
Abstract
A 61-year-old elderly male, hypertensive patient presented to the retina clinic with sudden drop in vision in the left eye for 6 days. His best-corrected visual acuity at presentation was counting fingers close to face. Fundus examination of the left eye revealed the presence of subretinal and preretinal haemorrhage at the macula along with hypertensive retinopathy changes in both eyes. Fluorescein angiography was done, which showed a retinal artery macroaneurysm at the optic nerve head. Optical coherence tomogram through the optic nerve head also confirmed the presence of retinal artery macroaneurysm. The patient was treated with injection of 0.4 cc of 100% C3F8 to displace the blood off the macula. At final follow-up visit at 2 months post treatment, his vision improved to 6/12, N8. Fundus examination showed a small residual altered blood nasal to the fovea. No treatment was however done to the retinal artery macroaneurysm due to its atypical location and chance of spontaneous involution. In conclusion, retinal artery macroaneurysm at the optic disc is extremely uncommon. Identification of the retinal artery macroaneurysm lesion is more difficult in glaucoma patients due to the large and deep optic cup. Fluorescein angiography remains the main investigative modality to confirm the diagnosis. Spontaneous involution still remains the mainstay of treatment in optic disc retinal artery macroaneurysm.
Introduction
Retinal artery macroaneurysm (RAM) usually occurs in elderly females associated with vascular problems such as hypertension and general arteriosclerotic cardiovascular disease. 1 RAMs are commonly observed along the first- or second-order retinal arterioles, but can rarely be observed on or near the optic nerve head (ONH).2–5 There are very few published reports in literature describing RAM at the papillary or peripapillary location. We present a rare case of ruptured ONH RAM in an elderly hypertensive patient with primary open-angle glaucoma (POAG).
Case presentation
A 61-year-old elderly male was referred by a local ophthalmologist to the retina clinic of a tertiary eye hospital with a history of sudden drop in vision in the left eye (LE) for 6 days. On passing through the patient’s documents, the local ophthalmologist had noted the presence of preretinal heme obscuring the ONH. He was recently diagnosed with non-insulin-dependent diabetes mellitus for 1 year. His blood pressure on presentation was recorded at 180/100 mm Hg, and he was started on anti-hypertensive medications. On examination, his best-corrected visual acuity (BCVA) was counting fingers close to face in both eyes (BE). Intraocular pressure (IOP) measurement using the Goldmann Applanation tonometer was 14 and 16 mm Hg in the right eye (RE) and LE, respectively. Gonioscopy revealed open angles in BE. Anterior segment examination of BE was normal. A dense nuclear cataract with post-subcapsular cataract was noted in the RE. Fundus examination of the RE revealed a hazy media with a cup:disc ratio (CDR) of 0.8:1. Other finer details of the fundus were not appreciated clearly due to dense cataract. LE was pseudophakic with a posterior chamber intraocular lens. LE fundus examination showed a clear media with CDR of 0.8:1, dilated retinal vessels and AV crossing changes, and cotton-wool spots suggestive of hypertensive retinopathy. Multiple layered preretinal and subretinal blood was surrounding the optic disc and macula (Figure 1). Fluorescein angiography (FA) was done to identify the source of heme in the retina. FA revealed blocked retinal and choroidal fluorescence due to the presence of the overlying preretinal and subretinal haemorrhage in the LE. A small focus of light-bulb hyperfluorescent lesion at the centre of the ONH corresponding to the macroaneurysm was noted in the progressive phases of the FA (Figure 2). RE showed an old inferotemporal vascular occlusion with areas of capillary non-perfusion along the inferotemporal quadrant and involving the macula as well. A diagnosis of ONH RAM with fresh premacular and submacular haemorrhage in a hypertensive patient was made in the LE. In view of the dense cataract in the RE and a co-existent retinal pathology in the LE, the patient was advised simultaneous cataract surgery in the RE and intravitreal 0.4 cc of 100% perfluoropropane (C3F8) gas injection with prone positioning in the LE after lowering the IOP with anterior chamber paracentesis. One week post treatment, his BCVA in BE was counting fingers at 3 m. LE fundus examination showed a resolved preretinal haemorrhage and altered subretinal haemorrhage with a residual gas bubble. At 3-week follow-up, his LE BCVA improved to 6/18, N6. LE fundus examination showed resolving retinal and subretinal haemorrhage (Figure 3). Optical coherence tomography (OCT) of the LE through the macula showed a normal foveal contour and a thin layer of subretinal blood with shadowing nasal to the fovea. High-definition OCT images (Zeiss Cirrus HD OCT-500) of the left ONH identified a bulbous lesion in continuation with the retinal vessel sitting within the ONH. This lesion corresponded to the hyperfluorescent lesion seen on the ONH head on FA. We believe this lesion could be the possible ONH RAM (Figure 4). RE BCVA was counting fingers at 3 m. FA revealed an inferotemporal retinal vein occlusion with macular ischaemia in the RE. Fundus examination at 2 months post treatment revealed a small residual altered subretinal bleed in the LE. His BCVA in the LE improved to 6/12, N8 (Figure 5). Written consent was obtained from the patient for the usage of data and images for this report. Institutional review board approval was taken for this particular case report (SCEH/17/005).

