
Abstract
Metastatic carcinomas in the nasopharynx are a rarity. We report a case of a 54-year-old male patient who presented with a history of recurrent epistaxis. On evaluation, a mass in the right Rosenmüller fossa was detected, which was biopsied and diagnosed as a poorly differentiated adenocarcinoma, immunoreactive for thyroid transcription factor-1, consistent with metastatic pulmonary adenocarcinoma. Fluorodeoxyglucose–positron emission tomography/computed tomography (FDG-PET/CT) scan confirmed the presence of a mass in the upper lobe of the left lung, proven pathologically to be a poorly differentiated pulmonary adenocarcinoma, with an immunoprofile similar to the nasopharyngeal tumor. The patient underwent palliative chemotherapy, and was then shifted to immunotherapy. He is currently alive and disease free 50 months after the initial diagnosis was made. The unusual presentation of a metastatic carcinoma in the nasopharynx will be discussed, along with a review of literature. The role of immunotherapy in cancer control and greater longevity will also be presented.
Introduction
In the nasopharynx, malignant tumors predominate, with nasopharyngeal carcinoma (NPC) constituting most cases. 1 Tumors metastasizing to the nasopharynx are seldom seen in clinical practice. 2
Lung cancer is the most common cancer worldwide and the leading cause of cancer-related mortality. 3 Pulmonary adenocarcinomas frequently metastasize to the regional lymph nodes, bone, liver, adrenal glands, and the brain. 4 However, pulmonary adenocarcinomas may present with metastases in unusual sites, including the conjunctiva, 5 and paranasal sinuses. 6
Currently, only a single other case of an isolated metastatic nasopharyngeal carcinoma originating from a pulmonary adenocarcinoma is reported in English language literature. 7
The diagnostic tools used in our case were pathological analysis and Fluorodeoxyglucose–positron emission tomography/computed tomography (FDG-PET/CT) scan, a non-invasive imaging technique which has, over the past decade, proven to be a valuable modality for the diagnosis, staging, and detection of carcinomas of unknown primaries. 8
This report presents an unusual case of a metastatic pulmonary adenocarcinoma, which was successfully managed with immunotherapy. A literature review on metastatic nasopharyngeal carcinomas as well as the role of immunotherapy in the treatment of pulmonary adenocarcinomas will also be included.
Case report
A 54-year-old male patient presented in February 2016 with a 5-month history of recurrent epistaxis. There were no symptoms of nasal obstruction, nasal discharge, ear symptoms or headaches. The patient was an ex-smoker, who had quit smoking 9 years prior to his presentation. An evaluation done by an ear, nose, and throat (ENT) physician revealed a mass in the right Rosenmüller fossa; so a biopsy was obtained. It was initially diagnosed as an undifferentiated carcinoma at another facility. Review of the biopsy at our center revealed the presence of poorly cohesive pleomorphic cells with abundant acidophilic and focally vacuolated cytoplasm (Figure 1(a)). The tumor cells grew in a diffuse sheet-like pattern with abundant mitotic figures. The background showed unremarkable lymphoid tissue. Mucicarmine special stain highlighted the mucin content in the cytoplasm of some of the tumor cells (inset). The tumor cells were immunoreactive for CK7 (not shown) and thyroid transcription factor-1 (TTF-1) (Figure 1(b)) and negative for CK20, PAX8, CDX2, and S100 immunostains (not shown). The case was diagnosed as a metastatic pulmonary adenocarcinoma and recommendations for further clinical and radiological confirmation were made.

Tumor from the nasopharyngeal mass and the lung. (a) The tumor in the nasopharynx is composed of dyscohesive cells, with abundant acidophilic cytoplasm, and large pleomorphic nuclei, with prominent nucleoli (H&E X40). Some tumor cells contain vacuolated cytoplasm containing mucin as highlighted by mucicarmine special stain (inset). (b) The tumor cells are diffusely positive for TTF-1 (X40). A biopsy was obtained from the lung mass that showed (c) poorly formed glands with pleomorphic nuclei (H&E X40) and (d) positive TTF-1 immunostain (X40).
