
Abstract
Melanomas most commonly localized in the skin can arise anywhere in the body, and approximately 5% of all melanomas appear in other sites of mucosal surfaces out of skin. Primary melanoma from nasal mucosa is quite rare. We present this case: a 46-year-old man had complained a pain in the left upper abdomen for 2 months when he was admitted to the Northern Jiangsu People’s Hospital. The pain was paroxysmal and enhanced when eating. There was no nausea, vomiting, or anorexia. There had been no change in weight in previous months. This patient had a past history of surgery for nasal mucosal malignant melanoma 2 years ago. Abdominal enhanced computed tomography (CT) indicated that a mass originated from small bowel and occupied the left upper abdomen. The patient underwent a laparotomy during which a black lesion measuring about 5 cm × 5 cm × 4 cm was found at the jejunum and resected totally together with partial jejunum. The patient was eventually diagnosed as secondary jejunal malignant melanoma from nasal mucosal melanoma. For patients with a history of melanoma, gastrointestinal metastasis should be considered when patients develop gastrointestinal symptoms. In addition, we recommend positive anti-tumor therapy after surgery.
Introduction
Mucosal melanomas located in the mucosal membranes are malignant primary tumors originating from melanocytes, which usually occur in occult sites like nasal cavity, and have the lowest 5-year survival rate compared with cutaneous and ocular melanoma, due to a lack of early specific signs and a delay of diagnosis. 1 The majority of malignant melanomas in the small intestine are metastases from primary lesions, and a primary mucosal tumor in the gastrointestinal tract is an extremely rare neoplasm. 2 Due to the lack of specificity of clinical symptoms and signs, preoperative diagnosis of gastrointestinal metastatic melanoma is difficult and often delayed until the pathology is clear after surgery. Clinical manifestations of gastrointestinal metastasis are relatively insidious, and diagnosis is often made as complications such as intestinal obstruction and intussusception. Surgery remains the preferred treatment for gastrointestinal melanoma.3,4 In this study, we report a quite rare case of a secondary jejunal malignant melanoma from nasal mucosal melanoma.
Case report
A 46-year-old man had complained a pain in the left upper abdomen for 2 months when he was admitted to the Northern Jiangsu People’s Hospital. The pain was paroxysmal and enhanced when eating. There was no nausea, vomiting, or anorexia. There had been no change in weight in previous months. This patient had a past history of surgery for nasal mucosal malignant melanoma 2 years ago. Physical examination showed deep tenderness in the left abdomen. Laboratory test is normal. Abdominal enhanced computed tomography (CT) indicated that a mass originated from small bowel and occupied the left upper abdomen (Figure 1).

Abdominal computed tomography (CT) scan showed a mass originated from small bowel occupying the left upper abdomen.
The patient underwent a laparotomy. A black lesion measuring about 5cm × 5cm × 4 cm was found at the jejunum (Figure 2). We resected the total lesion and partial jejunum (Figure 2). Hematoxylin–Eosin staining showed many bundles of oval tumor cells (Figure 3). Immunohistochemistry showed that the tumor cells were strong positive for HMB45, S-100, Melan-A and Vimentin, and extremely high for Ki67 (about 70%+), and negative for CKpan, CK20, Villin, CDX-2, and EMA. It is consistent with the primary nasal mucosal melanoma. Based on the above results, the tumor was finally diagnosed as secondary malignant melanoma of the small bowel. The post-operative course was uneventfully and the patient was discharged 2 weeks after surgery. However, the patient refused further anti-tumor treatment. Therefore, we recommend that patients be reviewed every 3 months with regular follow-up.

A black and hard lesion measuring about 5 cm × 5 cm × 4 cm was identified at the jejunum.
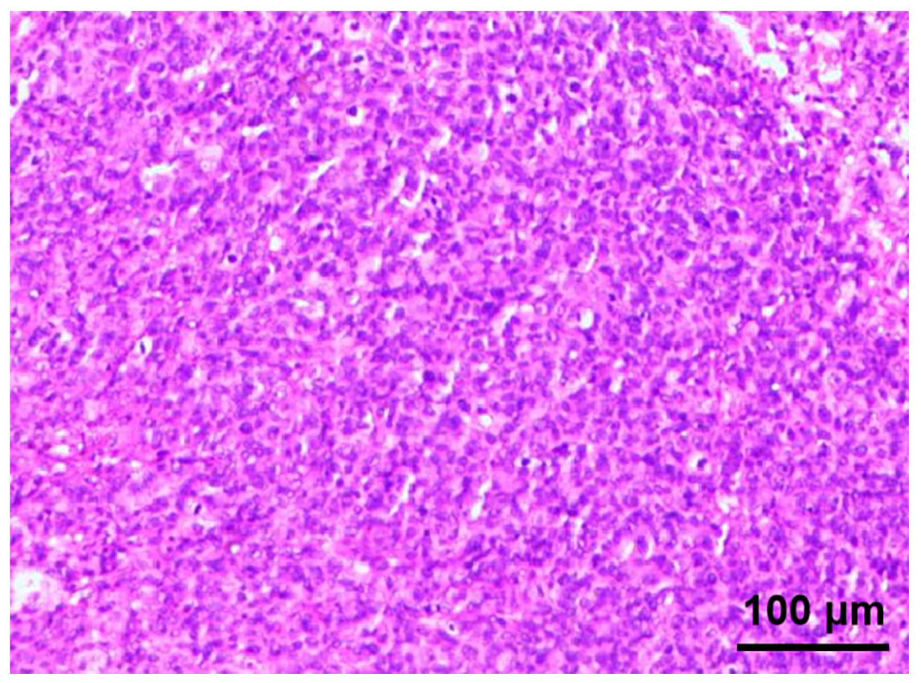
Hematoxylin–eosin (HE) staining showed homogeneous proliferation of bundles of oval tumor cells.
