
Abstract
Takotsubo syndrome has increasingly been recognized in the differential diagnosis of patients presenting with acute chest pain. Those affected are typically older women suffering after an emotional or physical stress. Normally it is a transient condition but complications including death have been reported. We reported a case of takotsubo syndrome who was initially diagnosed as acute coronary syndrome. The patient presented with typical angina, ST-T segment changes, and elevated high sensitive–troponin I. Coronary angiography showed normal coronary arteries. Transthoracic echocardiography revealed mild left atrial dilatation and left ventricle concentric hypertrophy, reduced left ventricle ejection fraction with circumferential hypokinetic, apical ballooning, systolic anterior motion, left ventricle outflow tract obstruction, and sigmoid septum hypertrophy. One month later, patient recovered and transthoracic echocardiography revealed improved heart anatomy and function. To differentiate takotsubo syndrome with other conditions, especially acute coronary syndrome, is crucial. Their clinical presentations are similar but the managements are different. The transthoracic echocardiography holds an important role in supporting the diagnosis of takotsubo syndrome.
Keywords
Introduction
The takotsubo syndrome (TS) is finally diagnosed in 1%–2% of patients previously diagnosed as acute coronary syndrome (ACS). 1 It is increasingly recognized in the field of cardiology due to increased accessibility of coronary angiography in patient present with acute chest pain. The catecholamine surge has been defined as one of the potential causative role of TS. 2 Troponin I level and electrocardiogram (ECG) changes in early presentation are not sufficient to differentiate these two conditions since more than 80% of TS cases have increased troponin I level, and ECG changes resemble ACS. 3 Therefore, coronary angiography, left ventriculography, transthoracic echocardiography (TTE) and, if necessary, cardiac magnetic resonance imaging are needed to fulfill the diagnostic criteria proposed by current guidelines. 4 Although TS is generally considered a benign disease, current observations show that short-term outcome was comparable with ACS treated according to current guidelines. 2 In the long-term follow-up, impaired cardiac function is detected in patients with TS. 5 We herein reported a case of 79-year-old woman presenting with ACS and finally was diagnosed as TS. In the follow-up, the clinical outcome was favorable.
Case report
A 79-year-old woman was referred to the emergency department of our hospital complaining of acute chest pain. The pain occurred 18 h before admission, described as tight, increased with activities, and not relieved with rest. Referred pain, cold sweating, nausea, and dyspnea were denied. The patient visited a district hospital and was diagnosed as anterior ST-elevation acute myocardial infarction (STEMI). She was hospitalized in intensive care unit and medicated with fondaparinux subcutaneous injection 2.5 mg one a day, aspirin oral 80 mg one a day, clopidogrel oral 75 mg one a day, bisoprolol oral 2.5 mg one a day, and captopril oral 12.5 mg total daily dose. Twelve hours later, she developed hypotension (blood pressure (BP) was 70/40 mm Hg and heart rate (HR) was 110 beats/min). The physician gave dobutamine and norepinephrine continuous infusion, and referred the patient to our hospital, which is a tertiary referral for cardiovascular disease in the region.
On admission, physical examination revealed hypotension with BP 90/60 mm Hg, regular HR 120 beats/min, respiratory rate 24 times/min, and axillar temperature 36.8°C. Common coronary risk factor was hypertension and menopause. There was no increase in jugular venous pressure. Cardiac examination revealed grade 3/6 pansystolic murmur at the left lower sternal border. There was no cardiomegaly. Other examinations were within normal limit.
An ECG showed sinus rhythm with symmetrical T-wave inversion in leads V3–V5 and pathologic Q wave in leads V1–V3. Laboratory investigation demonstrated hemoglobin level of 10.3 g/dL, leucocytosis with white blood cells count of 20.03 × 103/µL with 86% neutrophils, platelet count of 308 × 103/µL, creatine kinase (CK) level of 75 U/L, CK-MB of 31 U/L, high sensitive troponin I level of 6182 ng/L, and NT pro-BNP level of 13,349 pg/mL. A chest radiograph showed mild pulmonary edema with normal heart contour.
