
Abstract
Atypical Spitzoid lesions pose a distinct challenge in classification as they may comprise a mixture of both classic benign nevus and cutaneous melanoma characteristics. Immunostaining and molecular analysis, such as comparative genomic hybridization, can assist in narrowing the differential diagnosis. We present a case of a 5-year-old male with an atypical Spitzoid lesion on his back. Initial histopathology revealed a relatively symmetric lesion with mitotic figures and poor maturation of melanocytes with descent into the dermis. Immunohistochemistry demonstrated a loss of p16, and array comparative genomic hybridization revealed a loss of chromosome 9, supporting a diagnosis of invasive melanoma arising in conjunction with a remnant of a conventional melanocytic nevus. This case is the first in Canada to demonstrate the use of array comparative genomic hybridization for diagnosing melanoma in a young paediatric patient.
Introduction
Melanoma is a rare type of paediatric malignancy with an incidence of fewer than 500 cases being diagnosed annually in the United States. 1 The distinction of malignant Spitz lesions from the typically benign Spitz nevi is critical for prognosis and clinical management of paediatric patients. However, it can be difficult to distinguish these based solely on conventional histologic features because of morphologic heterogeneity, with poor diagnostic concordance among clinicians.2,3
In contrast with benign Spitz Nevi, approximately 96% of melanomas have chromosomal copy number gains and losses. 4 Therefore, array comparative genomic hybridization (CGH) can aid classification of melanocytic lesions, especially when diagnosis based on histology is inconclusive.5,6
To the best of our knowledge, there is a limited number of reports demonstrating CGH analysis in diagnosing melanoma in children aged 5 and younger.5,7 We report a case of invasive melanoma in a 5-year-old Canadian male whose genomic profile was assessed by array comparative genomic hybridization (aCGH).
Case report
A 5-year-old Caucasian male with Fitzpatrick skin type 2 was referred for evaluation of a lesion along the midline of his upper back. The lesion was first noted at 2 years of age. It later developed as a 6 mm brown papule, which was diagnosed as a nevus, with a peripheral halo of hypopigmentation and central thickening (Figure 1). There was no family history of melanoma.

The pigmented lesion with a peripheral halo of hypopigmentation. Within the previous year prior to referral, it had started to enlarge and thicken centrally with no associated pruritus or pain.
An excisional biopsy (9 mm by 6 mm by 3 mm) was performed. The junctional component of the nevus was relatively symmetric and contained large melanocytes with abundant cytoplasm and nucleoli. In the epidermis, melanocytes were distributed primarily as nests at the tips and sides of the rete ridges with some clefting from the overlying epidermis and discohesion among melanocytes within the nests (Figure 2(a)). Nests appeared to predominate over single cells, without a significant upwards scatter (Figure 2(b) and (c)). Single cells were plump epithelioid cells with amphophilic to eosinophilic cytoplasm and nuclei. Some had prominent nucleoli, and others had marked nuclear hyperchromasia and smudging. In the dermis, similar melanocytes were present with poor maturation upon descent. Kamino bodies were not observable. The dermal component also revealed prominent nuclear atypia with scattered mitotic figures (Figure 2(d)). Asymmetrical melanin pigmentation of the dermal component and a mild, asymmetric lymphocytic infiltrate were noted. A small cluster of melanocytes with cytomorphology suggestive of a conventional nevus component was also present.
