor response 1). 9 In addition, the patient was affected with aspiration pneumonia as a comorbidity of hypothyroid coma. Tracheal intubation could not be avoided, and the patient had been managed using mechanical positive pressure ventilation for 9 days. Eventually, extubation was realized. Tracheotomy was not required. However, the patient suffered from a repeated bout of aspiration pneumonia and was forced to be in lying position for a prolonged period. Thus, the patient was unable to feed by mouth, and a nasogastric tube that had already been intubated remained intubated for feeding prior to admission to our institution. Thereafter, the patient was presented to our emergency department with acute epigastralgia, vomiting, and sense of abdominal distention. Physical examination revealed mild epigastric tenderness and distension without any peritoneal signs. His blood pressure was at 128/79 mmHg; his pulse rate was fast at 98 beats/min; and body temperature was at 36.6°C. The degree of oxygen saturation was low at 93% (ambient air). In hematological parameters, white blood cell (WBC) count and C-reactive protein (CRP) were elevated up to 12800/μL and 1.27 mg/dL, respectively. The serum levels of blood urea nitrogen and creatinine were also elevated (41.7 mg/dL, 1.59 mg/dL, respectively), which were different compared with those of his blood samples withdrawn during his normal condition (10.5 mg/dL and 1.30 mg/dL, respectively). In radiological examination, a plain chest radiograph showed no free gas in the bilateral subdiaphragmatic space. A plain abdominal radiograph showed paralytic small intestine probably due to spread of inflammation in the abdominal cavity. Computed tomography (CT) revealed that intramural gastric gas spread throughout the stomach. Moreover, HPVG, especially in the left lobe of the liver, was also identified, coexisting with IFG around the stomach, but ascites was not present (Figure 1(a) and (b)). Subsequently, we added arterial blood gas analysis, which showed no abnormality (PH = 7.40). We did not perform blood culture because the patient was afebrile, and his vital signs were stable. We initially assumed perforation of the digestive tract; however, the upper gastrointestinal series using oral water-soluble contrast medium revealed no perforating site in the stomach (Figure 2). Furthermore, we assumed that irreversible ischemia would have been accompanied; however, we could not establish a definitive preoperative diagnosis. We selected a wait-and-watch approach because physical examination did not show any peritoneal signs, although the radiological examinations showed remarkable findings. As a result, he underwent conservative therapy with fasting, intravenous infusion of antibiotics, and gastric decompression by nasogastric intubation. Cefmetazole (2 g per daily) was administered for 3 days. The patient was easily relieved of the symptoms, and WBC and CRP were normalized 10 days after the treatment. In addition, the follow-up CT revealed that the intramural gastric gas, IFG, and HPVG disappeared just 3 days after the treatment (Figure 3). After the patient was completely relieved of the symptoms, esophagogastroduodenoscopy showed mild redness in the upper stomach on the 10th day (Figure 4), and total colonoscopy showed no abnormalities on the 17th day after starting the treatment. Eventually, the patient was permitted for oral intake 3 weeks after the treatment, and the patient has been well since the discharge. Comprehensively, we diagnosed the patient with gastric emphysema accompanied by IFG and HPVG. The radiological work-up showed no evidence of recurrence over a half-year follow-up period. Because the patient was unable to write letters, verbal informed consent was obtained from the patient for publication of the case report and the accompanying images. Thus, written informed consent was obtained from his oldest daughter retrospectively for publication of the case report and the accompanying images.

CT reveals intramural gastric gas spread throughout the stomach (black arrows), coexisting with IFG around the stomach (white arrows), but not ascites (a). HPVG is identified, especially in the left lobe of the liver (white arrows) (b).