Maximum intensity projection image of the FDG-PET/CT scan demonstrated an intensely hypermetabolic left lung mass and a hypermetabolic right nasopharyngeal lesion (Figure 2(a)). Axial fused PET/CT images at the level of the nasopharynx demonstrated the abnormal FDG metabolic activity in the right side of the nasopharynx, at the Rosenmüller fossa (Figure 2(b)). In the thorax, an intensely hypermetabolic left upper lobe lung mass was seen, as well as hypermetabolic mediastinal lymph nodes in the aorto-pulmonary (A-P window) group (Figure 2(c)). Axial fused PET/CT images also demonstrated hypermetabolic left axillary lymph nodes (Figure 2(d)). The maximum standardized uptake value (SUVmax) of the hypermetabolic nasopharyngeal lesion was 6.2, the upper lobe lung mass was 13, the mediastinal lymph nodes were 2.9, and the axillary lymph nodes were 2.1. These were considered metastatic and further biopsy was not obtained.
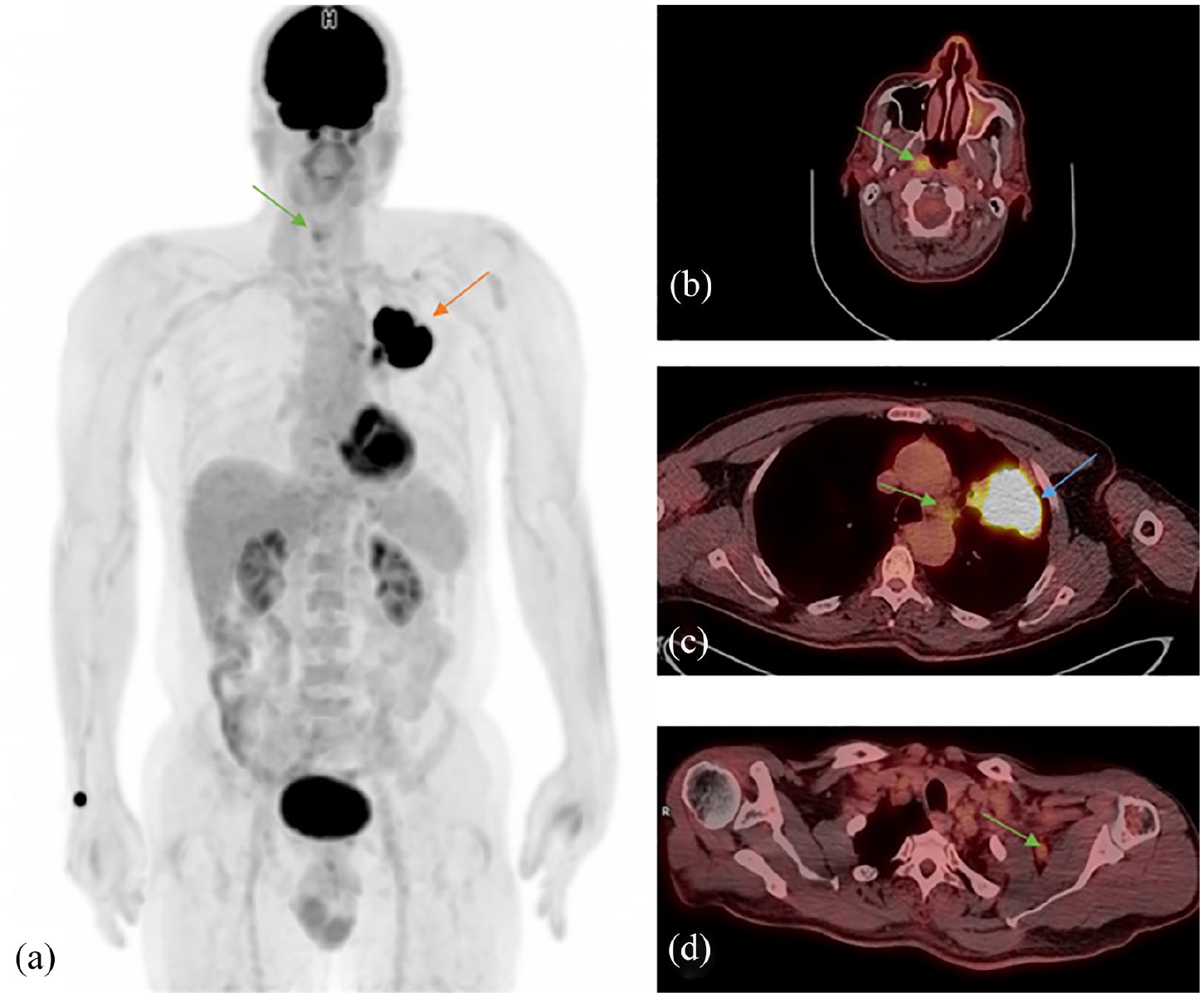
Maximum intensity projection image (MIP) of the FDG-PET/CT scan. (a) The red arrow points toward the intensely hypermetabolic left lung mass and the green arrow points toward the hypermetabolic right nasopharyngeal lesion. (b) shows an axial fused PET/CT image at the level of the nasopharynx, the green arrow demonstrates the abnormal FDG metabolic activity in the right side of the nasopharynx, at the Rosenmüller fossa. (c) shows an axial fused PET/CT image at the thorax, the blue arrow demonstrates the intensely hypermetabolic left upper lobe lung mass; the green arrow points toward the hypermetabolic mediastinal lymph nodes in the aorto-pulmonary (A-P window) group. (d) shows an axial fused PET/CT image and the green arrow points toward the hypermetabolic left axillary lymph nodes.