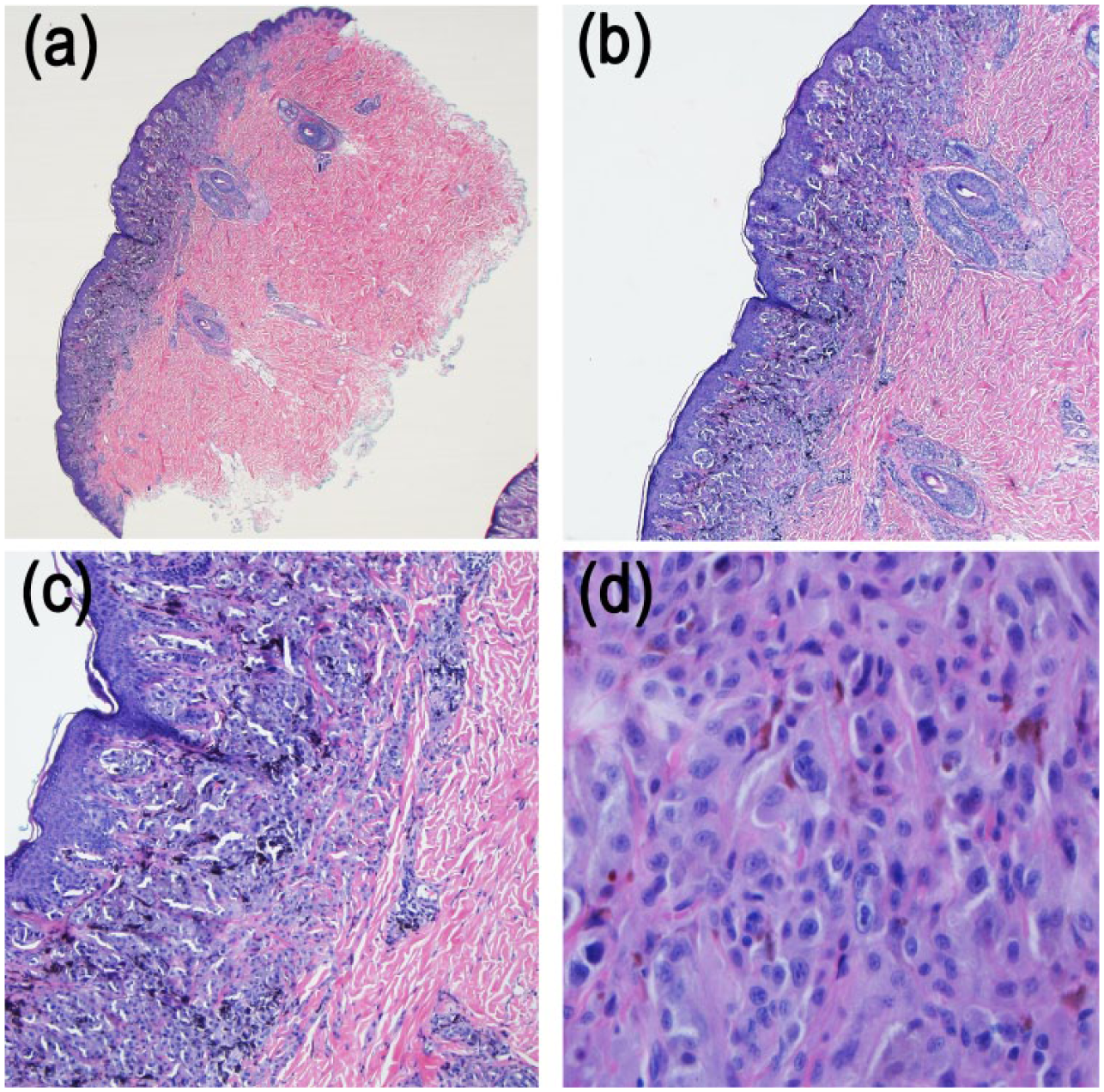
Hematoxylin and eosin stain of the biopsy. Low power 20x magnification (a) revealed a compound melanocytic proliferation involving the base of the epidermis and superficial dermis. The melanocytic proliferation was symmetrical. An inflammatory response was not identified. At 40x magnification, (b) most of the epidermal melanocytes were confined to the epidermal base. There was only focal intra-epidermal ascent of the melanocytes identified. At 100x magnification, (c) there was no intra-epidermal ascent of melanocytes identified in this photograph. The dermal melanocytes showed maturation to the base of the lesions. At 400x, (d) some of the melanocytes were multinucleate and exhibited pleomorphism of nuclear size variation (>4x variation). Occasional nucleoli and mitoses were identified.