Colour fundus (CF) images of both eyes at the time of presentation: (a) CF of the right eye showing a glaucomatous disc and hazy media secondary to cataract and (b) CF of the left eye showing an optic disc with high cup:disc ratio of 0.8:1 and presence of preretinal and subretinal haemorrhage at the macula and inferior to the disc and presence of AV crossing changes, arteriolar attenuation, and cotton-wool spots.
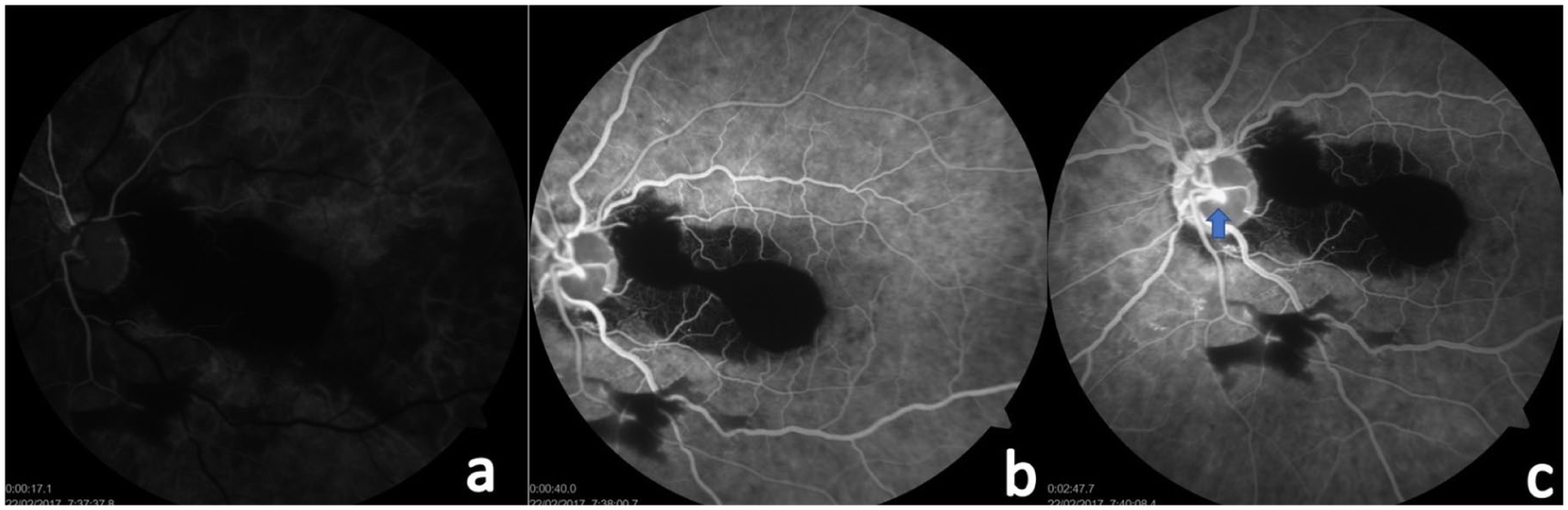
Fluorescein angiography (FA) images of the left eye at presentation: (a)–(c) FA images showing blocked fluorescence at the macula due to presence of preretinal and subretinal heme. Also seen is a light-bulb hyperfluorescent lesion deep at the centre of the ONH, suggestive of RAM lesion (blue arrow with blue outline).

