
Abstract
The AMS-800™ artificial urinary sphincter has become the ‘gold standard’ in the treatment of male stress urinary incontinence. In 2006, the novel artificial urinary sphincter FlowSecure™ containing a stress relief balloon providing low cuff pressures at rest with conditional pressure elevation during periods of stress has been launched. We assessed the intraurethral pressure in the cuff area of the AMS-800 and the FlowSecure by urethral pressure profile in four patients each. Urethral pressure profile was performed at rest and during coughing. In addition, continence situation and patient satisfaction after artificial urinary sphincter implantation was assessed. At rest, median pressure in the cuff region was 74 (38–117, FlowSecure) cm H2O and 102 (95–110, AMS-800) cm H2O. During coughing, pressure peaks rose to 135 (54–162, FlowSecure) cm H2O and 202 (128–216, AMS-800) cm H2O. Median pad usage before artificial urinary sphincter implantation in the FlowSecure and the AMS-800 group was 4 (3–4) and 4.5 (2–6) pads/24 h, respectively. At the time of urodynamic investigation, median pad usage declined to 1.5 (0–4) pads/24 h in the FlowSecure and to 1 (1–2) pads/24 h in the AMS-800 group. Seven of eight patients reported on a satisfactory quality of life, and one patient remained unhappy after FlowSecure implantation. It remains unclear if the trade-off in favour of lower cuff pressures, and consecutively lower intraurethral pressures, holds truly long-term benefits regarding device revision, explantation and patient satisfaction.
Keywords
Introduction
The first hydraulic artificial urinary sphincter (AUS) was introduced by Scott in 1974. 1 Over the following decade, the device has undergone several minor modifications until 1987, when the current AMS-800™ (AMS; American Medical Systems, Minnetonka, MN, USA) was released. 2 Until today, the AMS has become the most widely used AUS and ‘gold standard’ for the treatment of moderate to severe stress urinary incontinence (SUI). 3 Nonetheless, since its first description more than 40 years ago, the device remained mostly unchanged and still consists of three components: a pressure-regulating balloon (PRB), a scrotal pump and a cuff placed around the bulbar urethra. 1
The demand on reliable AUS models is growing because of the increasing number of prostatectomies worldwide, with SUI rates of up to 30% 4 consecutively deteriorating continence-related quality of life. 5 However, despite excellent outcome regarding continence, 6 long-term revision rates of up to 85% due to mechanical failure, and explantation rates of up to 20% due to urethral cuff erosion and/or infection, remain high. 7
In 2006, the novel hydraulic FlowSecure™ AUS (FS) was developed (and revised in 2012) to improve the rate of sequelae due to three changes: the single component construction, the additional stress relief balloon (SRB) and a self-sealing port at the scrotal pump 8 (Figure 1). First of all, avoiding multiple tubing components is considered to reduce the rates of postoperative device infections and long-term rates of mechanical failures. Second, since pressure-induced urethral tissue hypoxia is suspected to be the main pathophysiologic mechanism leading to urethral atrophy, 9 the SRB, which provides lower cuff pressures during rest and conditional elevated pressures during periods of stress, is expected to counteract this process. 10 Finally, regarding the self-sealing port, the device can be pressurized in the range from 0 to 80 cm H2O, 8 depending on the continence status, by injecting or withdrawing saline at any time postoperatively. To our knowledge, no data have been published proving this stress-relieving mechanism by urethral pressure profile (UPP) in vivo. The aim of this case series was to assess this principle by UPP and to compare the intraurethral pressures in the cuff area of the FS and AMS. The new FS was designed to create less urethral pressure than the well-tried AMS. This difference has – to our knowledge – never been evaluated via UPP. In addition, patient satisfaction and continence situation was evaluated.