Immunohistochemistry showed a loss of p16 throughout the lesion, except in the region of the conventional nevus component. HMB45 revealed faint positivity throughout the thickness of the lesion. MelanA/Ki67 was unable to be interpreted due to poor MelanA staining quality.
Due to the atypical features, the specimen was sent out for further molecular investigations. aCGH demonstrated gain in chromosome 7p, subthreshold gain in chromosome 7q, loss in chromosome 9, and subthreshold loss in 8p (Figure 3). The loss of chromosome 9 was the most prominent molecular result and directly correlated with the loss of p16 expression demonstrated by immunohistochemistry (Figure 3(d)). 6

(a) aCGH analysis of the lesion. There was a gain in chromosome 7p (B), (b) subthreshold gain in chromosome 7q, (c) subthreshold loss in 8p, and (d) loss in chromosome 9.
The patient then underwent wide local excision with 1 cm margins. Pathology of the wide local excision tissue showed a focal area of dermal fibrosis at the presumed previous biopsy site and some reactive, overlying melanocytic cells. However, there were no definitive atypical melanocytic cells and no evidence of residual malignant melanoma. Sentinel lymph node biopsy (SLNB) showed no evidence of metastatic malignant melanoma. The final diagnosis was an invasive melanoma, non-ulcerated, 1.2 mm Breslow thickness, mitotic index 1/mm2, Clark’s level unspecified, and Stage IB. The patient remains well 20 months after diagnosis and receives regular follow-up.
Discussion
This case highlights the diagnostic challenge of atypical Spitz lesions. The patient’s young age and lack of family history reduced the suspicion of malignant melanoma. However, due to the lesion’s evolution, further investigations were warranted.
Currently, histopathology is the standard for the diagnostic classification of melanocytic skin lesions. However, there is significant inter-observer variability, and no single feature or set of criteria are diagnostic. 8
In this case, the non-ulcerated lesion shared morphological features (melanocytes with abundant cytoplasm and relatively symmetric large nuclei) in keeping with benign or intermediate etiologies. However, the presence of nuclear atypia in the dermis and melanocytes with mitotic figures and poor maturation with descent were worrisome for malignancy. Thus, there was a need to implement diagnostic tools such as immunohistochemistry and aCGH to better characterize the lesion. A panel of immunohistochemical markers such as Ki-67, HMB45, p53, p16, p21, cyclin D1, and CD99 can complement conventional histopathology to distinguish melanomas from atypical Spitzoid lesions, although diagnostic uncertainty may remain.9,10
The main benefit of CGH is that it can investigate the entire genome. The relative abundancies of DNA from tumour specimens and normal controls after hybridization are compared to determine chromosomal aberrations, represented by DNA copy number gains or losses.11,12 Bastian et al. 4 have reported that less than 4% of all malignant melanoma studied had a normal CGH result. For our patient, the identification of multiple copy number gains and loss, such as chromosome 9 loss, indicated genomic instability that provided support for the diagnosis of melanoma ex melanocytic nevus.
At present, aCGH application in a clinical setting is limited, especially in the paediatric population. Previously, it has been used to confirm the histological diagnosis of a benign nodule developing within a congenital melanocytic nevus of a 3-month-old infant. 7 Vanison et al. 13 demonstrated its potential to amend a diagnosis of a compound melanocytic nevus in a 13-year-old patient. They suggested that earlier application of aCGH could avoid unnecessary surgical interventions such as SLNB and complete lymph node dissection. 13 Tom et al. 5 presented their experience of managing six paediatric cases of atypical Spitzoid nevi with diagnostic modalities including SLNB, immunostaining, and molecular analysis. A more recent study by Dubruc et al. 14 reported the use of aCGH and fluorescence in situ hybridization to reveal NRAS gene amplification in two atypical cutaneous melanocytic tumours.
In summary, our case highlighted the complexity of diagnosing an atypical Spitzoid lesions in young patients. We report that aCGH results corroborated with immunohistochemistry and demonstrate that these two adjunctive analytic methods can further support or refute the diagnosis of malignant melanoma.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent to perform and submit the case report for publication was obtained and given by the patient’s mother.