Colour fundus image of the left eye 3 weeks post treatment with intraocular gas injection.

High-definition OCT images through the optic nerve head using the enhanced depth imaging (EDI) mode.

Red-free fundus photo of the left eye 2 months post treatment showing the altered residual subretinal blood adjacent to the fovea.
Discussion
In our report, we describe a case of a hypertensive male with POAG and ONH RAM and its related review of literature. Commonly, RAMs affect the major arterial branches posterior to the equator. They are rarely found in the peripapillary region. Studies have shown that 2%–8% of macroaneurysms are located on the optic disc.1,2 The diagnosis of ONH RAM is not very easy and straightforward; this is due to its rare presentation; atypical location; and possible differential diagnosis of granulomatous and neoplastic mass lesion of the optic disc 6 and obscuration of the RAM by the overlying haemorrhage, oedema, and hard exudates. In our case, the RAM was not visualized on the direct slit lamp examination using the +78D lens. This could be due to the deeper location of the RAM hiding within the large glaucomatous cup of the optic disc and presence of overlying haemorrhage. The RAM was well visualized only on FA. One of the closest differential diagnoses could have been polypoidal choroidal vasculopathy (PCV). The characteristic OCT findings of PCV like tall retinal pigment epithelial detachment (PED) or branching vascular network and haemorrhagic PED were absent in our case. Classical FA findings for RAM along with OCT features made the diagnosis tilt more in favour of ONH RAM. Hence, we did not do an indocyanine green angiography in our case. ONH RAMs are usually associated with vascular occlusions, 7 anomalous retinal vasculature, 8 abnormal cilioretinal artery, and Sneddon’s syndrome. 9 A case of ONH RAM with secondary rupture leading to multi-layered haemorrhages in the retina was reported by Rahimy et al. 10 FA should be done to confirm the diagnosis, although dense haemorrhage can block fluorescence enough to obscure the macroaneurysm. In such cases, the use of indocyanine green angiography allows visualization of the macroaneursym through haemorrhage. Another method to image the RAM could be OCT. Goldenberg et al. 11 described the spectral-domain optical coherence tomography (SD-OCT) features of RAMs. On SD-OCT, RAMs were identified as abnormal retinal vessel enlargement located in the inner retinal layers with layers beneath the macroaneurysm appearing hyporeflective probably secondary to the masking effect. We used the high-definition enhanced depth imaging (EDI) mode of the Zeiss Cirrus HD OCT-500 machine to image the RAM. EDI mode showed an abnormal bulbous enlargement of the retinal artery deep within the optic nerve cup, suggestive of a macroaneursym. The natural course of the ONH RAM is spontaneous involution. Most cases on ONH RAMs were observed through spontaneous thrombosis. Treatment is usually reserved for symptomatic patients with submacular haemorrhage or persistent foveal oedema and/or haemorrhage, as was in our case. Treatment options for the RAM include observation, dye yellow laser targeting the macroaneurysm, perianeurysmal argon laser, and intravitreal anti-vascular endothelial growth factor (anti–VEGF) therapy. In our case, we displaced the heme away from the macula by injecting intravitreal gas and observed the RAM due to its close proximity to the ONH.
Conclusion
ONH RAM is extremely uncommon. Identifying RAM at/around the ONH is difficult in patients with glaucoma due to the large and deep optic cup and associated haemorrhage. FA remains the main investigative modality to diagnose RAM. Spontaneous involution still remains the mainstay of treatment in ONH RAM.
Footnotes
Authors’ note
This case was seen during R.V.’s association with his previous institution. Hence, the author’s affiliation is mentioned as Dr. Shroff’s Charity Eye Hospital, while his current affiliation is mentioned in the corresponding author details.
Criteria for inclusion in the authors’/contributors’ list
R.V. was responsible for drafting and analysing the scientific content of the manuscript. P.G. was responsible for data acquisition. The manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met and that each author believes that the manuscript represents honest work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series. Our case report was approved by the institutional review board of Dr. Shroff’s Charity Eye Hospital (SCEH/17/005). Written informed consent was taken from the patient for the usage of patient-related data including images for this particular case report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.