
Abstract
We present a 42-year-old man with acute coronary syndrome with normal coronary arteries and blue toe syndrome secondary to pheochromocytoma. The patient’s medical history included paroxysmal atrial fibrillation and severe hypertension. He complained of weight loss, headache, excessive sweating, palpitations, and anxiety. He had a dry gangrene on the extremity of the left big toe. Pheochromocytoma was confirmed by extremely elevated normetanephrine and metanephrine serum levels (40 and 61 times the upper limit of normal, respectively). Pheochromocytoma was confirmed. An abdominal computed tomography scan showed a voluminous left adrenal mass. Angio-computed tomography-scan of the lower extremities revealed normal arteries. The patient was treated with an alpha-adrenergic blocker, a beta-adrenergic blocker, and a calcium channel blocker. After discontinuation of the treatment by the patient, he presented with constrictive chest pain, blood pressure crisis, and palpitations. The diagnosis of non-ST segment elevation myocardial infarction was made. Coronary angiography revealed normal arteries. Antihypertensive treatment was reintroduced and a left adrenalectomy was performed without incidents. Ten days after surgery, blood pressure, heart rate, and electrocardiogram were normal. There was a significant improvement in the dry gangrene on the left big toe, 4 days after surgery. Pheochromocytoma may present with unusual clinical manifestations such as acute coronary syndrome and peripheral limb ischemia. Timely diagnosis and management of pheochromocytoma are crucial, as the manifestations in this case disappeared after the pheochromocytoma was surgically removed.
Introduction
Pheochromocytoma is a rare catecholamine-secreting tumor that arises from chromaffin tissues of the adrenal medulla. 1 Its clinical presentations are heterogeneous ranging from mildly symptomatic forms to acute cardiovascular events. The excessive release of catecholamines is commonly expressed by paroxysmal or sustained hypertension, headache, and palpitations. 2 Circulating catecholamines exert profound systemic effects through overstimulation of adrenergic receptors, particularly α-adrenergic and β-adrenergic subtypes. One of the most clinically significant cardiovascular complications of pheochromocytoma is myocardial infarction in the absence of overt atherosclerotic coronary artery disease, frequently attributable to intense, transient coronary vasospasm. During catecholamine surges, profound vasoconstriction reduces coronary blood flow to critical levels, resulting in myocardial ischemia. Repeated or sustained episodes of vasospasm can progress to myocardial infarction via prolonged ischemia; even in angiographically normal coronary arteries. 3 Acute myocardial infarction has rarely been reported in literature and its actual incidence among pheochromocytoma patients remains to be determined by large-scale studies. 3 Catecholamine-induced cardiomyopathy in general was identified in 58% of autopsy in patients with pheochromocytoma. 4 Its prevalence varies between 8% and 11%. 5
Peripheral critical chronic ischemia is an uncommon manifestation of pheochromocytoma. 6 Rare cardiovascular manifestations pose significant diagnostic challenges in pheochromocytoma, often leading to misdiagnosis or delayed recognition due to their overlap with more common cardiac conditions.
Herein, we report the case of a 42-year-old man presenting an acute coronary syndrome with normal coronary arteries and a blue toe syndrome that were finally attributed to pheochromocytoma.
Case presentation
A 42-year-old man was referred to the Department of Endocrinology for severe hypertension. His medical history included paroxysmal atrial fibrillation and hypertension, diagnosed 2 years earlier. The patient was taking vitamin K antagonists and amiodarone for the arrhythmia. He complained of weight loss, headache, excessive sweating, palpitations, and anxiety.
On physical examination, he had a body weight of 70 kg, a height of 170 cm with a body mass index of 24.2 kg/m2, a blood pressure of 170/100 mmHg without orthostatic hypotension, and a heart rate of 80 beats/min. Thyroid examination and cardio-pulmonary auscultation were normal. Peripheral pulses were present and symmetrical. There were no clinical signs of heart failure. The patient had a dry gangrene on the extremity of the left big toe with no signs of inflammation (Figure 1(a)). He had no history of trauma and no identified thromboembolic risk factors.