A TTE was subsequently performed and demonstrated a left atrial dilatation with left atrial volume index (LAVI) 30 mL/m2 and left ventricle (LV) concentric hypertrophy (LVIDd 35 mm, IVSd 12 mm, and LVPWd 12 mm). There were LV systolic dysfunction with LV ejection fraction (LVEF) 46%, severe hypokinetic in apical, and moderate hypokinetic in mid-anterolateral, mid-anteroseptal, mid-inferolateral, and mid-inferoseptal segments (circumferential hypokinetic). It also revealed apical ballooning, systolic anterior motion (SAM) of mitral valves, and hypertrophy of basal septum with LV outflow tract (LVOT) obstruction with peak pressure gradient 106 mm Hg. Figure 1 shows two-dimensional echocardiogram of basal septum hypertrophy and basal hyperkinetic. Severe mitral regurgitation (MR) was found with regurgitant maximum velocity of 5.4 m/s and positive systolic reversal in pulmonary vein (Figure 2). The LV diastolic dysfunction was grade I with E 39 cm/s, e′ 5 cm/s, E/e′ 7.8, DT 229 ms, and E/A 0.6. The right ventricle (RV) systolic function decreased with tricuspid annular plane systolic excursion (TAPSE) value 12 and mild tricuspid regurgitation (TR).

The TTE showed basal septum hypertrophy (PSLAX view; left figure) and basal hyperkinetic (apical 4C view; right figure).
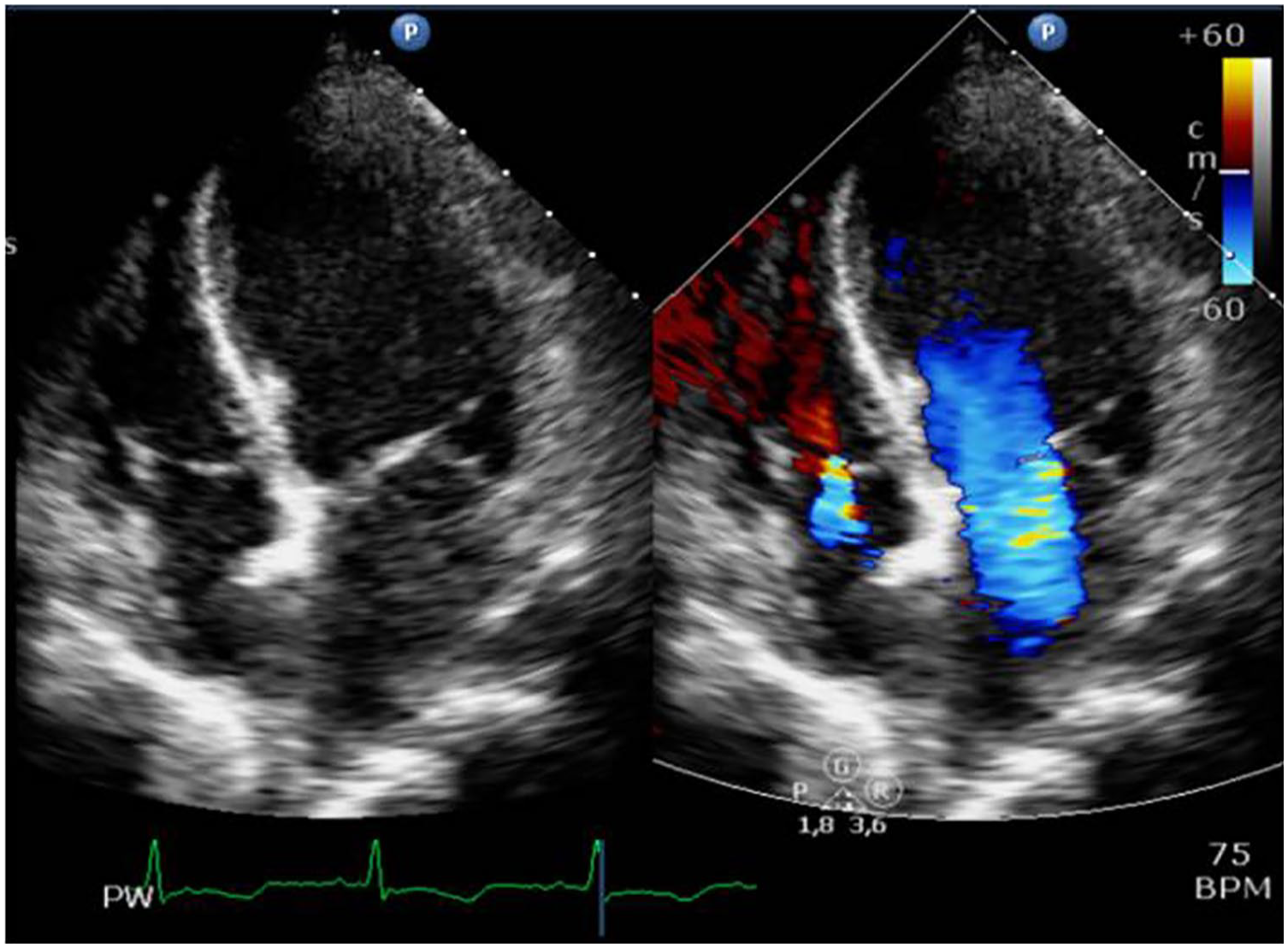
The TTE showed severe mitral regurgitation (apical 4C view; left and right figures).
