
Abstract
Some patients presenting with acute coronary syndrome may have had nonobstructive coronary arteries. Nevertheless, a lot of people are not aware that, as of the fourth universal definition of myocardial infarction, Takotsubo syndrome is no longer categorized as myocardial infarction with non-obstructive coronary arteies group. This can lead to diagnostic delays, the use of unnecessary examination, and harmful medical intervention. We present a 68-year-old woman with typical chest pain for 6 h. She had a history of hypertension, transient ischemic attack, and diabetes mellitus. She was diagnosed first with acute coronary syndrome but was later found to have takotsubo syndrome, based on high international takotsubo diagnostic score and transthoracic echocardiography findings of systolic apical ballooning. Within 5 days, she makes a gradual recovery.
Introduction
Takotsubo syndrome (TTS) is characterized by a temporary impairment of the left ventricle resembling a traditional Japanese octopus’s trap and shares certain similarities with acute coronary syndrome (ACS) (similar symptoms, electrocardiogram (ECG) abnormality, elevated cardiac biomarker, and comparable in-hospital mortality). Nevertheless, coronary angiography reveals that the coronary arteries are typically, but not always, normal. Consequently, this syndrome has often been misclassified as being part of the MINOCA category despite the presence of distinct etiological and histological characteristics. To date, a challenge persists in the differentiation of TTS and ACS.1,2
Case presentation
A 68-year-old anxious woman with a history of hypertension, transient ischemic attack, and type-2 diabetes presented with persistent, non-radiating, and pressing left-side chest pain for 6 h prior admission. She confessed that she was experiencing significant stress due to her intense longing for a family member. Vital signs were in normal limits and her ECG revealed a multisite ST-segment elevation (Figure 1). She was hypoglycemic (plasma glucose 62 mg/dL), with elevated levels of cardiac troponin-I (5.36 ng/dL; normal value 3.42 ng/dL) and NT-proBNP (9288 pg/mL; normal value 125 pg/mL). Coronary angiography, however, revealed normal coronary artery. Echocardiography uncovered a left ventricle (LV) apical ballooning and mid-range ejection fraction (LVEF 48% BIPLANE Simpson; Figure 2(a)). Strain imaging using speckle tracking echocardiography displayed a hypokinetic LV apex (Figure 2(b)). Her signs and symptoms gradually improved, followed by a recuperated troponin-I and LV apical hypokinesis (LVEF 62% Simpson BIPLANE) on day 2 of admission (Figure 2(c) and (d)). She was discharged on the fifth day with physical activity restrictions.
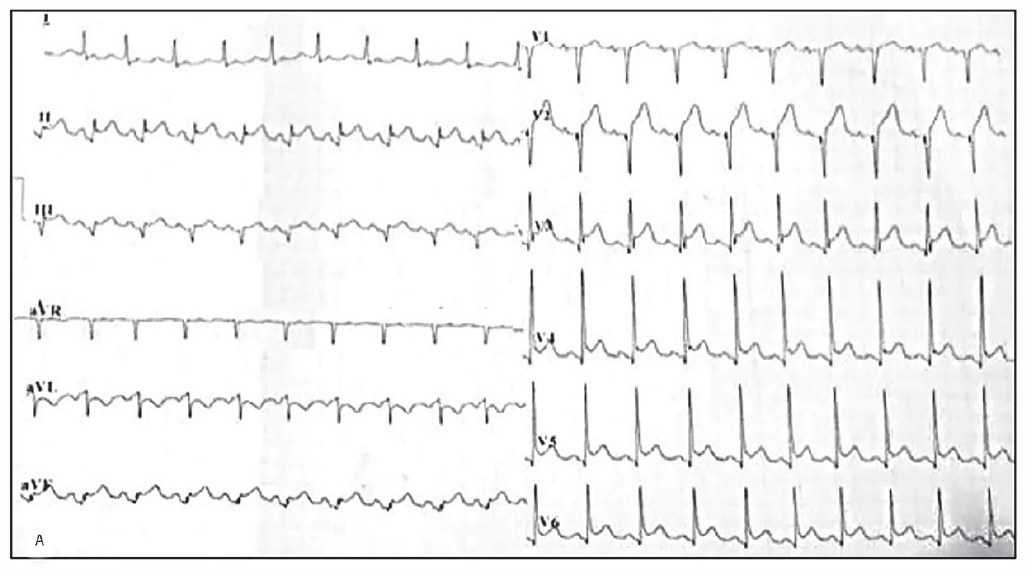
ECG revealed sinus rhythm, ST-segment elevation in inferior extremity lead (lead II, III, aVF) and anterior precordial lead (lead v2-v6), and ST-segment depression at lead I, aVL.