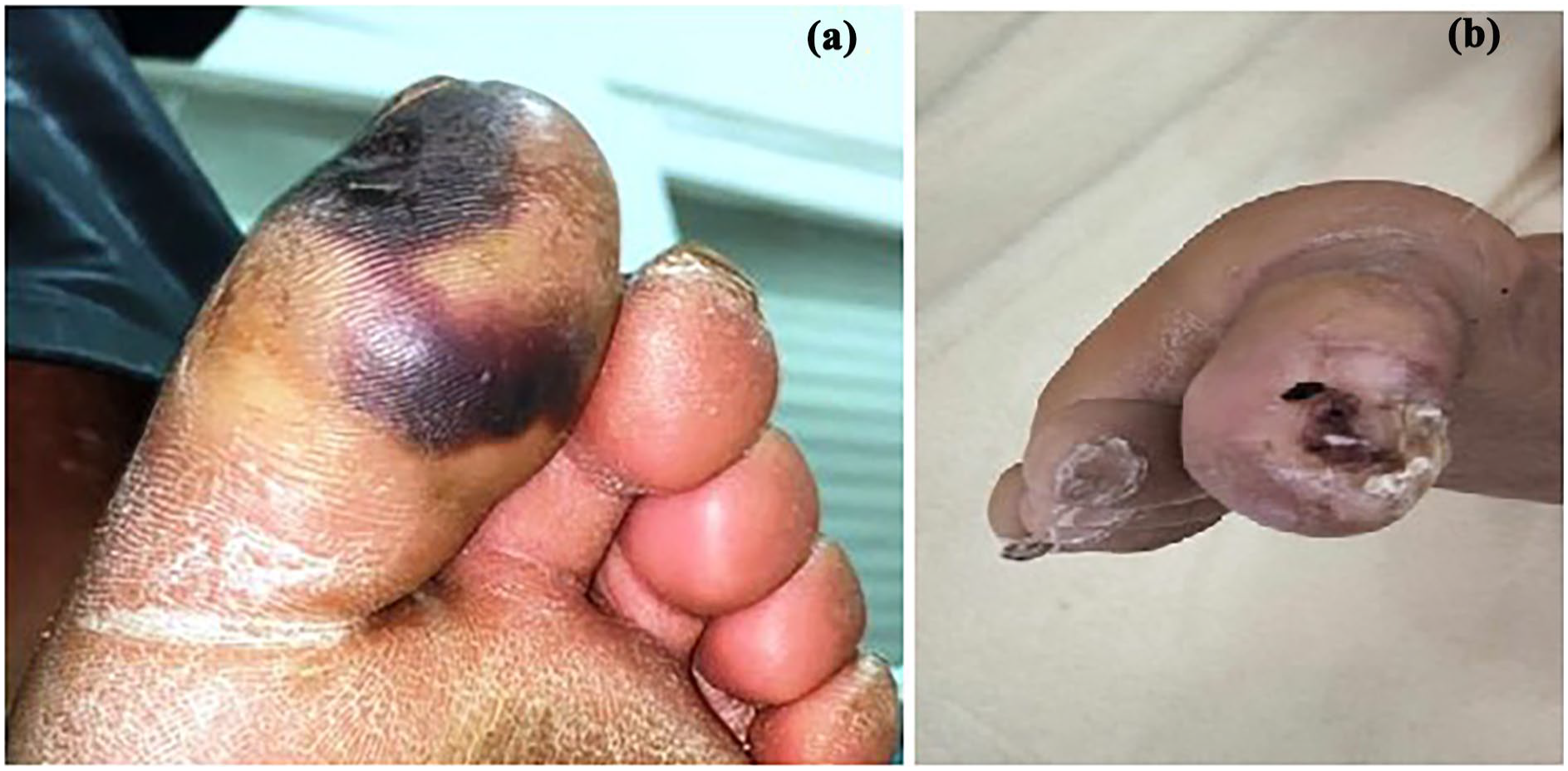
Dry gangrene on left big toe before (a) and after (b) surgery.
The electrocardiogram showed a normal heart rate at 85 beats/min, left ventricular hypertrophy, and inversed T-waves in the antero-septal leads (Figure 2(a)). Cardiac ultrasound showed concentric left ventricular hypertrophy with a preserved ejection fraction at 62%, no valvulopathies, and no evidence of intra-atrial thrombus. Fundoscopic exam did not reveal any signs of hypertensive retinopathy. Troponin levels were 22 ng/mL (normal < 34 ng/mL). The results of biological investigations are shown in Table 1. The diagnosis of clinically suspected pheochromocytoma was confirmed by high levels of plasmatic normetanephrines and metanephrines at 40 and 61 times the upper limit of normal, respectively. Abdominal computed tomography (CT) scan showed a well-limited left adrenal mass measuring 92 × 72 mm with heterogeneous contrast enhancement (Figure 3). Angio-CT-scan of the lower extremities revealed normal lower limb arteries.
