
Abstract
Perivascular epithelioid cell tumour is a rare mesenchymal tumour with distinct immunohistochemical profile. While it is known to occur in various anatomical sites, the central nervous system had always been a protected site for primary or secondary perivascular epithelioid cell tumours. We describe a 61-year-old lady who presented with symptoms of raised intracranial pressure, 3 months after the resection of duodenal and thoracic tumours which were histologically consistent with perivascular epithelioid cell tumour. She was investigated and then subsequently subjected to resection of two metastatic intracranial lesions. The radiological, intraoperative as well as histopathological findings of the metastatic lesions are discussed. Metastatic perivascular epithelioid cell tumour of the brain is extremely rare. However, patients who are stratified as high risk for recurrence or metastases should undergo an early magnetic resonance imaging/computed tomography of the brain in addition to a whole-body positron emission tomography scan, to allow for early detection and management of these tumours.
Introduction
Perivascular epithelioid cell tumours (PEComas) are rare tumours of the mesenchymal origin which has characteristic perivascular epithelioid histomorphology and immunohistopathological expression of melanocytic markers (HMB 45) and smooth muscle (actin) markers.1,2 It is increasingly reported in a variety of anatomical sites due to the advances in imaging and immunohistopathological techniques. The clinical course is usually benign; however, malignant PEComas have been reported before and often have an aggressive course. 3
Frequent metastatic sites for malignant PEComa include the lung and bone.1,4 The central nervous system has always been a protected site from either primary or secondary PEComas as this is affirmed by the paucity of literature describing these tumours in the brain. 3 We report a patient with the primary diagnosis of duodenal PEComa presenting with two cranial metastases that was treated surgically.
Case report
A 61-year-old lady presented with complaints of acute headache with nausea and vomiting. Physical examinations revealed ataxia and right hemiparesis. She also revealed that she had undergone an abdominal and thoracic surgery to remove tumours from the duodenum as well as the right lung 3 months earlier. The duodenal lesion was presumed to be the primary lesion, while the lung was thought to be the metastatic site. Histopathological findings were consistent with PEComa for both sites.
During current admission, a contrast-enhanced computed tomography (CT) of the brain revealed two lesions – one right cerebellum (4 × 4 cm2) and another left temporal lobe (2 × 2 cm2) with avid contrast uptake (Figure 1). Magnetic resonance imaging (MRI) revealed two distinct lesions with low signal intensity on T1-weighted sequence and avid enhancement post gadolinium administration (Figure 2). T2-weighted sequence demonstrated blooming artefact in the right cerebellar lesion suggestive of intratumoural haemorrhage and necrosis.
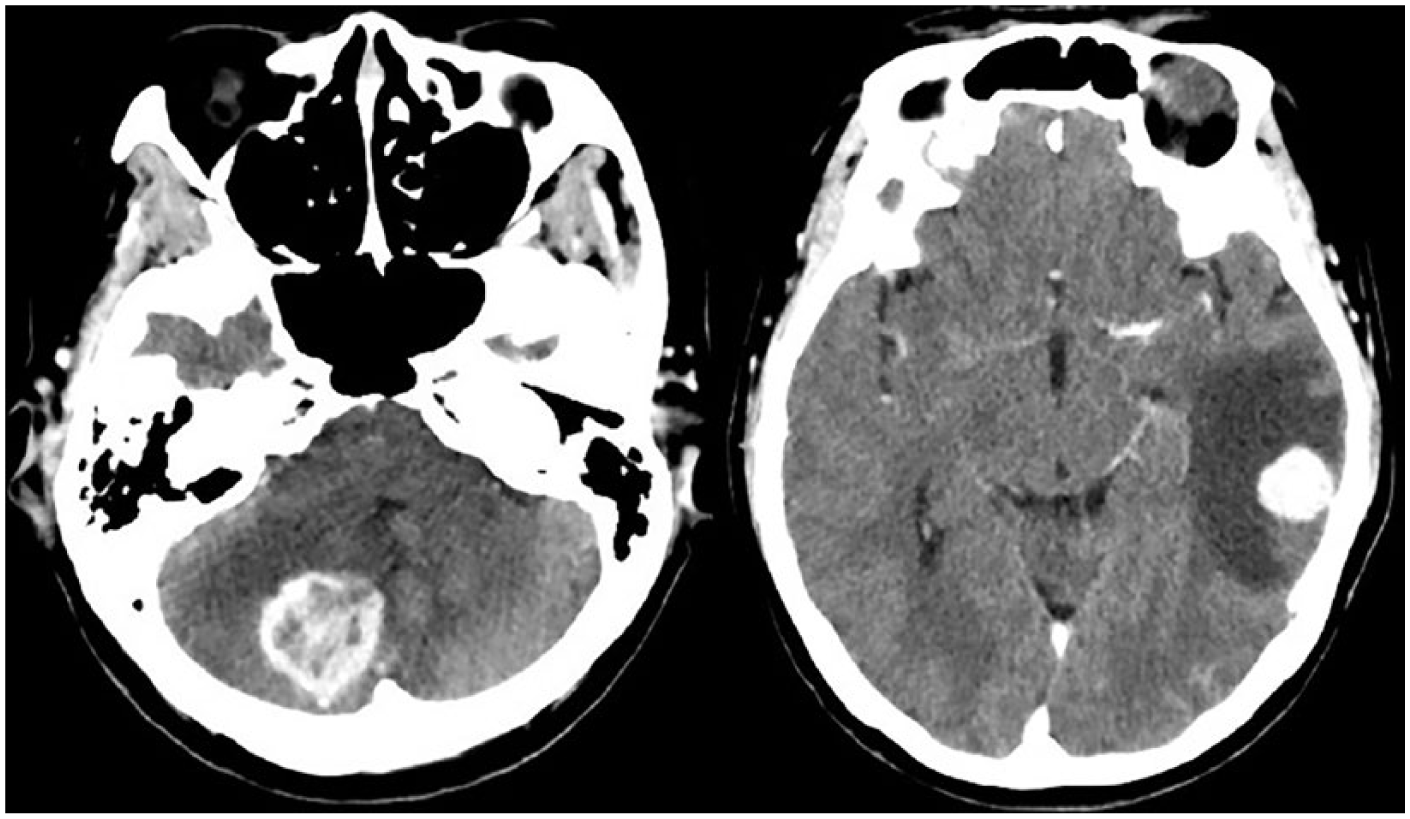
Contrast-enhanced CT of the brain: right cerebellar mass (left) and left posterior temporal mass (right) showing a good contrast uptake.

