
Abstract
The severe acute respiratory syndrome coronavirus 2 pandemic has necessitated enhanced protection against viral transmission among healthcare professionals, particularly relating to handwashing and personal protective equipment. Some of these requirements may persist for years to come. They bring associated concerns around skin hygiene and general care, with damage to the face and hands now a well-documented consequence among healthcare professionals. This review assesses optimal skin care during the severe acute respiratory syndrome coronavirus 2 pandemic and in the “new normal” that will follow, identifies current knowledge gaps, and provides practical advice for the clinical setting. Regular, systematic hand cleaning with soap and water or an alcohol-based hand rub (containing 60%–90% ethanol or isopropyl alcohol) remains essential, although the optimal quantity and duration is unclear. Gloves are a useful additional barrier; further studies are needed on preferred materials. Moisturization is typically helpful and has proven benefits in mitigating damage from frequent handwashing. It may be best practiced using an alcohol-based hand rub with added moisturizer and could be particularly important among individuals with pre-existing hand dermatoses, such as psoriasis and eczema. Face moisturization immediately prior to donning a mask, and the use of dressings under the mask to reduce friction, can be helpful dermatologically, but more work is required to prove that these actions do not affect seal integrity. Nonetheless, such measures could play a role in institutional plans for mitigating the dermatologic impact of transmission control measures as we exit the pandemic.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic has had a significant impact on healthcare provision across the world. It has raised urgent questions about the most appropriate techniques for preventing viral transmission within the healthcare setting, particularly relating to handwashing and the use of personal protective equipment (PPE). The adoption of effective preventive measures has created mounting dermatologic challenges for healthcare professionals (HCPs), with many reporting the development or exacerbation of skin conditions as a result of these measures.1–8 For some practitioners, this has had significant detrimental effects on personal well-being, including pain, sleep disruption, and anxiety.9,10
The successful roll out of vaccination programs in many parts of the world will most likely reduce the burden of transmission prevention measures on HCPs. Nonetheless, we may have to live with enhanced requirements for handwashing, PPE, and other controls for many years to come. As dermatologists, the authors of this article are often asked by medical colleagues (and patients) about how best to manage the impact of these measures.
The purpose of this review is to (1) assess current evidence regarding optimal skin hygiene and general care during the SARS-CoV-2 pandemic and in the “new normal” that will follow, (2) identify knowledge gaps that require further investigation, and (3) provide practical advice for the clinical setting. The focus is primarily on HCPs but much of the discussion is applicable to the general public.
Methods
The origins of this narrative review came from the discussions of a working group of 11 experienced dermatologists from across Canada (with expertise in medical and surgical dermatology) who convened online to provide written input and then met through videoconferencing to discuss key issues. Searches of online databases (PubMed and Google Scholar) were performed to collate relevant literature, based on combining the search term “SARS-CoV-2 OR COVID-19” with other applicable terms, such as “hand AND (wash OR clean),” “gloves,” “moisturise OR moisturize,” and “face AND mask.” Searches were limited to texts in the English language, with no restriction on the year of publication. Retrieved records were first evaluated for relevance, and greater weighting was then given to data from randomized controlled trials and systematic reviews/meta-analyses compared with other study types.
Hand and skin hygiene
The principal mechanism of infection with SARS-CoV-2 is through exposure to respiratory droplets harboring the virus. 11 However, high viral inoculums can remain viable and infectious on surfaces for several days.12–14 Frequent cleansing of the skin, particularly the hands, provides a simple, inexpensive, widely used and effective strategy for preventing self-inoculation, by reducing viral transfer to the mucous membranes of the nose, mouth, and eyes.
International recommendations on regular hand cleansing are based on data demonstrating protection against the transmission of respiratory viruses in general.15–19 A meta-analysis of six studies performed during the 2003 SARS-CoV-1 epidemic found that frequent handwashing (> 10 times daily) was associated with significantly reduced transmission (odds ratio (OR) 0.45; 95% confidence interval (CI): 0.36–0.57). 16 A recent Cochrane review noted a more modest benefit from handwashing in preventing respiratory illness (OR: 0.89; 95% CI: 0.84–0.95); the included studies were highly heterogeneous, but the overall effect size was statistically significant. 19
Frequent hand cleaning is therefore likely to remain an important strategy for reducing SARS-CoV-2 transmission. Among HCPs, “frequent” cleaning should be defined not by a specific number of times daily but rather by the particular situations in which it must be performed (Table 1).20,21 Regular hand cleaning is also recommended among patients and support staff entering the clinical environment.