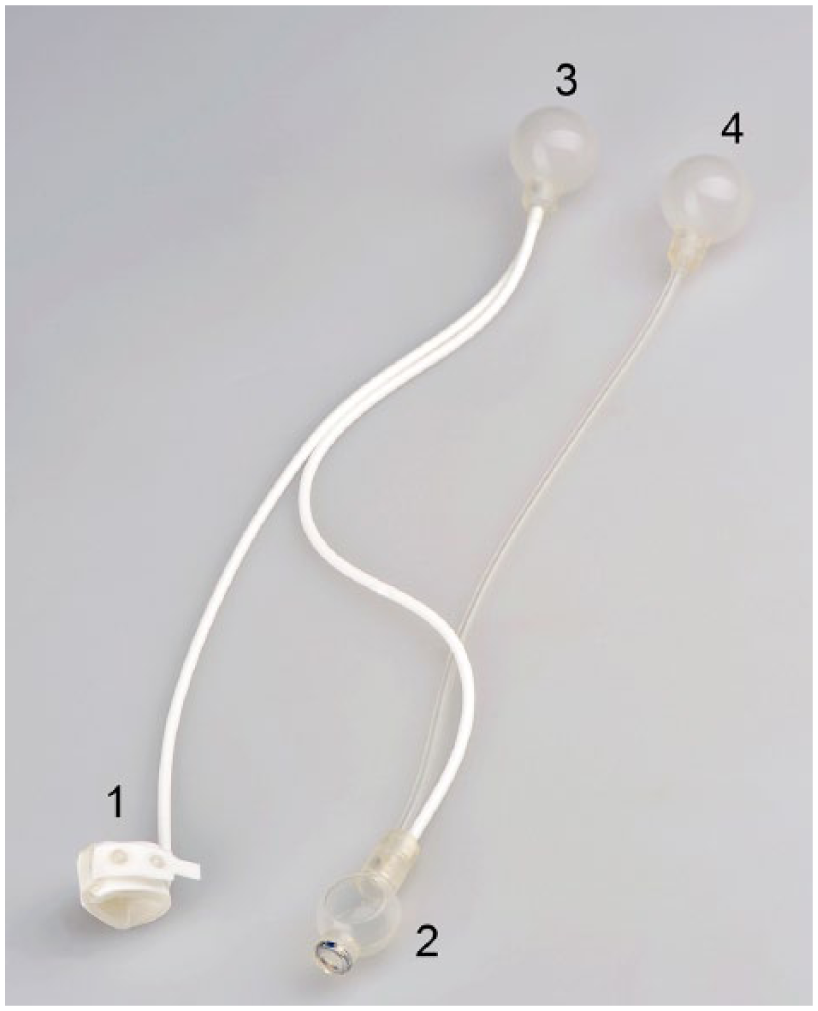
The design of the FlowSecure™ AUS.
Case series
Clinical characteristics
Eight male patients with previous AUS implantation (FS n = 4 and AMS n = 4) were prospectively assessed with urodynamic investigation (UDI) and UPP in this case series after giving their written informed consent. AUS implantation was performed in all patients by the same surgeon, and cuffs were placed periurethrally. Cause of SUI was radical prostatectomy in six patients, transurethral prostate resection in one patient and high-intensity focussed ultrasonography (HIFU) in one patient. All patients had pelvic floor muscle training and conservative incontinence treatment for at least 12 months before AUS implantation, and three patients (3/4) in the FS group had previous unsuccessful male sling surgery. Incontinence was quantified by the number of used pads per day and continence-related quality of life was asked.