(a) On the first day, the echocardiography demonstrated LV apical ballooning on four chamber view. (b) Two-dimensional speckle tracking bull’s eye patterns of LV Global longitudinal strain (GLS) illustrate apical hypokinesia at diagnosis. (c) On the second day, the echocardiography results indicated a noteworthy improvement in left ventricular motion. (d) The bull’s eye patterns of LV GLS, tracked through two-dimensions of speckles tacking, demonstrate a noteworthy improvement within a span of 2 days.
Discussion
TTS, also known as neurogenic stunned myocardium or acute cardiac sympathetic disruption syndrome, is an acute stress-induced inflammatory condition of the heart. 3 The disease has predilection for elderly menopausal women and there is often an adrenaline-related precipitant (emotional stress, major physical illness, administration of catecholamines, or of antidepressants which inhibit catecholamine reuptake). 1 Other distinguishing features are disproportionate elevation of NTproBNP concentrations, multisite ST-elevation, left and right ventricular hypokinesis not corresponding to distribution of a particular coronary artery, and absence of infarction (presence of edema) on cardiac MRI. 2
A considerable number of patients exhibit initial hypotension, which cannot be solely attributed to a decrease in cardiac output. The initial hemodynamic instability is influenced by the acute impairment of the coronary micro vessels. This impairment is characterized by the damage to the endothelial glycocalyx, which leads to an elevation in vascular permeability and subsequently results in a decrease in blood pressure. 4 Additionally, there is an observed augmentation in tissue sensitivity to nitric oxide and the subsequent formation of peroxynitrite, which potentially plays a role in the decline of blood pressure. 5
TTS therapy, which differs from ischemic (e.g. myocardial infarction) origins, can be fatal for patients, with a 20% mortality rate for unstable TTS patients treated with catecholamines. 2 According to expert consensus, mechanical approaches such as extracorporeal membrane oxygenation, temporary left ventricular assist devices, and intra-aortic balloon counter pulsation have been identified as viable options for managing cardiogenic shock in TTS patients. Nevertheless, it is crucial to identify left ventricular outflow obstruction, due to the potential worsening of hemodynamic status when intra-aortic balloon counter pulsation is employed in these cases. In certain countries, the utilization of low-dose levosimendan is observed as a positive inotrope that acts as a Ca2+-sensitizer. 2 Some evidence suggests that patients should be administered ACE inhibitors or ARB to facilitate LV recovery and improve patient survival, but controlled studies are awaited. 2 Several complications, including atrial fibrillation, low ejection fraction, and low glomerular filtration rate, have been recognized as independent predictors of adverse events. 6
The process of recovery typically occurs gradually, characterized by persistent fatigue and heart failure despite an improvement in LVEF. Additionally, certain patients may experience the development of myocardial fibrosis as the inflammation in the myocardium subsides.2,7
The common theory regarding the pathophysiology of TTS is the occurrence of an endogenous adrenergic surge. This hypothesis is supported by the notable association between the disease and instances of sudden and intense stress, as well as severe physical illness or trauma. 8 It was found that the catecholamine and stress-related neuropeptide levels were higher in 13 TTS patients who were affected by emotional stress compared to 7 patients who had myocardial infarction and Killip class III. 9 An additional rationale for the higher occurrence in the postmenopausal female population can be attributed to the diminished levels of estradiol, a significant hormone that minimizes catecholamine-induced vasoconstriction and reduces the sympathetic response to psychological stress.1,10
Because coronary angiography frequently reveals normal coronary arteries, TTS is frequently confused with MINOCA. TTS differs from MINOCA etiologically and histologically. In ischemic pattern the cells die in an atonic state without myofibrillar damage. Conversely, the TTS biopsy revealed that cells die in a hypercontracted state along with early myofibrillar damage and irregular cross-band formations. Furthermore, TTS lesion areas are located at the ends of intracardiac nerves, as opposed to MINOCA, which may involve a significant decrease in coronary blood flow. 11 TTS typically exhibit multisite ST-segment elevation, without clear localization to a specific territory. 8 In addition, it should be noted that troponin levels are typically elevated in TTS, albeit with lower peak value compared to those observed in ischemic origins. 2