HCP: healthcare professional.
The best two methods for doing this are to use soap and water, or an alcohol-based hand rub (ABHR) containing 60%–90% ethanol or isopropyl alcohol (Table 2).22–24 Both work by disrupting the lipid envelope of the SARS-CoV-2 virus,24,25 although the former has the additional advantage of physically washing away pathogens with running water. 24
Practical advice for the clinical setting.
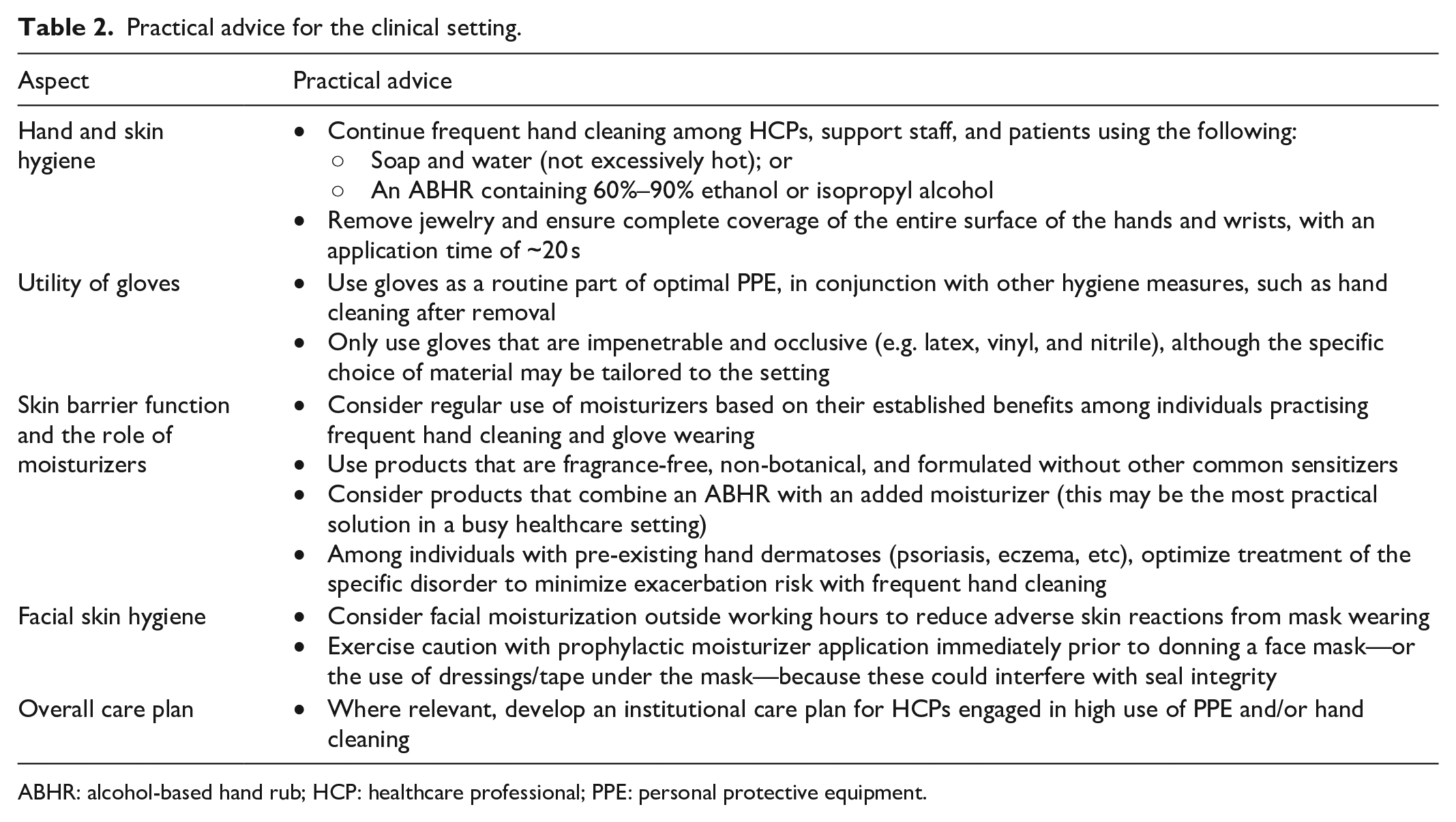
ABHR: alcohol-based hand rub; HCP: healthcare professional; PPE: personal protective equipment.