UDIs
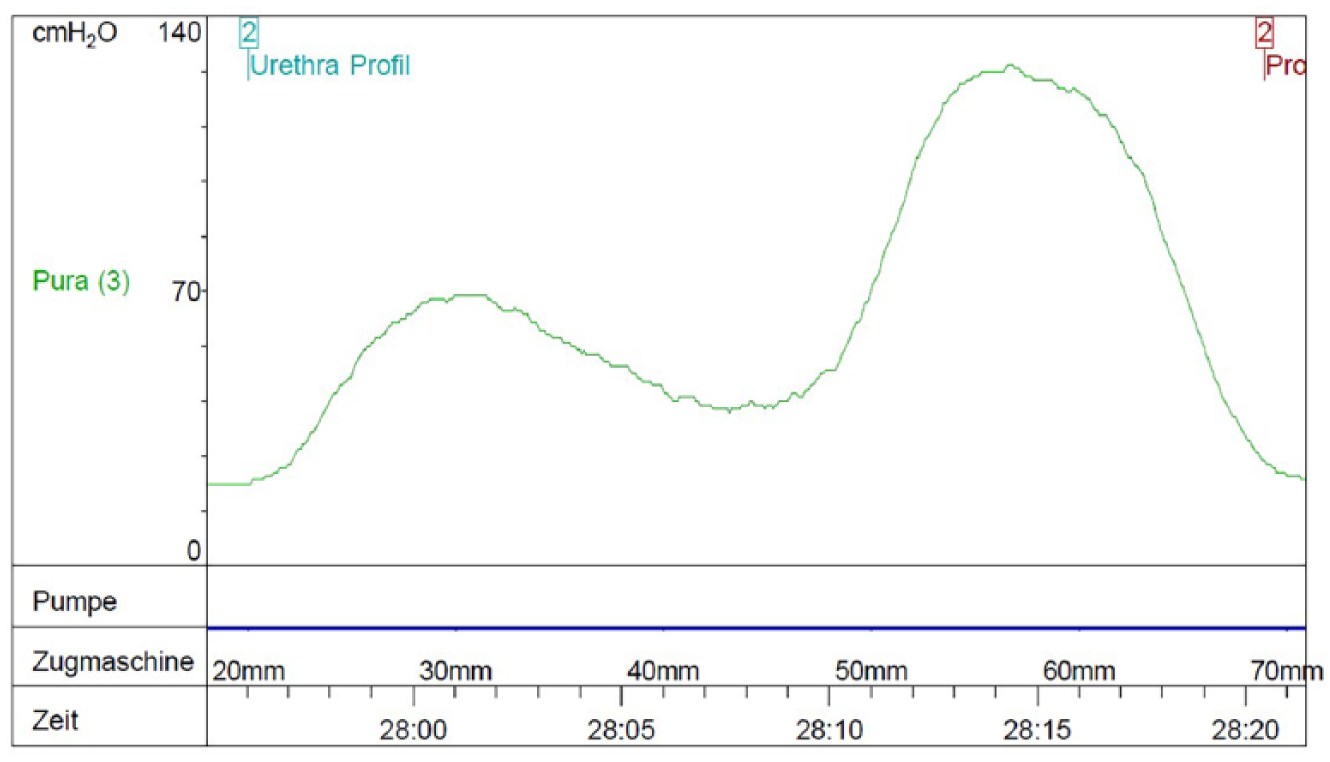
UDI was performed in the FS and the AMS group after a median postoperative period of 24 (17–31) weeks and 79 (49–288) weeks, respectively. The examination was performed in supine position with a MMS solar silver system (Medical Measurement Systems B.V, AN Eschede, The Netherlands) using T-DOC air-charged urodynamic catheters (Laborie Medical Technologies, Mississauga, ON, Canada). For analysis, MMS Database software version 9.1aa, Build 2595 (Medical Measurement Systems B.V) was used. UPP was performed with a pulling speed of 2 mm/s of the measurement catheter at maximum bladder capacity. All UPPs showed two peaks: the first in the membranous urethra and the second in the cuff area of the bulbar urethra. Three measurements were performed in every patient during resting and coughing in supine position.
Statistical analyses
Due to the small number of subjects in each arm (FS n = 4 and AMS n = 4), the validity of statistical analyses is limited. Therefore, we resigned to use any statistical test and limited ourselves instead to a descriptive presentation of the data with medians and their corresponding ranges.
Results
Patient characteristics are shown in Tables 1 and 2. Median age was 73 (68–78) years in the FS and 72 (69–76) years in the AMS group. Before AUS implantation, the median pad use in the FS and AMS group was 4 (3–4) and 4.5 (2–6) pads/day, respectively. All patients reported on an unsatisfactory continence-related quality of life before surgery. The median postoperative period between AUS implantation and UDI was 24 (17–31) weeks in the FS and 79 (49–288) weeks in the AMS group. After surgery, pad usage had declined in both groups to 1.5 (0–4) pads/24 h in the FS and 1 (1–2) pads/24 h in the AMS group. At the time of UDI, seven of eight patients reported on a satisfactory quality of life, and one patient in the FS group remained unhappy.
Patients’ characteristics (FlowSecure™).

NAD: no abnormality detected; TUR-P: transurethral prostate resection; AUS: artificial urinary sphincter.
In selected values, the median has been indicated.
Patients’ characteristics (AMS-800™).