The mass in the upper lobe of the left lung was then biopsied and diagnosed as a poorly differentiated adenocarcinoma (Figure 1(c)) immunoreactive for TTF-1 (Figure 1(d)) and CK-7 (not shown), similar to the metastatic carcinoma in the nasopharynx. It was concluded that the poorly differentiated adenocarcinoma was the primary carcinoma. Testing for epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) came back negative. PD-L1 (22 C3) tumor proportional score (TPS) was positive in 50.0% of tumor cells. Magnetic resonance imaging (MRI) revealed another metastatic lesion in the cerebellum. According to the eighth edition of the TNM staging system for non-small cell lung cancer (NSCLC), the patient was diagnosed as stage IV (T3N2M1c).
The patient began radiotherapy (30 Gy/10fx) and chemotherapy (Carboplatin and Pemetrexed × 6). Pemetrexed was switched to Docetaxel later on. Despite treatment, there was evidence of disease progression, with the development of new metastases in the adrenal gland.
On 18 April 2017, the patient was started on Pembrolizumab (2 mg/kg) intravenous (IV) infusion in 50 ml normal saline, given over 30 min, over 32 cycles, once every 3 weeks for a period of 2 years. Pre-medications included Paracetamol (1000 mg P.O.) and Chlorpheniramine (10 mg IV over 20 min), both administered half an hour before Pembrolizumab. The patient was regularly followed-up (every 2–3 months) with chest and abdominal CT and brain MRI studies. Partial response was noted following the third cycle. Following the fifth cycle, further regression of the primary tumor was seen, alongside slight progression in the axillary lymph nodes which demonstrated a 10% increase in size. Post cycle 14, the disease began to stabilize with complete resolution of the metastatic brain and nasopharyngeal lesions. Post cycle 22, further response in the primary tumor was evident, and post cycle 26 the disease was stable. The last cycle was given on 13 February 2019, where complete resolution of the metastatic nasopharyngeal, brain, and left axillary lymph nodal lesions were noted. The last available follow-up was on 19 April 2020 (50 months following the initial diagnosis); the patient was doing well and showed no evidence of disease progression. The treatment was generally well tolerated by the patient, with no grade 3 or 4 adverse reactions seen. Two attacks of grade 2 community acquired pneumonia occurred during his treatment course, which were successfully treated on an out-patient basis.
Discussion
Squamous cell carcinoma is the most common primary NPC; it arises from the squamous epithelium lining the nasopharynx. They typically arise in the lateral wall of the nasopharynx, usually in the Rosenmüller fossa, and have well-established associations with Epstein–Barr virus (EBV) infections, genetic predispositions, and environmental carcinogens. 1 The nasopharynx is an uncommon site for metastases. However, metastases in the nasopharynx originating from unusual primaries such as hepatocellular carcinoma, 9 renal cell carcinoma, 10 and breast carcinoma 11 have been encountered.
A review of English language literature from the year 2000 up to April 2020 yielded 18 cases, including ours, of carcinomas metastasizing to the nasopharynx. Breast carcinoma is the most common (n = 6, 33.3%), followed by renal cell carcinoma (n = 3, 16.7%), hepatocellular carcinomas (n = 3, 16.7%), and bronchogenic carcinomas (n = 2, 11.1%). Table 1 summarizes the demographics, treatment, and outcome of the reported cases. These tumors generally carry a dismal prognosis; 7 (38.4%) patients succumbed to their disease within a year.
A summary of all available cases in English language literature of cancers that have metastasized to the nasopharynx from 2000 to 2020 (up to April 2020).

