
Abstract
A 62-year-old male with type 2 diabetes mellitus presented to our nationally accredited breast center with bilateral breast masses present for 7 years and new-onset pink nipple discharge for several months. Mammography and ultrasound demonstrated a left 2.7 retroareolar cystic lesion and a right 2.1 cm retroareolar solid lesion. Given the suspicious nature of the bilateral breast discharge, core needle biopsies were performed to rule out underlying malignancy. The biopsies revealed benign results, but the discordance between the biopsy, imaging, and suspicious discharge led to the decision to perform bilateral excisional biopsies. Intraoperatively, a small organism resembling a larva was encountered. The abnormal tissue was sent for histopathological examination, along with the organism, which was identified as the larvae of Musca domestica, or common house fly.
Keywords
Introduction
Breast abscess is a common pathological entity seen in surgical practice. While most commonly seen in breastfeeding mothers, they may present in a wide range of patients of both sexes. A spectrum of disease from simple mastitis to complicated abscess exists. 1 In general, breast infections are more prevalent in individuals with comorbidities such as diabetes, recent instrumentation, trauma, and tobacco use.2,3 These predisposing factors lead to a tissue microenvironment that is under-perfused, increasing the risk of infection. 2
The differential diagnosis of a breast mass is broad and includes inflammatory, infectious, neoplastic, and benign causes. When an abscess is present, most commonly it is the result of infection with Staphylococcus or Streptococcus bacterial species. 1 Uncommonly, larvae have been described in the literature as being associated with breast abscesses; however, the presence of coexisting Musca domestica in breast abscess excisions has not been previously described.
Case presentation
A 62-year-old Italian-American male presented to our nationally accredited Breast Center with a history of a prior left breast biopsy at an outside institution for a palpable mass, the pathology of which was unavailable but was reported to be benign by the patient. He also reported long-standing retroareolar masses with new onset of bilateral pink nipple discharge. He denied recent trauma or infection. He had a history of type 2 diabetes managed with metformin and a 20 pack-year cigarette smoking history. He did not have a family history significant for breast cancer or gynecomastia. On physical exam, he had appropriate hygiene, further examination was remarkable for bilateral breast tenderness on palpation without any overlying skin erythema or other local sign of inflammation and 2 × 2 cm bilateral retroareolar masses.
Mammogram demonstrated BIRADS 3 lesions bilaterally (Figure 1). Ultrasound performed the same day confirmed a 1.5 cm cystic lesion containing debris in the right breast and a 2.1 cm complex cystic and partially solid mass in the left breast (Figure 2). The presence of nipple discharge prompted bilateral ultrasound-guided core biopsies to rule out underlying malignancy, which revealed benign inflammatory tissue and a foreign body-type giant cell reaction in both lesions without evidence of malignancy (Figure 3). Microbiology results from biopsy samples grew Staphylococcus lugdunensis.

Mammogram demonstrating bilateral BIRADS3 lesions.
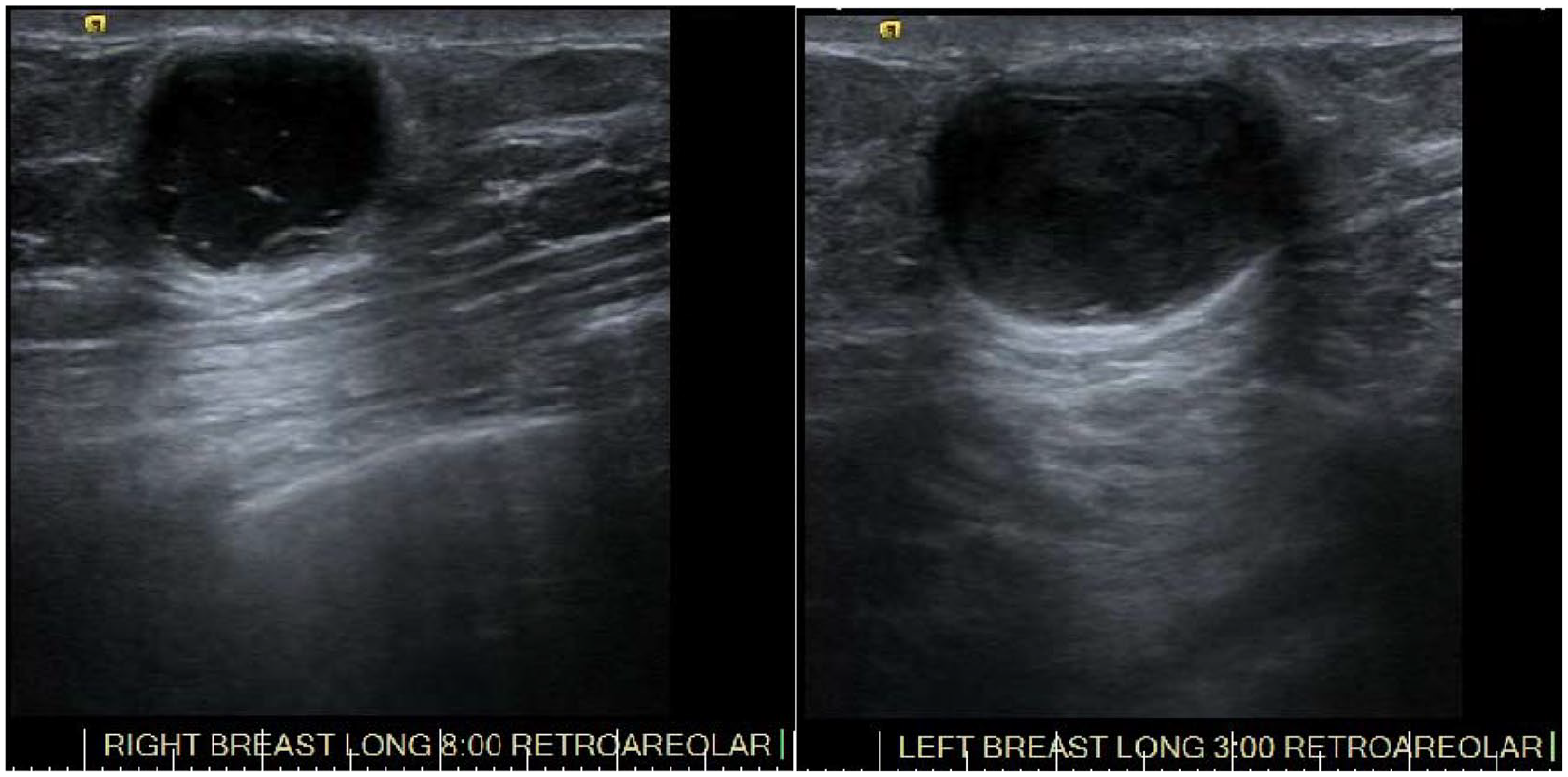
Bilateral breast ultrasound demonstrating subareolar hypoechoic masses.