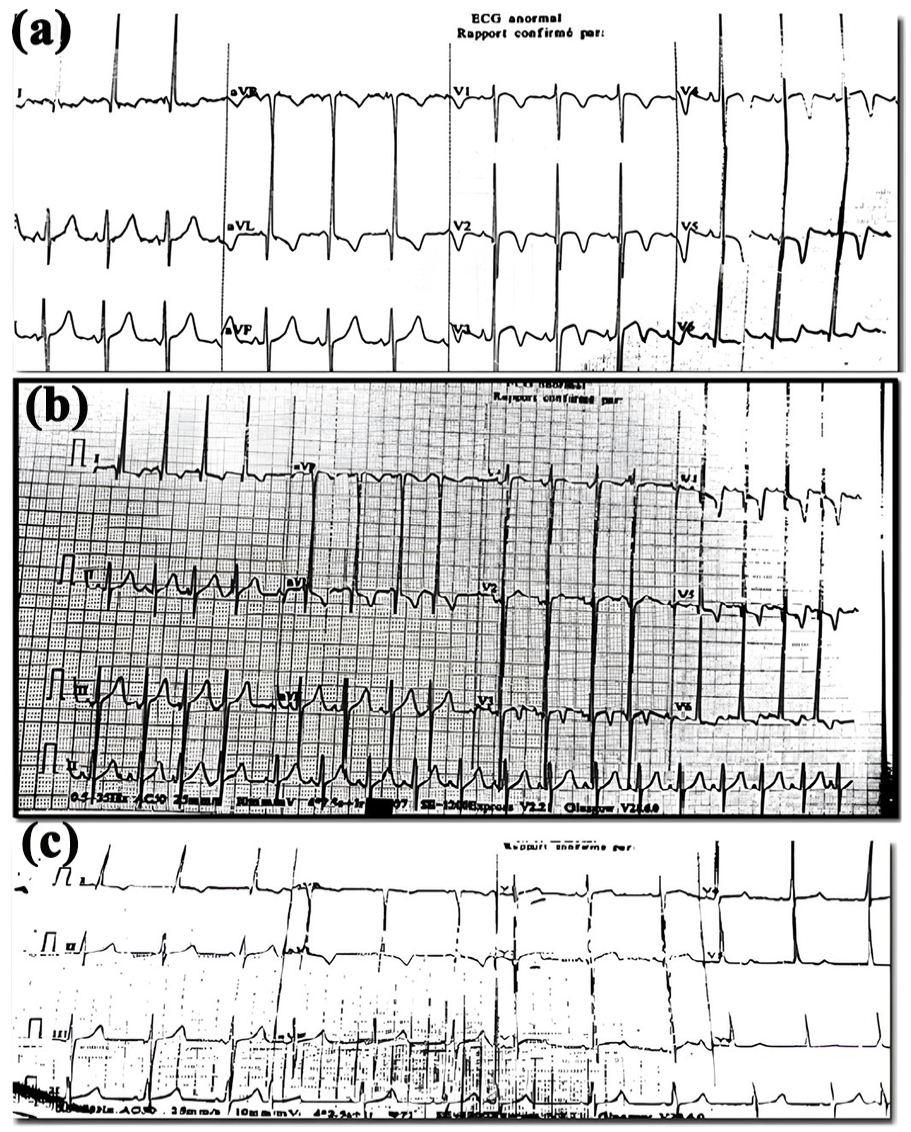
Patient’ s ECG: (a) ECG at baseline, (b) ECG during adrenal crisis, and (c) ECG after adrenalectomy.
Laboratory blood investigations.

HDL: high-density lipoprotein; TSH: thyroid stimulating hormone; PTH: parathormone.

Abdominal CT scan showed a well-limited left adrenal mass measuring 88 × 73 mm, with heterogeneous contrast enhancement.