In the acute phase, two evaluations can be used quickly to differentiate between MINOCA and TTS. First, echocardiography can determine whether abnormal regional wall motion abnormality matches coronary perfusion. If so, a coronary examination could be performed using intravascular imaging (optical coherence tomography or intravascular ultrasound) for detection of thrombus, plaque rupture or erosion, or spontaneous coronary artery dissection, and a provocation test when coronary or microvascular spasm is suspected.7,12 As in our case, TTS is more likely because it does not match coronary perfusion. Second, the international takotsubo (InterTAK) diagnostic score can be used, as in our case there are risk factors for females: emotional stress (longing for her family member), physical trigger (hypoglycemia), and psychological disorder (anxiety), resulting in a total score of 73, indicating a >91.7% probability of TTS.1,2,13
In contrast, distinguishing TTS from myocarditis is more challenging since the two diseases are not mutually exclusive and have comparable examination characteristics. Acute myocarditis does not exclude TTS; rather, it may be an essential histopathologic feature (catecholamine myocarditis) of the syndrome in some patients. Furthermore, acute infectious myocarditis may induce TTS in a manner like that of sepsis and other physical stressors. 3 TTS, myocarditis, and MINOCA can be distinguished by cardiac magnetic resonance (CMR). 14 CMR cannot be utilized easily in the acute phase of TTS, but is greatly useful in the subacute phase. 2 CMR can be used in TTS patients in the acute phase when echocardiographic images are suboptimal, there is an atypical presentation of TTS (mid-ventricular, basal, and focal wall motion patterns), or there are “red flags” of infectious myocarditis (signs of viral infections, elevated erythrocyte sedimentation rate and/or c-reactive protein, and pericardial effusion).2,7
In the subacute phase, CMR is required within 1 month of TTS onset in all patients without an identifiable trigger event or in the event of incomplete recovery (persistent ECG alterations and/or abnormal wall motion on echocardiography).2,7 In CMR, ischemic pattern may be indicated by subendocardial or transmural late gadolinium enhancement (LGE) and myocarditis may be indicated by subepicardial LGE, whereas TTS is characterized by the absence of relevant LGE, the presence of reversible tissue injury (edema), and specific wall motion abnormalities (apical, mid-ventricular, or basal ballooning).2,12,14 CMR provides an important information on MINOCA which can give 74% MINOCA patients a definitive diagnosis. The population of patients with MI generally exhibited an older age demographic, which may overlap with the TTS population. CMR has been shown to provide a significant diagnostic value, playing a crucial role in the diagnosis of this condition. 15
The conclusive differential diagnosis between TTS and ACS necessitates the implementation of coronary angiography, which is carried out in the setting of all STEMI and high-risk to very high-risk NSTEMI manifestations. When there is a suspicion of TTS accompanied by significant obstruction, it is imperative to conduct a thorough analysis of coronary angiography and ventriculography in comparable views to identify any perfusion–contraction mismatch.2,7 It is important to acknowledge that the presence of obstructive coronary stenosis should not be considered an absolute exclusion criterion for TTS. However, if there is evidence of coronary artery disease, it may not be adequate to account for the observed regional wall motion abnormalities.
In our case, we did not perform left ventriculography because the echocardiography clearly revealed apical ballooning, and the global longitudinal strain (GLS) supported apical hypokinetics with an InterTak score of 73. We also considered MRI in the subacute phase 2 months later. However, when the echocardiography evaluation on day 2 confirmed the reversibility of apical hypokinetic, we did not perform an MRI as recommended by the TTS diagnostic algorithm. 2 This case has a limitation, as we did not follow up with the patient to assess her recovery progress, nor did she undergo CMR.
Conclusion
In the present study, we presented a case involving a postmenopausal female who initially exhibited clinical similarities to a patient experiencing ACS. However, subsequent findings revealed that the patient actually had TTS, as indicated by a high diagnostic score according to the InterTAK diagnostic criteria and echocardiography results showing systolic apical ballooning and reversible myocardial dysfunction. It is imperative to distinguish between these two conditions, as they not only stem from distinct pathophysiological, etiological, and histological origins but also necessitate distinct treatment approaches, particularly in individuals experiencing hypotension.
Footnotes
Acknowledgements
None.
Author contributions
M.Y.A. contributed to the concept and critically reviewed the article; T.T.E.L. and R.I.G. contributed to the concept and collected the patient information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.