Pathology demonstrating benign fibroadipose/breast tissue and subcutaneous tissue with cystically dilated ductal structures lined with benign cuboidal and squamous epithelium. The cystic structures are filled with keratin debris and have surrounding acute and chronic inflammation, granulation tissue, fibrosis and multinucleated foreign body-type giant cells.
The pathology and microbiology results were discussed with the patient, and given the symptomatic nature of his presentation and continued nipple discharge, bilateral surgical excision of the masses was planned. During the operative procedure, well-defined cystic lesions were noted. During dissection of the right-sided mass, a small defect was inadvertently created in the cyst wall, and a small larva was noted in this defect. This was sent separately with the specimen. Bilateral tissue specimens were sent for surgical pathology to rule out malignancy. The surgical pathology of both retroareolar masses revealed fibrosis and multinucleated foreign body-type giant cells, deemed non-specific (Figure 3). The organism was identified as the larvae of Musca domestica.
The patient was seen in clinic postoperatively and was determined to be recovering well from surgery.
Discussion
The concerning presence of breast discharge in our patient, accompanied by breast masses was a significant factor in the choice to offer surgical excision to this patient. When accompanied by an underlying mass, nipple discharge in a male is associated with an increased risk of malignancy. 4 Benign causes of nipple discharge in males are found infrequently in the literature. They include duct ectasia (dilation and shortening of the terminal ducts of the breast), which has been associated with HIV/AIDS and Bechet’s disease in isolated case reports. 5 Other causes include papillomata, which are rarely found in men, gynecomastia, or skin cancer located in the periareolar region. 6
Retroareolar breast abscess can develop as a reaction to infection or to the presence of foreign bodies. We hypothesize that the patient’s nipple was innoculated by the eggs of Musca domestica either through the Montgomery glands or the terminal ducts and therefore caused a foreign body-type reaction. Most commonly, breast abscesses occur in females during breastfeeding, as a result of retrograde infection. 7 Men, whose breasts do not serve the same role, have an undeveloped ductal system and therefore the risk of abscess formation is typically very low in the absence of significant comorbidities. 8
Breast abscesses are more likely to develop in a patient with a history of diabetes mellitus, smoking or previous iatrogenic procedures. Specific predisposing factors to non-bacterial abscess are not described, but would appear to be similar to those predisposing to bacterial abscesses. Adisa and Mbanaso 9 have described cutaneous infestation of the breast by the larva of Cordylobia anthropophaga (Tumbu fly), a common cause of larva infestation in humans. Other reported non-bacterial organisms found in the breast include fungi such as Candida and Cryptococcus, and parasites such as Schistomiasis and Cysticerosis. 10 In addition, many rare causes of breast abscesses have been linked to early presentations of HIV. 11 While S. lugdunensis, the bacteria identified in our patient’s biopsies, may be a component of normal skin flora, it has also been associated with cases of skin and soft tissue infections. 12 Finally, malignancy should be ruled out if antibiotic treatment of mastitis or a presumed breast abscess does not result in improvement. 13
In both women and men, treatment with broad-spectrum antibiotics and potentially needle aspiration may be necessary to ensure complete resolution of breast abscesses. If tissue necrosis exists, then the necrotic tissue should be excised to prevent infestation of non-bacterial organisms such as Musca domestica, particularly in the case of patients with predisposing factors such as uncontrolled diabetes or prior instrumentation as may have been the case for this patient.
Conclusion
We identified the larvae of Musca domestica—the common housefly—in a male breast abscess associated with nipple discharge. We posit that the patient in our case report had chronic underlying abscess which created a fertile environment for the eggs of Musca domestica. We believe this case is important to contribute to the literature because it represents an extremely rare potential sequela of breast abscess.
Footnotes
Acknowledgements
The authors acknowledge the residents, faculty, and staff of Maimonides Medical Center for their dedication to the care of patients with breast pathology.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Written informed consent was obtained from the patient including consent for the usage of radiological and pathological images for publication. Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.