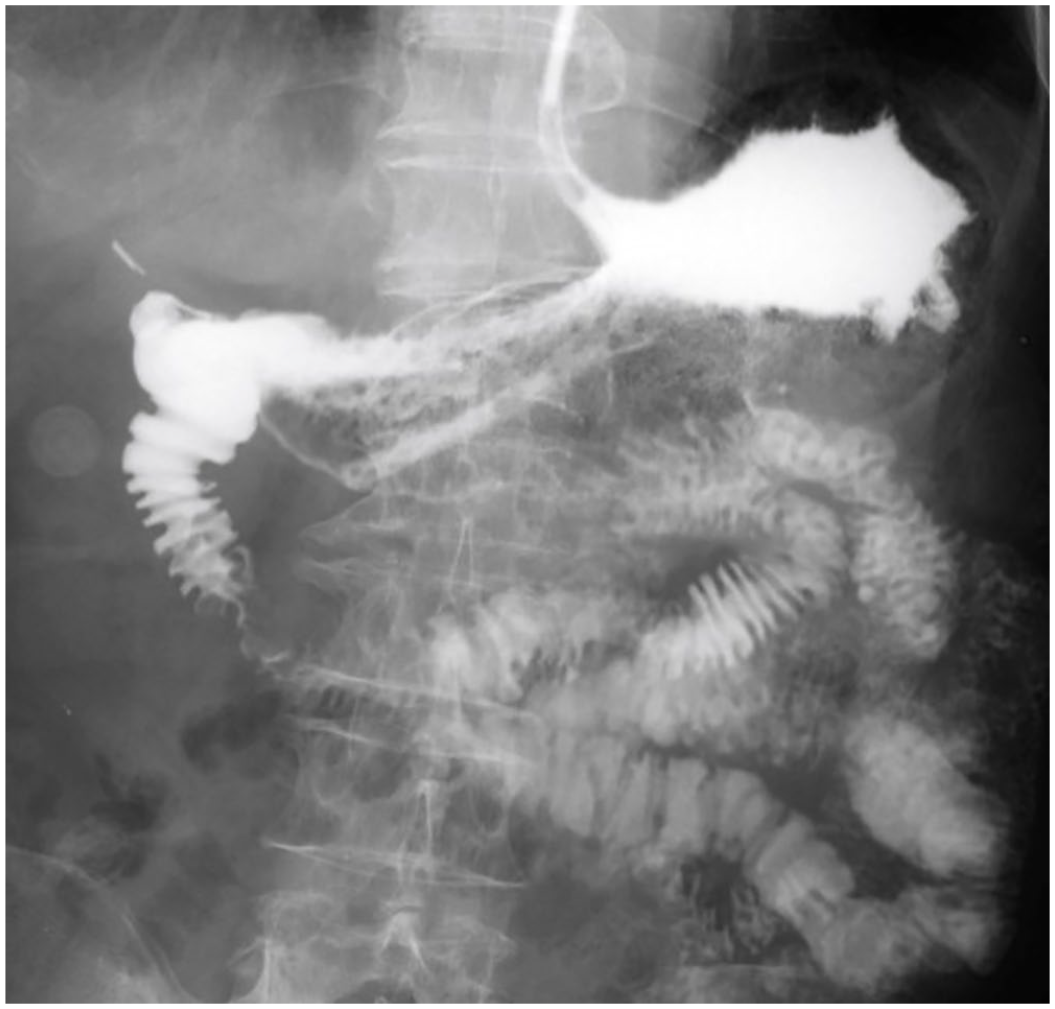
Upper gastrointestinal series by oral water-soluble contrast medium reveals no perforations in the stomach.

CT reveals intramural gastric gas, IFG, and HPVG disappearing 3 days after the treatment.