The patient was treated with a progressively increasing dose of the alpha-adrenergic blocker prazosin, up to 15 mg per day, along with a normal-sodium diet and oral hydration (3 L/day). Then, a nonselective beta-adrenergic blocker (propranolol 20 mg three times per day) and a calcium channel blocker (amlodipine 10 mg/day) were added. The patient’s blood pressure and heart rate were well controlled. After appropriate medical preparation, the patient was discharged from the Department of Endocrinology and referred to the surgery department for a surgical treatment of his pheochromocytoma. However, he presented with an acute hypertensive crisis (blood pressure: 200/100 mmHg) with constrictive chest pain and palpitations secondary to the nonadherence to antihypertensive treatment. An electrocardiogram revealed sinus tachycardia at 120 beats/min with ST-segment depression in anteroseptal and lateral leads (Figure 2(b)). Troponin levels were high (1038 ng/mL) and increased within a 3-h interval, reaching 1623 ng/Ml (73 times more than the initial troponin level). Thus, the diagnosis of a non-ST segment elevation myocardial infarction was made. Coronary angiography revealed normal arteries (Figure 4).

Patient’s coronary angiography showed normal coronary arteries.
Antihypertensive drugs were reintroduced. The patient had no complaints and his blood pressure and heart rate were normal. After appropriate medical preparation, a left adrenalectomy was performed without any incident. Pathological examination showed a pheochromocytoma with a PASS (Pheochromocytoma of the Adrenal gland Scaled Score) of 1. After surgery, antihypertensive drugs were discontinued. A 24-h blood pressure monitoring was performed 10 days later, showing normal mean blood pressure levels (113/67 mmHg during the day, 102/59 mmHg during the night) with no paroxysms. The patient did not complain any further chest pain or palpitations. His electrocardiogram was normal (Figure 2(c)). In addition, there was significant improvement in the dry gangrene on the left big toe 4 days after the surgery (Figure 1(b)). However, the patient was lost to follow-up.
Figure 5 represents the treatment-symptom resolution relationship.
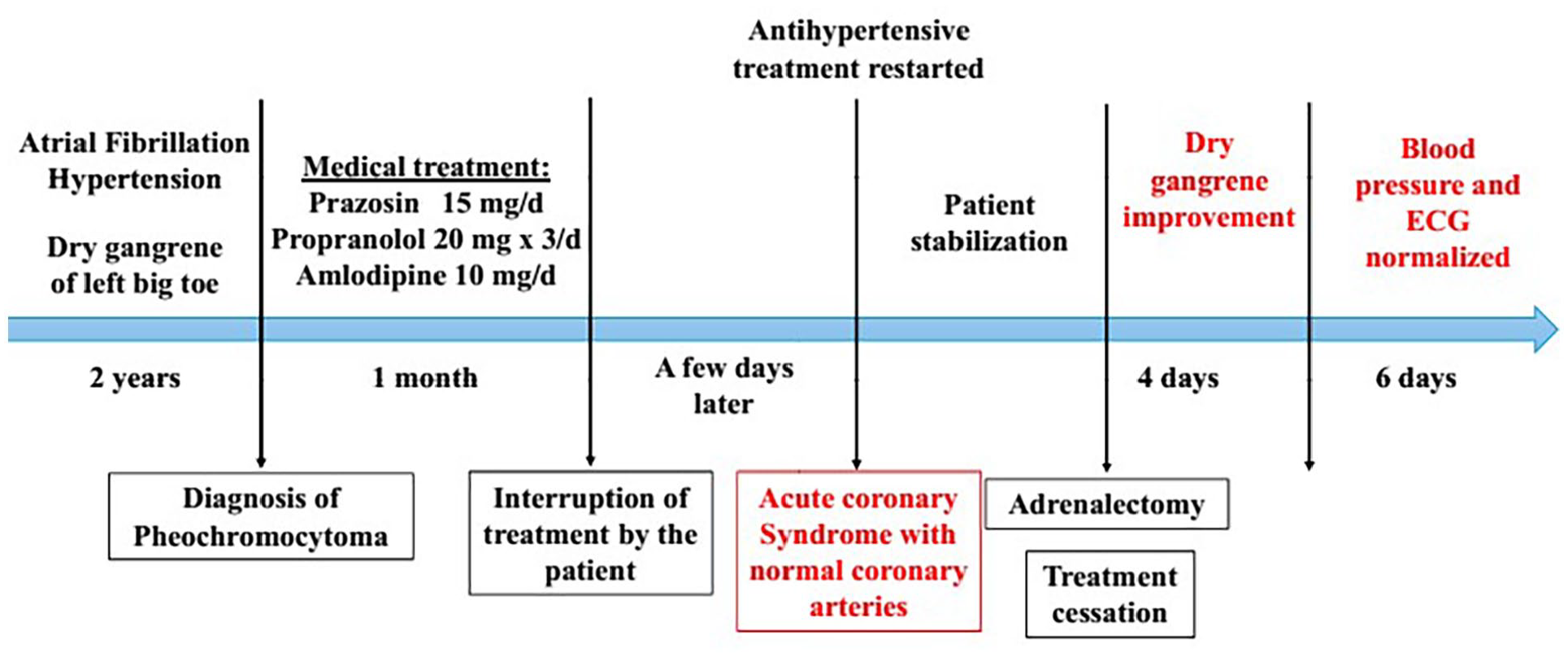
Timeline of the symptom-treatment relationship.