Soap and water are typically preferred if the hands are visibly soiled. Broadly speaking, water temperature does not matter, although excessively hot water should be avoided because it may increase the risk of damaging the skin barrier. 24 Importantly, the soap used must meet the strict definition: a fatty acid salt with detergent properties created when a fat interacts with an alkali.24,26 It is not yet clear whether synthetic detergents (syndets)—which are generally well tolerated and have a more neutral pH closer to that of skin 26 —are sufficient to provide effective cleaning. However, syndets are typically efficacious against other lipid-enveloped viruses, and hence they are likely to have some activity against SARS-CoV-2. 24
Cleaning with ABHRs is associated with reduced skin barrier disruption and lower rates of irritant contact dermatitis (ICD) and eczema exacerbation compared with soap and water.24,27–31 Hence, ABHRs may be preferable for some HCPs. Many ABHRs are formulated to contain no or low allergen levels. 32 In addition, their dispensers require no plumbing and can therefore be located wherever required, providing greater flexibility and potentially supporting adherence with hand hygiene protocols. 33 When selecting an appropriate ABHR, it should be noted that alcohol percentages differ depending on whether they are calculated by weight or volume. 24 Formulations recommended by the World Health Organization (WHO) based on 80% ethanol or 75% isopropyl alcohol (by weight) both demonstrated high levels of SARS-CoV-2 viral inactivation following 30 s of exposure in vitro. 34 Practical guidelines recommend that these products should contain 60%–90% ethanol or isopropyl alcohol;22–24 levels above 90%–95% should be avoided because they evaporate too rapidly to ensure biocidal activity. 25
Irrespective of whether an ABHR or soap and water is used, cleaning practice should be motivated by ensuring complete coverage of the entire surface of the hands and wrists, based on a systematic approach. Jewelry must be removed. 20 However, there remains uncertainty over both the quantity of soap or ABHR needed for effective hand cleaning and the optimal duration of washing. Current recommendations on the required application time are typically around 20 s with soap and water.22,35 A recent in vitro study found that this duration of exposure to soap products was sufficient to produce ⩾ 3-log reductions in SARS-CoV-2 viral titres, 36 but the impact on skin surface virus levels has not been assessed. With an ABHR, the required application time equates to the time needed to ensure complete coverage of the entire hands and for the alcohol to evaporate; in practice, this may also be (at least) 20 s if a sufficient quantity is used.37,38 Although the exposure time was 30 s in the WHO’s in vitro study of SARS-CoV-2 inactivation with ABHRs, 34 longer application times may not increase antimicrobial efficacy when these products are used in practice and could actually reduce efficacy due to desquamation of the skin.39,40
Utility of gloves
Gloves are routinely recommended as part of optimal PPE.23,41 However, they should only be used in conjunction with other hygiene measures, such as hand cleaning after removal—using either an ABHR or soap and water (Table 1).20,23,41
Several studies have suggested that gloves can reduce the risk of SARS-CoV-2 infection among HCPs.42–44 For example, an analysis of > 10,000 practitioners found that self-reported glove wearing was associated with a 28% reduction in infection risk. 42 Furthermore, a recent US survey showed that patients prefer that their physicians wear appropriate PPE, including gloves, during outpatient consultations. 45 This preference is likely to continue even as the pandemic wanes.
Glove material may be important. In particular, porous fabrics, such as cotton, should be avoided in healthcare settings. Instead, the material should be impenetrable and occlusive to prevent the wicking of water and fomites. Beyond this, there are no data comparing SARS-CoV-2 protection among glove materials, such as latex, vinyl, and nitrile, although previous laboratory experiments have suggested no significant differences in viral penetrability between intact gloves made from these substances.46–48
Glove choice should therefore be specific to the HCP, patient, and healthcare setting. Vinyl gloves are prone to puncturing and tearing and hence have the highest failure rate,46,49,50 but they are inexpensive and may be sufficient for routine skin checks; latex is effective and durable but is associated with allergy problems; 51 nitrile gloves are more durable than vinyl, 50 but are more expensive, may be less “tactile,” and can be difficult to put on and take off, particularly if the hands are not completely dry. In addition, rubber additives found in latex and non-latex rubber gloves are a common cause of allergic contact dermatitis (ACD),52–55 and practitioners may need to switch glove type if such problems arise.