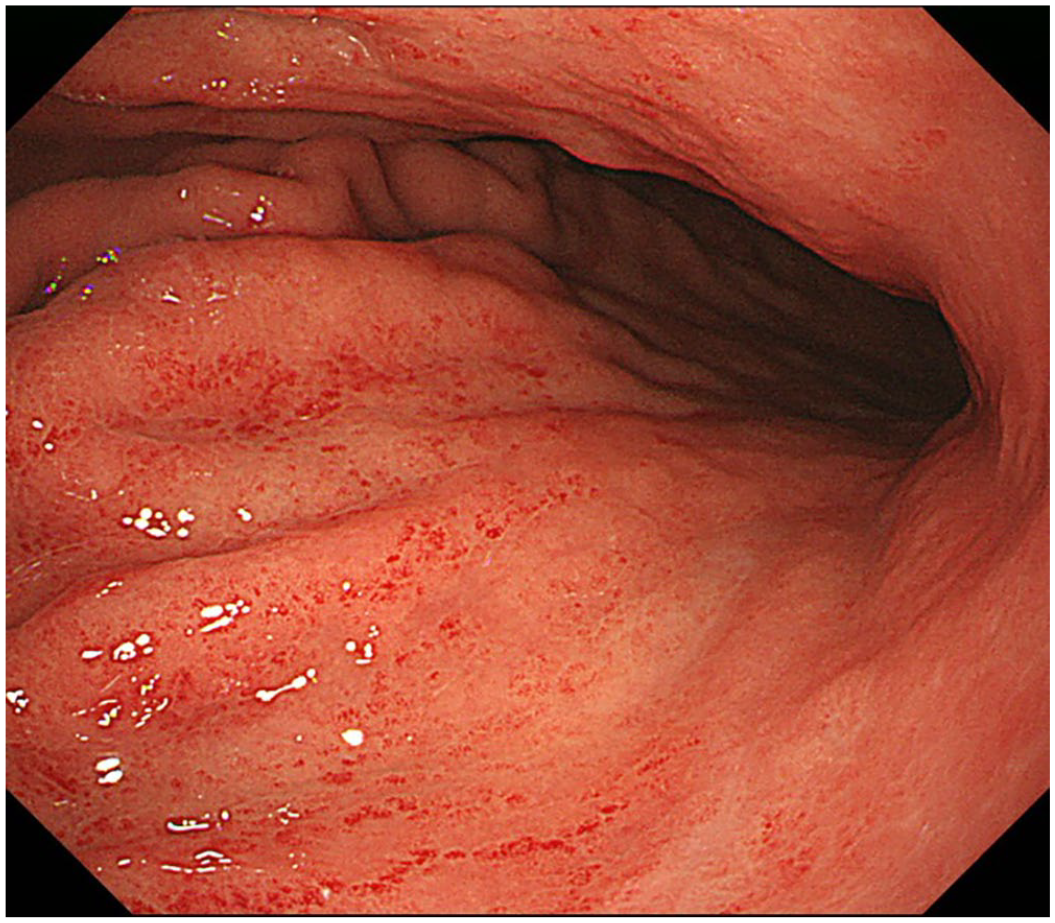
Esophagogastroduodenoscopy shows only mild redness in the upper stomach.
Discussion
This report is the first case in the world that describes gastric emphysema, IFG, and HPVG simultaneously, based on our search in the English literature using MEDLINE. The most significant point of this report is if clinicians can make a correct judgment regarding need for surgical intervention when they encounter these fatal conditions of gastric emphysema, IFG, or HPVG. It is natural for clinicians to fear digestive tract perforation or ischemia because it can be fatal. IFG and HPVG are both radiological signs of underlying serious gastrointestinal pathology, such as ischemia or necrosis. The mortality for HPVG ranges between 75% and 95%. 7 Khalil et al. 10 mentioned that the coexistence of PCI and HPVG is associated with bowel ischemia in about 70% of cases. If these two pathological conditions coexist, it can be fatal for the patient if clinicians do not administer any treatment. 6 Therefore, clinicians are required to make quick decisions regarding the need for surgical intervention. 11
PCI is characterized by free gas in the submucosal or subserosal layer of the gastrointestinal tract. The most common location of gas was in the submucosa (69.9%). 1 Koss 12 first reviewed the cases with PCI and reported that approximately 85% of all cases were classified as secondary PCI, derived from other underlying disease. Morris et al. 13 showed that the incidence of PCI was 46% in the colon, followed by 27% in the small intestine, 7% in the colon and small intestine combined, 5% in the stomach, and the remaining in other gastrointestinal tract. The term “gastric pneumatosis” or “gastric emphysema” are both used interchangeably for indicating the same pathological condition of intramural gastric gas in MEDLINE. It appears that both terms are not defined to use differently. We think that gastric pneumatosis or gastric emphysema may be categorized as a part of PCI.