RCC: renal cell carcinoma; NSCLC: non-small cell lung carcinoma; FTC: follicular thyroid carcinoma; SCLC: squamous cell lung carcinoma; HCC: hepatocellular carcinoma; F: female; M: male; NA: not available; DOD: died of disease.
Metastasis at the time of presentation is commonly encountered in patients with primary lung carcinomas. These carcinomas metastasize through lymphatic and vascular channels to extra-thoracic sites, mostly to the adrenal glands, brain, bone, and liver. 5 Metastasis accounts for the generally poor outcome seen in these patients.
Whether primary or secondary, the clinical presentation of a mass in the nasopharynx varies depending on its location and extent of spread. It may present with nasal obstruction, nasal discharge, epistaxis (as was seen in our case), ear infections, diplopia, or headaches.9–11 These symptoms overlap with the presenting symptoms of a primary NPC. However, a possible distinguishing feature is cervical lymphadenopathy, due to the propensity of NPC to metastasize to the cervical lymph nodes. Moreover, the vast majority of NPC patients have positive EBV serologies. 1 Nonetheless, a confident diagnosis of a primary versus metastatic tumor in the nasopharynx remains a challenge, necessitating a high index of suspicion, the use of appropriate imaging tools, and a thorough pathological analysis.17,24
FDG-PET/CT has been playing an increasingly important role in the staging and management of head and neck tumors. MRI is superior in unfolding the exact anatomical location and extent of tumor spread, especially when the need to investigate intracranial and soft tissue invasion arises. However, FDG-PET/CT is superior due to its ability to scan most of the body using a single study, providing information not only on the primary tumor but on nodal and distant metastases, and the potential presence of second primary tumors, features which justify recognizing FDG-PET/CT as one of the most useful tools for diagnosing metastasis of head and neck cancers.1,8
Due to the scarce number of cases, there is currently no consensus or established guidelines on the best modality of treatment for metastatic nasopharyngeal carcinomas. Surgical resection proved effective in two cases.17,21 Wong et al. 7 reported a case similar to ours and advocated the use of radiotherapy; the patient responded well to treatment and remained disease free for 10 years following the initial diagnosis of a nasopharyngeal metastasis. Only a single other case, in which the patient’s condition improved, used immunotherapy as their treatment modality. 22
Immunotherapy has revolutionized the treatment of advanced NSCLC. Pembrolizumab is a monoclonal antibody that targets programmed cell death protein-1 (PD-1) receptor and is one of the few Food and Drug Administration (FDA) approved immunotherapies used to treat metastatic lung adenocarcinomas. The use of Pembrolizumab as a single agent in our case was based on the PDL-L1 TPS of 50%, negative EGFR mutations and ALK translocation, as well as the signs of disease progression despite the patient receiving platinum-based chemotherapy. This is supported by the results of the randomized trial, KEYNOTE-010, which confirmed the efficacy of Pembrolizumab in patients with previously treated NSCLC. For the subgroup of patients with a PD-L1 TPS of 50% or greater who were given Pembrolizumab, an increased overall survival and longer progression-free survival was evident in comparison to the patients on Docetaxel. 25 Of note, the detection and treatment of metastatic carcinoma as soon as possible is of paramount importance for metastatic nasopharyngeal tumors, as these tumors have the potential to invade the base of the skull, induce pain, damage cranial nerves, and could lead to focal motor deficits.17,26
Conclusion
In conclusion, here we report the second case of a metastatic pulmonary adenocarcinoma in the nasopharynx. Although the chances of encountering such a case are infrequent, a thorough examination of the patient and the recognition of this possibility is warranted. The sequence of events that led to our patient’s diagnosis and subsequent prolonged survival emphasizes the importance of maintaining a high index of suspicion when an unusual tumor morphology is encountered in an unusual location. It is through the use of FDG-PET/CT along with pathological analysis that a swift confirmation of the suspected diagnosis was rendered. The patient’s drastic improvement on Pembrolizumab supports the notion of using immunotherapy as an effective second-line treatment in advanced lung adenocarcinoma and in the treatment of nasopharyngeal metastases.
Footnotes
Author contributions
Conception of the idea: M.A-H. Collection of data: M.A-H., A.A-I., and S.Y. Literature review: S.I., J.N., R.A., and B.O. Drafting the manuscript: S.I. and M.A-H. Critical review and final approval: all authors. Accountability: all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.