Skin barrier function and the role of moisturizers
Frequent hand cleaning (particular with soap and water27–29) and the use of PPE can have a substantial impact on skin barrier function.1–8 In a systematic review of 35 studies (including > 30,000 participants), the prevalence of skin damage caused by PPE for protecting against SARS-CoV-2 infection was estimated at 75.1%. 8 That review also found that the most frequently observed disorders were contact dermatitis, acne, and eczema; the most common symptoms included itching and burning, and frequently documented signs included erythema and papules. Effects on the hands, cheeks, and nasal bridge were all noted by over 60% of participants. 8
Specifically concerning the hands, a Chinese study found that frequent cleaning (> 10 times daily) appeared to increase the risk of hand skin damage more than wearing gloves for long periods. 2 Nonetheless, the use of gloves even for relatively short periods (> 2 h per day) has been associated with negative effects on the skin.31,56 There is no evidence of dermatologic transmission of SARS-CoV-2, but damage to the skin of the hands could still increase the risk of viral transmission through an indirect effect on hygiene; if skin barrier function is disrupted, cleaning of the hands may become uncomfortable—potentially leading to less frequent and less thorough cleansing.
Moisturizers can be helpful among individuals practising frequent hand cleaning. Studies have demonstrated that moisturizers specifically reduce dermatitis caused by regular handwashing, with positive effects on skin hydration and roughness, reduced transepidermal water loss (TEWL), and improvements in Hand Eczema Severity Index relative to controls.57,58 Skin-surface evaporation from water-based moisturizers may create a cooling effect that is antipruritic. 59 In addition, some moisturizer components—such as glycyrrhetinic acid, palmitoyl-ethanolamine, and telmesteine—have anti-inflammatory properties, which are mediated by blocking cyclooxygenase activity and downregulating the production of proinflammatory mediators. 59 Further studies are needed to confirm that these anti-inflammatory components can reduce dermatitis associated with handwashing and PPE and also to assess possible allergenicity. Nonetheless, in a recent questionnaire-based study of HCPs, the frequency of PPE-related skin problems was significantly lower among those who were using a moisturizer. 60
In practice, the overall usefulness of these products will depend on the particular skin disorder (if any), frequency of hand cleaning, the soap or ABHR used, and the specific moisturizer or barrier cream applied. Moreover, it is not always possible to moisturize after every instance of hand cleaning in a healthcare setting. Therefore, products that combine an ABHR with an added moisturizer may be particularly useful. Separate use of a moisturizer may only be practical during periods of downtime and/or outside working hours.
Preservatives are often included in moisturizer products, although this is primarily to inhibit microbial growth in the container rather than on the skin. Their virucidal activities are typically not well characterized, but some (such as benzalkonium chloride 61 ) do have known antiviral activity. It is unlikely that these preservatives can protect against SARS-CoV-2 transmission at clinically relevant concentrations, but further studies may be warranted.
The improved barrier function associated with moisturizer use57,58 could also reduce the penetration of potential allergens and thus decrease the risk of ACD. However, moisturizers may contain potential contact sensitizers, such as fragrances and preservatives.59,62 Thus, the risk of ACD will differ depending on the specific product used.
Nonetheless, the overall risk–benefit calculation favors moisturizer use given that they are much more likely to have a positive effect on barrier function (indirectly encouraging proper hand hygiene) rather than a negative role in inducing contact sensitization and elicitation. This risk can be further reduced using moisturizers that are fragrance-free, non-botanical, and formulated without other common sensitizers.59,62 Recent recommendations from the American Contact Dermatitis Society also support the use of moisturizers as part of an optimized hand hygiene routine. 24
Repeated daily hand cleaning undoubtedly presents additional challenges to individuals with pre-existing hand dermatoses, such as psoriasis and eczema. Indeed, exacerbation of hand eczema appears to be common,8,63 particularly when using soap and water.30,31 Whether this results in reduced compliance with SARS-CoV-2 hygiene recommendations will likely depend on the individual and the nature and severity of their condition. It is essential to optimize treatment of their specific disorder; regular use of moisturizers and barrier products may help to reduce mechanical irritation and prevent TEWL. 59
Facial skin hygiene
Hand cleaning is recommended primarily for reducing viral transfer to the face, and this provides a potential rationale for washing the face itself. However, there remains a lack of data assessing the impact of regular face washing and it is not part of typical institutional protocols for HCPs. If performed, it should be gentle to avoid causing irritation, particularly among individuals with dermatologic conditions. Nonetheless, normal hygiene routines should be observed, based on face washing in the morning, on returning home from work, and/or at night.