The reporting of this case conforms to the CARE guidelines. 7 A written informed consent was obtained from the patient for treatment and for the publication of this case report. Ethical approval for this case report was not required because of the retrospective nature of the study.
Discussion
Pheochromocytomas are reported to be the cause of secondary hypertension in approximately 0.1%–0.6% of hypertensive patients. 8 Hypertension represents the most common manifestation of pheochromocytoma, occurring in about 80%–90% of cases. 9 Catecholamines elevate blood pressure through three mechanisms: peripheral vasoconstriction secondary to the stimulation of postsynaptic α1-receptors, inotropic and chronotropic effects by stimulation of postsynaptic ß-receptors, and secondary hyperaldosteronism. Patients may exhibit sustained hypertension, paroxysmal hypertension, or sustained hypertension with paroxysms, determined by the specific type of catecholamine released by the tumor. 10 In addition to hypertension, activation of α- and β-adrenergic receptors can cause vasoconstriction of the coronary arteries and have positive inotropic effects on the heart resulting in tachyarrhythmia. 9 Cardiac arrhythmia and heart failure with dilated cardiomyopathy are known complications of prolonged exposure to excessive catecholamines.11,12 However, acute coronary syndrome has only been reported in a few cases.3,13–20 Myocardial ischemia in pheochromocytoma can result from two mechanisms: reduced coronary artery perfusion due to coronary vasospasm and increased myocardial oxygen consumption due to tachycardia and hypertensive cardiomyopathy.3,9,21 Clinical presentations varied from isolated paroxysmal chest pain to acute heart failure complicated with cardiogenic shock. Electrocardiographic findings varied significantly from ST-segment depression with deep T-wave inversion to ST-segment elevation with the presence of Q waves. In previously reported cases, echocardiogram showed various abnormalities including segmental wall motion hypokinesis, concentric left ventricular hypertrophy, and mild-to-severe left ventricular systolic dysfunction.11,19 Our patient had acute constrictive chest pain, elevated blood pressure, and palpitations. His electrocardiogram showed new onset abnormalities and he had high myocardial injury markers. However, coronary angiography did not show occlusion of coronary arteries. Thus, acute coronary syndrome was attributed to vasospasm of coronary arteries secondary to pheochromocytoma after treatment discontinuation.
The understanding of acute coronary syndrome related to pheochromocytoma is still incomplete and management guidelines are lacking. Although beta-blockers are usually recommended in acute coronary syndrome, they can aggravate cardiac manifestations in patients with pheochromocytoma causing high hypertensive peaks and increasing the severity of cardiac crisis if prescribed without α-blockers.21,22
In addition to the acute coronary syndrome, our patient had ischemic gangrene of his left big toe that was also attributed to vascular spasms induced by normetanephrine release. Gangrene of any part of the feet is a manifestation of limb-ischemia. 23 The most common cause of chronic limb-ischemia is atherosclerosis, followed by cardiac embolism due to arterial fibrillation. 24 In the case of pheochromocytoma, arrhythmia was described in three cases as the cause of acute limb ischemia.25,26 Our patient indeed had paroxysmal atrial fibrillation. However, there was no evidence of an intracardiac thrombus and his angio-CT-scan showed no signs of intravascular obstruction, which further suggests the role of intense distal vasoconstriction and vasospasm caused by excess catecholamine release. 27 According to a brief case report and literature review by Lutchman et al., 6 this phenomenon has been described in 12 cases. Most of these patients were middle-aged women with unilateral pheochromocytoma. Another patient with confirmed pheochromocytoma was reported to have a narrowing of the popliteal arteries by diffuse spasms on angiography. 28 This vasoconstrictive effect induced by catecholamines can be severe and may lead in some cases to progressive acral ischemia of the four limbs, then to amputation.6,29 Unfortunately, this symptom can be easily overlooked when the patient does not have any symptoms suggestive of pheochromocytoma.