A diagnosis of anterior STEMI with suspected hypertrophic obstructive cardiomyopathy was made at the time. The clinical suspicion of myocarditis was arised, but because of the TTE results, the myocarditis was less likely diagnosis. The dobutamine and norepinephrine continuous infusion were stopped. We administered intravenous fluid and oral bisoprolol 1.25 mg. The BP was increased to 100/70 mm Hg. Concurrently, we gave fondaparinux injection 2.5 mg one a day, clopidogrel 75 mg one a day, aspirin 80 mg one a day, and atorvastatin 40 mg one a day. The coronary angiography revealed normal coronary arteries. The patient was treated in intensive cardiovascular care unit with uneventful condition.
The TTE evaluation 1 week later showed left atrial dilatation (LAVI 29 mL/m2) with LV concentric remodeling (LVIDd 33 mm, IVSd 10 mm, and LVPWd 8 mm). An LV systolic dysfunction and circumferential hypokinetic remained. There was still apical ballooning but no more SAM and LVOT obstruction. Basal septum hypertrophy decreased with LVOT peak pressure gradient at 82 mm Hg. The patient was discharged from hospital with assessment of TS and given the medication with oral clopidogrel 75 mg one a day, bisoprolol 2.5 mg one a day, captopril 12.5 mg total daily dose, and atorvastatin 40 mg one a day.
One month later, the patient was followed-up and TTE evaluation was performed. We remarkably found significant improvement of heart condition with normal heart chamber (LA diameter 32 mm, LAVI 15 mL/m2, LVIDd 38 mm, RA diameter 27 mm, and RV diameter 23 mm). The LV systolic function was improved with LVEF 77% and normokinetic. There was no apical ballooning, SAM, LVOT obstruction, or sigmoid septum hypertrophy detected by TTE (Figure 3). An RV systolic function was also improved (TAPSE 20 mm). Severe MR was improved into mild MR (Figure 4). The patient remained hemodynamically stable. The patient still routinely visited our hospital outpatient clinics and was doing well after 6 months since hospital discharge.

The TTE showed improvement of systolic anterior motion and basal hyperkinetic (PSLAX view; right and left figures) in 1 month evaluation.

The TTE showed mild mitral regurgitation (PSLAX view; right and left figures) in 1 month evaluation.
Discussion
TS accounts for 0.02% of the whole acute heart disease, with the majority of patients being post-menopausal women. 1 TS is a clinical entity characterized by transient LV wall motion abnormality resembling “takotsubo” or octopus pot. 1 The “takotsubo” appearance of LV by ventriculography was classified as typical variant of TS. 1 Currently, TS has been classified into five anatomical variants: the typical (apical ballooning) variant, mid-ventricular variant, basal or inverted-type variant, biventricular variant, and focal variant. 5
Clinical presentation of TS is mostly similar to ACS. 3 Epidemiological study showed that 1%–2% of suspected ACS patients, finally diagnosed as TS. 1 To differentiate between these two conditions is of paramount importance, since different conditions bring different managements. The current diagnostic criteria of TS (International Takotsubo Diagnostic Criteria (InterTAK Diagnostic Criteria)) help to differentiate those two previous conditions. 4 Our case was initially diagnosed and worked up as STEMI, but eventually TS was an appropriate diagnosis. In our cases, the patient fulfilled six over eight InterTAK Diagnostic Criteria for TS (Table 1).
Diagnostic criteria of TS from International Takotsubo Diagnostic Criteria (InterTAK Diagnostic Criteria). 4

TTE: transthoracic echocardiography; ECG: electrocardiogram.