NAD: no abnormality detected; HIFU: high-intensity focussed ultrasonography; AUS: artificial urinary sphincter.
In selected values, the median has been indicated.
UPP showed a double-peaked curve (Figures 2 and 3) in both AUS systems, with the first peak in the membranous urethra and the second higher peak in the AUS cuff area of the bulbar urethra. At rest, the median pressure in the cuff region was 74 (38–117) cm H2O in the FS and 102 (95–110) cm H2O in the AMS group (Table 3). During coughing, median pressure in the cuff region in the FS rose to 135 (54–162) cm H2O and 202 (128–216) cm H2O in the AMS group. No leakage occurred during coughing in both groups. In addition, median residual volume assessed by free uroflowmetry was 15 (0–45) mL in the FS and 0 (0–25) mL in the AMS group. No serious adverse events have been observed after UDI. One patient had to be treated with antibiotics due to a symptomatic urinary tract infection (UTI) after UDI.

Double-peaked urethral pressure profilometry of the FlowSecure™.
Double-peaked urethral pressure profilometry of the AMS-800™.
Comparison of the median urethral pressure in the cuff region.
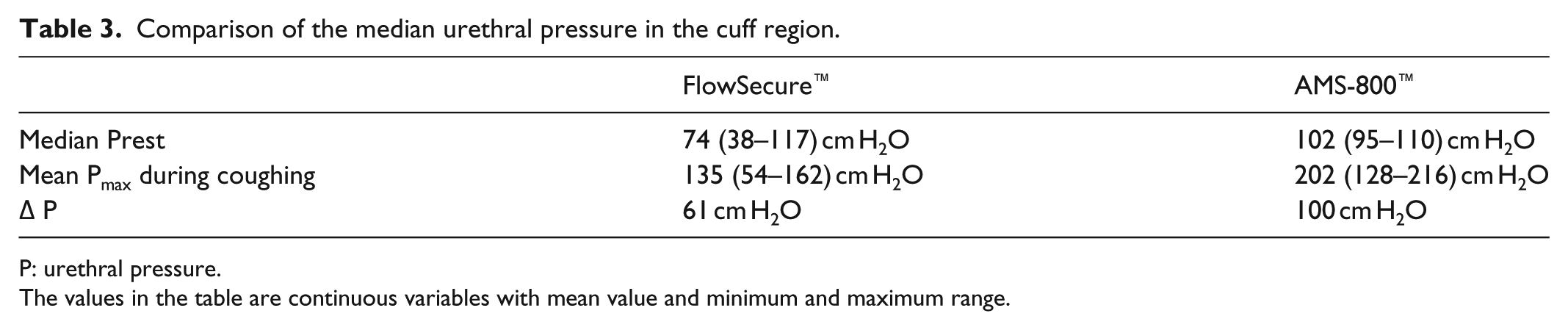
P: urethral pressure.
The values in the table are continuous variables with mean value and minimum and maximum range.
Discussion
In this case series, patients in the FS group had lower median urethral pressures in the cuff region measured by UPP as compared to patients with the AMS. Furthermore, pressure transmission from the abdomen to the cuff, by the extraperitoneally placed SRB, could be observed through pressure amplitudes (Table 3). Interestingly, this was also detected in the AMS group. We interpret this phenomenon due to two main causes: additive transmission of the pelvic floor pressure to the cuff and the guarding reflex. However, if this behaviour could be proven in a larger AMS patient collective, the necessity of the additional SRB regarding continence improvement during stress might be questioned.
In addition, it must be emphasized that exact pressure-amplitude quantification is limited due to the fact that pure cuff pressure could not be measured directly in situ. Instead, urethral pressure was assessed, which is not only caused by the cuff but also by cofactors such as the urethra, corpus spongiosum and the pelvic floor. Therefore, only estimations on cuff pressures and amplitudes can be made with the existing data. Nonetheless, our observations indicate that higher urethral pressures in the AMS group might reflect higher system pressure compared to the FS group.
Finally, regarding clinical outcomes, patients in both groups showed similar improvements of the pad usage and continence-related quality of life.