In general, as Agha 14 previously described in 1984, gastric emphysema can be divided into three categories based on its pathogenesis: (1) obstructive type, (2) traumatic type, and (3) pulmonary types. In this case, the following hypotheses for specific causative factors have been made. First, gastric emphysema occurred because the patient had been given positive pressure ventilation by mechanical ventilator for 9 days due to respiratory failure caused by aspiration pneumonia. Second, increased intramural gas in the stomach was partially transported via gastric drainage veins to the hepatic portal veins. Subsequently, transient ruptures of serosa of the stomach caused IFG. If these hypotheses are possible, the mechanism of life-threatening conditions, such as gastric emphysema, IFG, or HPVG can be reasonably explained. Agha 14 reported that the pulmonary type of gastric emphysema is the rarest subclassification, and all pulmonary cases were caused by air from ruptured bullae dissected along the vascular sheaths reaching the paraesophageal area followed by a gradual downward dissection into the gastric submucosa conducing to gastric emphysema. In this case, the patient did not show bullae on CT. In the meantime, Reuter presented a case of gastric emphysema with HPVG caused by mechanical trauma due to long-time resuscitation and bag-mask ventilation. The author speculated that gastric emphysema and HPVG were primarily caused by the distention of the stomach during cardiopulmonary resuscitation. 5 This case is similar due to cardiopulmonary resuscitation and tracheal intubation; however, the disappearance of gastric emphysema combined with IFG and HPVG immediately after the treatment is unexplained, because the patient was given respiratory support by mechanical ventilation about 2 months prior. Third, it appears that the nasogastric tube placement can be one of the triggers. The patient was fed using the nasogastric tube because of repeated vomiting. Zenooz et al. 15 reported a case of gastric emphysema following the nasogastric intubation. They raised instrumentation such as biliary stenting, nasogastric tube placement, endoscopy with air insufflation, or gastrostomy as benign causes of gastric emphysema. 15 The mechanism of how nasogastric tube placement induces gastric emphysema and whether duration of placement concerns or not is still unclear. Surely, we can substitute gastrostomy for nasogastric tube for the purpose of feeding; however, we should recognize that gastrostomy can also be a cause of gastric emphysema. Thus, it is also important to obtain the past and present medical history to identify the confrontive causes of gastric emphysema.
Differential diagnosis of gastric emphysema and emphysematous gastritis (EG) is important because they have varying prognosis despite similar appearances on imaging studies. EG can be confused with gastric emphysema because both are identified by accumulation of gas within the gastric wall. EG is a rare form of gastritis caused by invasion by gas-producing organism.15,16 Because of its fulminating course, it can be an emergency with life-threatening complications, usually resulting in emergent surgery. 17 Patients with EG rapidly progressed to a state of septic shock by bacterial invasion of Streptococci, Escherichia coli, Enterobacter species, Pseudomonas aeruginosa, and Clostridium perfringens that results in death in spite of medical treatment with a high mortality rate of 60%–80%.17,18 Pursuantly, prompt diagnosis and treatment are required to prevent further complications. 17 Although EG and gastric emphysema present overlapping clinical features and radiological findings, CT is very useful and the most sensitive modality for the diagnosis of gastric emphysema. CT shows that the intramural air has the characteristics of round air bubbles in EG, while gastric emphysema shows single or double linear stripes or streaks with round areas of radiolucency a few millimeters wide and parallel to the border of the stomach.15,17,19,20
Thus, we definitively diagnosed the patient with gastric emphysema combined with IFG and HPVG. In addition, we could treat these life-threatening conditions without surgical intervention using the conservative wait- and-watch approach. We think the location and degree of IFG does not have an impact on treatment strategy for the case with IFG, HPVG, and gastric emphysema simultaneously. We reiterate that the reasons we chose conservative therapy in this case were as follows: (1) the patient did not show any peritoneal signs; (2) vital signs, such as blood pressure, pulse rate, or oxygen saturation were stable; (3) arterial blood gas did not show metabolic acidosis; (4) inflammatory parameters, such as WBC and CRP were slightly elevated; and (5) CT showed the typical findings of gastric emphysema without ascites, and not those of EG.
In case clinicians including gastroenterologists and general surgeons encounter IFG with HPVG, gastric emphysema should be considered in the different diagnosis. Lack of knowledge may lead to misdiagnosis, which may result in unnecessary surgical intervention.
Conclusion
In conclusion, the intramural gastric gas even with both IFG and HPVG does not always require surgical intervention. A judgment is required on the basis of knowledge of gastric emphysema.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient’s old daughter who was legally authorized representative for anonymized information to be published in this article. The patient had definitely agreed his anonymized information to be published in the article; however, the patient was not able to write letters because he had been bedridden for a long period. Verbal informed consent was obtained from the patient for his anonymized information to be published in this article.