Discussion
Melanoma is a highly malignant tumor that occurs in the skin, eyes, and anal canal. The pathogenesis of mucosal melanoma is unclear, but some genetic and metabolic alterations are known. Recent data suggest that GNAQ/11 mutations occurred in 9.5% of the patients. The mean survival of patients with GNAQ/11 was significantly shorter than that of wild-type GNAQ/11. 5 Furthermore, Itoh et al. 6 suggest C-KIT (CD117) is overexpressed in over 80% of cases. B-type Raf (BRAF) mutations are uncommon (less than 10% of cases) in mucosal melanoma. 7
A gastrointestinal malignant melanoma is rare in clinical practice. 8 Most of the reports are gastrointestinal metastases, and very few are primary gastrointestinal tract. The small intestine became the most common site of gastrointestinal metastatic melanoma due to blood supply (67%), followed by colon (9%), stomach (6%), and rectum (2%). 9 The clinical symptoms of patients with malignant melanoma with gastroduodenal metastases are not typical. They may have non-specific symptoms such as bloating, hernia, acid reflux, and complications such as bleeding and perforation. 10 In this case, the patient had a pain in the left upper abdomen for 2 months. Abdominal enhanced CT indicated that a mass originated from small bowel and occupied the left upper abdomen. Combined with the history of nasal mucosal melanoma, the final diagnosis was secondary intestinal melanoma. Therefore, in patients with a history of melanoma, gastrointestinal metastasis should be considered when they develop gastrointestinal symptoms. There are a few studies on melanoma gastrointestinal metastasis, and most of them are case reports. 11 Many melanoma patients with gastrointestinal metastases are missed early, until a diagnosis or death is made. Fiber endoscopy can detect gastric, duodenal, and colon melanoma lesions and can obtain histological evidence while imaging studies are the most important means to diagnose small intestinal melanoma, including intestinal angiography, abdominal CT, and positron emission tomography (PET). 12 Transabdominal ultrasonography is usually the first diagnostic method in patients with unclear abdominal symptoms. Barium examination is the standard method for diagnosis of intestinal melanoma. The technique accurately detects lumen abnormalities, including low-grade ileus, but does not reveal important extra-intestinal signs. CT intestinal lavage increased the detection rate of primary or metastatic intestinal melanoma compared with conventional CT. The sensitivity and specificity of whole-body PET imaging in detecting gastrointestinal metastasis in melanoma patients were higher than that of conventional CT. Capsule endoscopy is a new technique to improve preoperative diagnosis. It can examine intestinal segments that cannot be examined by conventional endoscopy. It has good diagnostic efficacy for the presence and degree of small intestinal metastasis. Immunohistochemical S-100, HMB45, Melan-A, SOXl0, MiTF, BRAF and Vimentin positive are helpful for diagnosis and identification. S-100 is highly sensitive to melanoma (97%–100%), but its diagnostic specificity is poor due to its expression in nerve sheath cells, myoepithelial cells, and adipose cells. HMB45 has high specificity but poor sensitivity. Melan-A is a melanoma-specific antigen with a specificity of 95%–100% and sensitivity of 75%–92%. Vimentin is almost universally expressed in melanoma. 13 However, a definite diagnosis can only be made after a thorough investigation in order to exclude the coexistence of a primary lesion. 2
There are not yet established standard treatments for small intestinal malignant melanoma metastasis. The combination of surgical resection and different ancillary treatments is a reasonable choice, and the choice of treatment should vary from person to person. Some authors believe that surgical resection is necessary. 14 Early detection and radical surgery are important means of treating gastrointestinal melanoma. The main influencing factors for long-term survival of small intestine metastatic melanoma patients are complete resection of the intestinal metastases and complete removal of the initial site of distant metastasis of metastases. The average survival time of patients undergoing radical resection was only 29.7 months, 15 and untreated is only 8 months. 16 Aggressive surgical treatment is not recommended for patients with diffuse disease because it does not remove distant metastatic disease, and therefore does not improve prognosis. Systemic therapy does not improve the prognosis of patients with melanoma small bowel metastases. The response rate of the chemotherapy regimen is very low. 17 However, a recent study shows that target therapy against c-KIT activating mutations and the immunotherapy have emerged as a promising treatment modality for these aggressive tumors. 1 Total surgical resection of the lesion is a correct approach for this patient. Although the effect of surgery combined with chemotherapy or radiotherapy is not clear, we recommend further anti-tumor therapy after surgery. However, due to the high cost, the patient did not take adjuvant treatment.
Conclusion
Gastrointestinal malignant melanoma is rare in clinical practice. Systemic therapy and chemotherapy does not improve the prognosis of patients with melanoma small bowel metastases. The combination of surgical resection and different ancillary treatments is a reasonable choice, and the choice of treatment should vary from person to person. Although the effect of surgery combined with chemotherapy or radiotherapy is not clear, we recommend further anti-tumor therapy after surgery.
Footnotes
Author contributions
L.Z., W.H., and P.C. designed the study. Z.D. and Y.X. collected the data; Y.X., Z.D., K.Z., and Z.D. wrote the manuscript. L.Z., W.H., and M.A. revised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Jiangsu Natural Science Foundation (BK20180274).
Research ethics and patient consent
The study was reviewed and approved by the Northern Jiangsu People’s Hospital Institutional Review Board (BK20190304), and written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.