The TTE is a preferred non-invasive modality to detect the transient and dynamic LV dysfunction and wall motion abnormality in TS. It is a main part of the integrative pathway to build the diagnosis of TS, based on criteria by InterTAK. 4 It is able to assess the LV morphology and function, classify anatomic variant, detect complication, and monitor the LV changes during recovery phase. 6 The key characteristics of TTE in TS is the presence of regional wall motion abnormality (RWMA) over single epicardium Vascularization. 6 One of the TS variant shows RWMA in symmetrical pattern, involving midventricular portion of anterior, inferior, and lateral segment.6,7 The origin of LV RWMA is midventricle asynergy with or without apical involvement. 6 American Society of Echocardiography (ASE) describes the location of LV myocardial dysfunction or RWMA in TS is located in segment 7–12 (midventricle) and 13–17 (apical) of LV walls. 7 Our case had circumferential RWMA pattern with apical akinetic that was appropriate for TS characteristics.
The TTE is a standard imaging modality to detect all dynamic findings in TS, not only to assess the apical ballooning, but also its complication such as SAM, LVOT obstruction, MR, LV thrombus, and RV involvement.8,9 The SAM generally is a temporary condition and will relieve in recovery phase. The SAM and LVOT obstruction are significant markers for complications, such as congestive heart failure, hypotension, and MR. 9 The LVOT obstruction is described as intraventricular gradient ⩾25 mm Hg. Significant LVOT obstruction with peak gradient 20–140 mm Hg has been reported in 10%–25% cases of TS. This phenomena is important to find as it helps us to determine therapeutic decision. Use of inotropic agent and nitrate may exacerbate LVOT obstruction with the consequences of hemodynamic instability, while beta blocker will reduce intraventricular gradient and improve this condition.2,10 In this case, the patient had SAM and LVOT obstruction with severe peak intraventricular gradient. In the presence of LVOT obstruction, intravenous fluids and low dose of short-acting b-adrenergic blockers (i.e. esmolol or metoprolol) may be used with caution to reduce the LVOT obstruction. 2 We had optimized the filling fluid status and gave bisoprolol 1.25 mg in the patient.
MR happens as a result of two mechanisms, tethering and SAM. 9 Transient dilatation of LV will cause tethering of the mitral valves to the apex, causing mitral non coaptation, and finally MR. Study from Izumo et al. 8 found that beside tethering and SAM, there is another independent factor that can cause MR, mitral valves tenting area. Mitral valves tenting area is the main cause of MR caused by ischemic condition (ischemic MR). 9 In such condition, the use of vasodilator and diuretic is contraindication, since it will worsen the SAM, LVOT obstruction, and MR. Herein once again the importance of echocardiography is not only to assess the complications (MR) but also to find pathophysiology to help decide the management. 9 In this case, the patient had severe MR with MR velocity maximum of 5.4 m/s, maximum pressure gradient of 117 mm Hg, and positive systolic reversal in pulmonal veins. But after 1 month evaluation, there is significant improvement to mild MR with MR velocity maximum of 1.4 m/s and maximum PG of 7 mm Hg.
TS with RV involvement was first described in 2006 and occurred in 14.5%–50% from all cases. Citro et al. 10 showed that in patient with biventricular ballooning, RV contraction pattern is a mirror image from left ventricle wall motion abnormality. The patient with RV involvement has lower LVEF and highest TR velocity than the patient who does not. 10 An RV involvement without LV could happen and is defined as isolated RV takotsubo cardiomyopathy.
During TS recovery phase, mild LV dysfunction and other cardiac abnormality may persist.5,11 From the TTE evaluation, improvement of LV wall motion is a common finding, but mild abnormality of regional LV function actually persists and could only be detected with three-dimensional speckle tracking. 11 Our case had significant clinical improvement and parameters of heart anatomy and function, proven by TTE examination. In this case, the patient had SAM with LVOT obstruction, and severe MR and RV systolic dysfunction during hospitalization which were resolved overtime. A significant improvement occurred after 1-month evaluation. The initial LVEF was decreased and gradually normalized during follow-up. The circumferential hypokinetic also became normal to normokinetic.
Conclusion
This case represents acute chest pain as manifestation of TS. The TTE with Doppler examination became the preferred non-invasive imaging modality to suggest the diagnosis of TS. Our case emphasizes the important role of TTE in TS diagnosis and evaluation during recovery phase.
Footnotes
Acknowledgements
Authors acknowledge the echo-lab staffs of Dr Sardjito Hospital for the acquisition of transthoracic echocardiography of this case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent (retrospectively) was obtained from the patient for their anonymized information to be published in this article.