With regard to the wearing of face masks, a recent meta-analysis confirmed that this practice is associated with significant reductions in the risk of SARS-CoV-2 infection among HCPs (pooled OR: 0.29; 95% CI: 0.18–0.44). 64 However, numerous studies have demonstrated that it leads to high rates of adverse skin reactions, particularly on the nasal bridge and cheeks.1–3,5–8 Precise dermatologic diagnoses were often lacking in these studies, but the main issues described include pressure/friction injuries, ICD, ACD (e.g. from the elastic straps, glue, and formaldehyde released from the mask fabric), facial acne flares, and exacerbation of existing dermatologic conditions (e.g. eczema and rosacea).6,7,65 N95 devices are particularly problematic; ensuring an optimal fit to the face may mitigate skin irritation.3,7
Moisturizing the face outside working hours could help to reduce adverse skin reactions, although this should be tailored to the underlying problem(s). Many mask-related skin reactions can respond well to these products.3,7 Furthermore, in an analysis of mask wearing in which participants moisturized one side of their face and not the other, moisturization significantly reduced detrimental effects on skin quality markers, such as wrinkling and skin-pore area. 66
Prophylactic moisturizer application immediately prior to donning a face mask is still somewhat controversial because it could interfere with the seal of the mask. A small study of N95 use following the application of a bland emollient or silicone barrier cream found no impact on the seal. 67 Canadian guidelines suggest that facial moisturizers should be allowed to dry before donning a mask; 68 others have proposed a 30-min gap between moisturizing and mask application to mitigate the risk of seal damage. 3
The wearing of dressings or tape under the face mask has also been shown to reduce adverse skin reactions, although there is conflicting evidence on whether this can adversely impact on the seal of the mask.7,69–71
Drawing on this research, a recent study evaluated a five-point care plan developed for HCPs who regularly wear face masks. 72 It consisted of the following: skin protection through cleansing and moisturization; appropriate face mask selection; use of dressings/tape to reduce friction; skin and face mask inspection during clinical shifts; and cleansing and hydration on removal. Deployment of this plan was associated with a reduction in the incidence of skin injury from 29% to 8% (OR: 4.75; 95% CI: 2.15–10.49; p = 0.0001). 72 Care plans of this type could be an important feature of the “new normal” for HCPs even as the pandemic comes under control.
Limitations and research needs
Huge amounts of SARS-CoV-2-specific data have been generated in a short space of time since the pandemic began. Nonetheless, the most important limitation of this article is that some of the commentary is based primarily on expert opinion and/or extrapolation of data from other respiratory viruses. SARS-CoV-2 remains a relatively new entity and much virus-specific work is still ongoing. A list of some of the key research requirements is provided in Table 3. In particular, there remains a need for SARS-CoV-2-specific analysis of the impact of hand cleaning techniques and of different glove materials on viral transmission, and risk–benefit analysis of moisturizer use during frequent hand cleaning (relating to ICD/ACD). More work is also needed to analyze the effect on seal integrity of moisturizer application immediately before putting on a face mask, and of using dressings or tape under the mask to reduce friction.