Managing acute coronary syndrome in patients with pheochromocytoma involves addressing both the cardiovascular complications and the underlying catecholamine-secreting tumor by adrenalectomy after appropriate medical preparation by alpha-blockers then beta-blockers. Alpha-blockers aim to prevent intraoperative hemodynamic instability during resection of pheochromocytoma.30,31 Additionally, beta-blockers are prescribed to control heart rate after sufficient alpha blockade. In fact, blocking beta-receptors without concurrently blocking alpha receptors can lead to severe hypertension due to unopposed alpha-adrenergic receptor activity. While beta-blockers are generally beneficial in managing acute coronary syndrome, they can be contraindicated in certain scenarios, particularly in hemodynamically unstable patients and the early stages of myocardial infarction. The primary concern is the risk of cardiogenic shock. 32 Calcium channel blockers can be added in case of persistent uncontrolled hypertension. 31 Moreover, it is important to ensure adequate volume expansion to counteract the vasodilatory effects of alpha-blockade and prevent hypotension during surgery. 33 In cases where atherosclerotic coronary syndrome is present, cardiac revascularization under alpha-blockade before tumor resection was performed in one case report to minimize peri-operative risks. 34 Once the patient is stabilized, it is safe to proceed with resection of the adrenal mass. Peroperative management includes continuous blood pressure and cardiac output and use of other molecules like remifentanil and diltiazem to manage blood pressure fluctuations. 35 Postoperative care should include monitoring for vasoplegia and cardiogenic shock. Mechanical circulatory support may be necessary in severe cases. 33 Regular follow-up to monitor for recurrence and manage any residual cardiovascular issues is recommended. 15
After the stabilization of hypertension and heart rate under these drugs, our patient underwent surgery with no complications. Within 10 days of the surgery, blood pressure levels normalized without the use of any drug and electrocardiogram abnormalities disappeared. In addition, significant improvement of the dry gangrene of the left big toe was noted. However, our patient was lost to follow-up.
Among the few cases of acute coronary syndrome described in the literature, hypertension subsided for all patients, giving way to normal blood pressure levels, as well as completely normal electrocardiogram after surgery.3,13,15,19 As for the peripheral chronic ischemia, all cases except for one showed a significant decrease in the necrosis areas after a period varying from 24 h to 3 months after surgery.6,29,36
The present case underlines the importance of an early diagnosis of pheochromocytoma, and helps identify the clinical pearls for the recognition of atypical manifestations, such as myocardial infarction and arrhythmia in young patients without cardiovascular risk factors with normal coronary angiography findings, and peripheral severe ischemia with no history or evidence of atherosclerotic disease. However, this was a single case report which inherently limits the generalizability of its findings to the broader population. Thus, conclusions must be interpreted with caution. Additionally, the absence of long-term follow-up precludes assessment of sustained cardiovascular outcomes. Furthermore, no genetic testing was conducted to explore potential underlying hereditary syndromes which may have implications for patient surveillance and family screening. These limitations underscore the need for larger studies and comprehensive genetic evaluation in similar clinical presentations.
Conclusion
In the present case, pheochromocytoma manifested with severe hypertension, paroxysmal atrial fibrillation, myocardial infarction caused by coronary vasospasm, and peripheral limb ischemia caused by extreme vasoconstriction. Early diagnosis and management of pheochromocytoma are essential since these manifestations disappeared after the pheochromocytoma was removed.
Footnotes
Acknowledgements
We would like to express our deepest gratitude to our colleagues from the departments of Radiology, Cardiology, Cardiovascular Surgery, and Urology of La Rabta University Hospital for their invaluable assistance in managing the patient.
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Written informed consent was obtained from the patient for anonymized information to be published in this article.
Author contributions
IO: conception and design, acquisition, analysis, and interpretation of data, manuscript creation and drafting; MM: acquisition, analysis, and interpretation of data, manuscript creation and drafting; FC, AT, MY, and MC: acquisition, analysis, and interpretation of data; MC: revising the manuscript critically for important intellectual content; all authors were involved in the management of the patient and the revision of the manuscript, and approved the final version.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing is not applicable—no new data was generated.