In 2006, the innovators group 8 published preliminary data of the largest FS patient cohort so far. Nine male patients, having a FS implanted for SUI after prostatectomy and transurethral prostate resection, were included in this observational study, with a follow-up of 12 months. Two devices needed to be explanted within the first 3 months postoperatively: the first, being removed after 8 weeks due to a secondary undone cuff fixation, therefore, not applying any pressure to the urethra, and the second, being removed after 3 months because of a fracture at the joint between the tubing and the cuff. Both problems were interpreted as mechanical issues and lead to subsequent changes in the manufacturing process. UPPs were carried out in the remaining seven patients 3 months postoperatively. The mean urethral pressure (±SD) in the cuff area, calculated from the difference between the peak and the baseline pressure at rest, was 39.4 (±14.7) cm H2O. In comparison, urethral pressures observed at rest in our four FS patients were clearly higher. However, this might be coincidence due to the small patient number and/or methodological reasons, since we have not measured and subtracted the baseline urethral pressure.
Regarding the relationship between cuff pressure and urethral atrophy, a recent publication by Bugeja et al. 11 caused this hypothesis to totter. First, evidence supporting a relationship between high cuff pressure, urethral hypoxia and atrophy has never been published so far. Second, the development of a mesothelial sheath encapsuling the cuff and causing extrinsic urethral constriction might be an alternative explanation.
Regarding clinical improvement, mean pad usage declined from 3.3 to 1.6 pads/24 h at 12 months, which was comparable to the improvement we observed in our patient series. Nonetheless, the authors did not perform UPP during periods of stress, hence not observing the pressure relief mechanism.
To sum up, although our case series is small, findings regarding clinical outcome were in general consistent with the data published by the group from London.
What are the clinical implications of our case series? The FS was developed to provide an alternative AUS for the efficient control of SUI and to improve the shortcomings of the market-leading AMS, consecutively lowering revision and explantation rates. 8 Using a lower urethral pressure in the FS is assumed to lower the risk of urethral erosion. Our small series did show a lower urethral pressure in the FS compared to the AMS. Further studies with a long-term follow-up are needed to assess whether the lower urethral pressure will also lower the risk of urethral erosion and the need of surgical revision of the AUS.
In our results, a pressure transformation from the abdomen to the urethra can be demonstrated in both FS and AMS patients. This finding questions the need of the additional SRB in the FS.
From a surgical perspective, particularly the one-piece assembly of the FS makes the handling and the implantation quick and simple. 12 Consecutively, shorter operating time and minimized perioperative handling might reduce prosthesis infections, leading frequently to explantation of the AUS in the first months after surgery.
Up to date, no data have been published regarding long-term clinical outcomes and revision rates of the FS. Our case series has two main limitations: low number of patients, which does not allow any statistical analyses, and a heterogenic study population with different causes of SUI.
First, regarding the low number of patients, the aim of this case series was to observe the mechanism of the pressure course and its transmission from the abdomen to the cuff. In our view, this principle can be answered with a low number of patients. Since almost all patients had a long way of suffering from SUI and insufficient treatment behind them, we decided not to expose more patients to a potentially harmful examination, such as the UDI, as the principle questions of the study could be answered. Despite stringent hygienic measurements and very careful catheter placement, one patient suffered from a UTI after the urodynamic examination.
Conclusion
It remains unclear if the trade-off in favour of lower cuff pressures, and consecutively lower intraurethral pressures, holds truly long-term benefits regarding device revision, explantation and patient satisfaction. For this reason, long-term data of sufficiently powered and well-designed prospective randomized trials, comparing both devices, are highly needed to make final recommendations.
In conclusion, the newer FS needs some adaptions in clinical practice regarding postoperative management to secure high quality in care of those highly challenging patients. However, trials with longer follow-up are needed to pinpoint on possible new challenges, such as scrotal infections due to manipulations at the self-sealing port or iatrogenic device lesions, and their solutions and prophylaxis.
Footnotes
Author contributions
A.C.H. and J.T. drafted the manuscript (contributed equally). H.A.J. provided critical revision of the manuscript. All the authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was not sought for this case series. Patients had undergone a routine clinical follow-up, which included the assessment of the urethral pressure profile through the placement of a tiny catheter through the urethra into the bladder. Due to the small number of patients, no further investigations were conducted.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the implantation of the artificial urinary sphincter. This consent also includes the follow-up examinations and the publication of the obtained data.