Areas for further investigation.
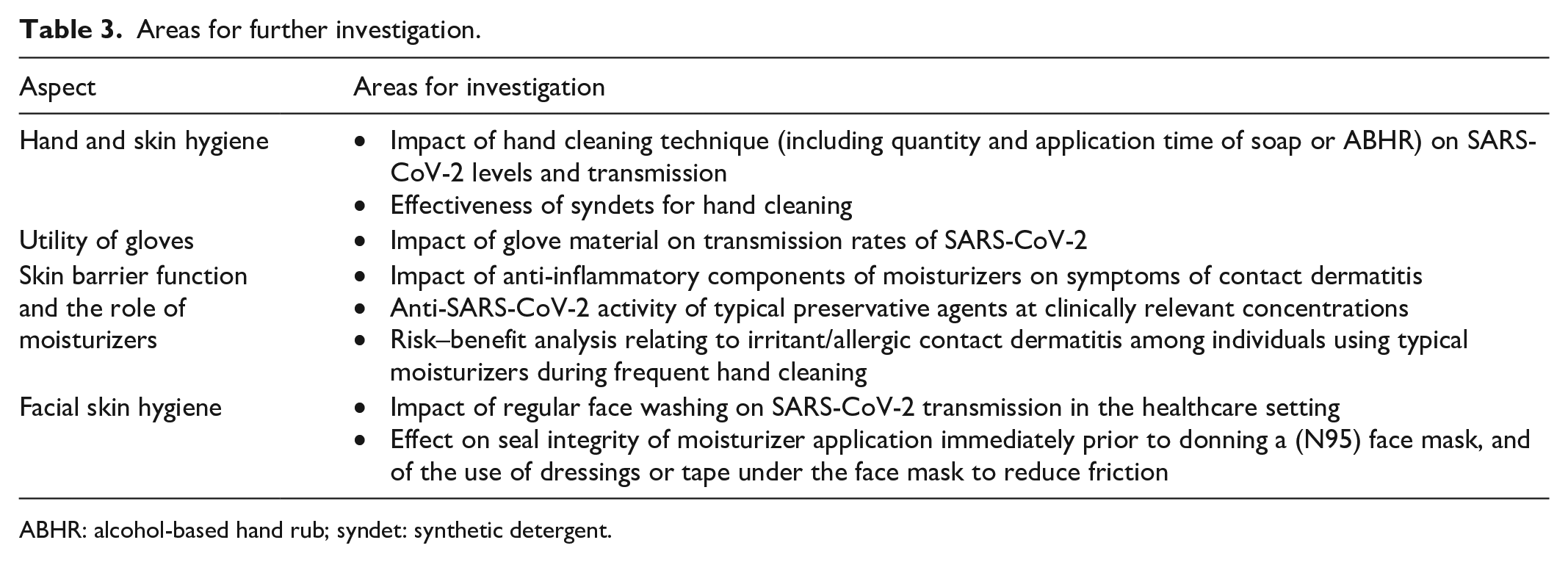
ABHR: alcohol-based hand rub; syndet: synthetic detergent.
Conclusion
Successful SARS-CoV-2 vaccination programs should reduce the burden of transmission prevention measures on HCPs, but heightened requirements for handwashing and PPE could persist for many years. In particular, the continued use of gloves and possibly also face masks may be necessary to reassure patients, even in non-SARS-CoV-2-related outpatient settings.
Thus, the associated dermatologic challenges will remain. Our practical advice for mitigating these issues is summarized in Table 2. Skin damage to the face and hands is now a well-documented and common consequence of SARS-CoV-2 infection prevention measures among HCPs, often causing meaningful reductions in personal well-being. Moisturization is generally helpful. In particular, moisturizing the hands has proven benefits in mitigating damage from frequent washing and may be best practiced using an ABHR with added moisturizer. This could be particularly important among individuals with pre-existing hand dermatoses, such as psoriasis and eczema. The application of moisturizer on the face immediately prior to donning a mask, or the placement of dressings or tape under the face mask to reduce friction, remains somewhat controversial and further work is needed to prove that these actions do not interfere with seal integrity. Nonetheless, such measures could play an important role in institutional care plans designed to mitigate the dermatologic impact of transmission control measures as we exit the pandemic.
Footnotes
Acknowledgements
The authors thank Timothy Ryder, DPhil, of Biological Com-munications Limited (London, United Kingdom) for providing writing and editorial assistance funded through an unrestricted educational grant from AbbVie.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.K.R. has been a consultant, investigator, and speaker for AbbVie, Allergan, Galderma, Leo Pharma, and Pfizer; is a consultant for MetaOptima Technology Inc.; and is the founder and a shareholder of Riversol Skin Care Solutions Inc. J.P.A. reports no conflicts of interest to disclose. J.D. reports no conflicts of interest to disclose. L.C.G. has been a consultant, investigator, and speaker for AbbVie, Allergan, Janssen, and La Roche-Posay, and a speaker for Johnson & Johnson and Pierre Favre. C.M. reports no conflicts of interest to disclose. V.R. has been an investigator for AbbVie, Allergan, Galderma, Leo Pharma and Pfizer, and a speaker and consultant for AbbVie, Bausch Health, Celgene, Eli Lilly, Galderma, Janssen, Leo Pharma, L’Oréal (La Roche-Posay), Novartis, Pfizer, Proctor & Gamble, and Sanofi. N.R. reports no conflicts of interest to disclose. J.-F.T. reports no conflicts of interest to disclose. M.C.W. reports no conflicts of interest to disclose. C.Z. reports no conflicts of interest to disclose. D.Z. has been a consultant, investigator, and speaker for Genentech/Roche and Sanofi Genzyme.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Writing and editorial assistance was provided by Timothy Ryder, DPhil, of Biological Communications Limited (London, United Kingdom) funded through an unrestricted educational grant from AbbVie.