Post-gadolinium contrasted MRI images showing a distinct right cerebellar lesion with central necrosis (black arrow). The left temporal lesion is entirely solid, and the vein of Labbe is seen traversing along the tumour (white arrow).
An initial diagnosis of metastatic PEComa to the brain was made. The patient underwent excision of both lesions via left posterior temporal and right cerebellar craniotomy using intraoperative CT image guidance in a single setting. The right temporal tumour was greyish, vascular and friable, contained within a loosely adherent pseudocapsule, excised en bloc. The cerebellar tumour was excised en bloc in a similar manner. Intraoperatively, no macroscopic parenchymal invasion was noted and clear excision margin confirmed with intraoperative CT scans.
Histopathological sections of the specimens showed sheets, clusters and haphazardly dispersed spindled and epithelioid tumour cells (Figure 3(a)). These cells exhibited pleomorphic vesicular nucleus with occasional prominent nucleolus, as well as moderate to fairly abundant clear to faintly granular cytoplasm. In certain areas, the tumour cells were seen closely aggregated around blood vessels (Figure 3(b)). Mitotic figures were easily seen. Foci of necrosis were present. There was no evidence of keratinization or gland formation.
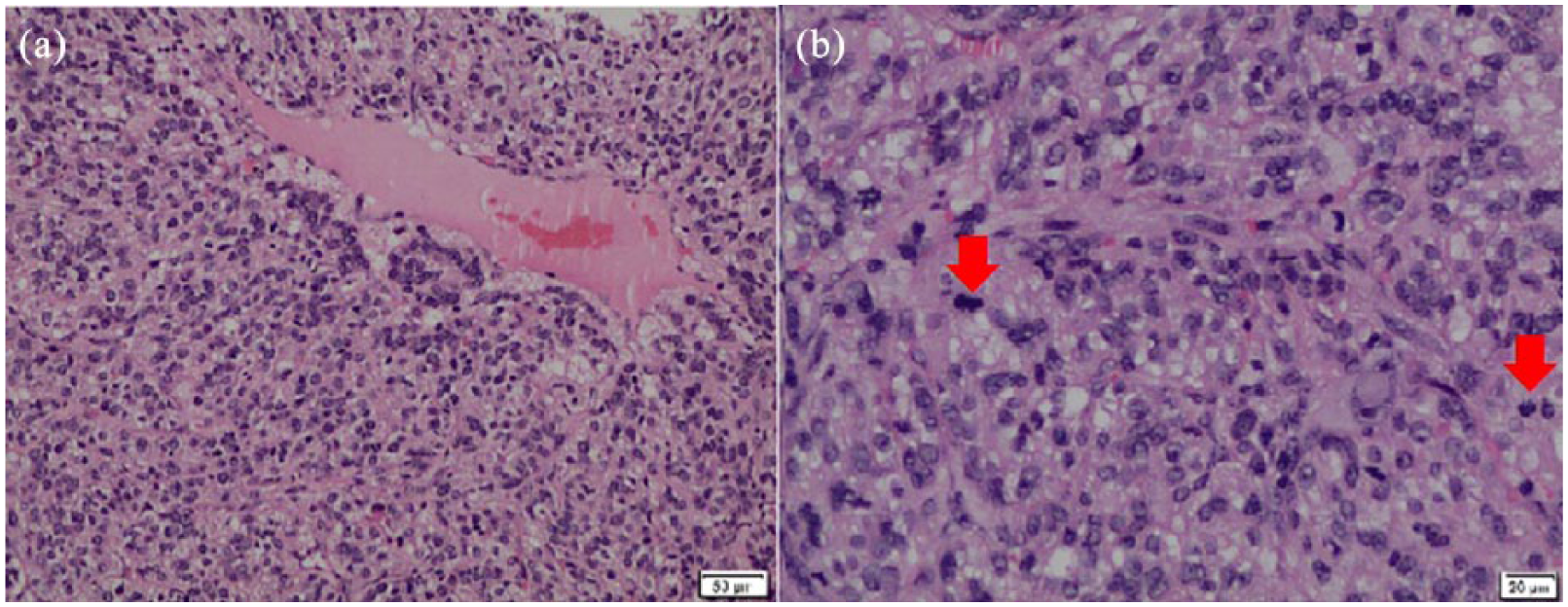
(a) Tumour cells clustering around a blood vessel: haematoxylin and eosin (original magnification: 10× objective), (b) spindle and epithelioid tumour cells with increased mitotic activity (red arrow): haematoxylin and eosin (original magnification: 20× objective).
Immunohistochemistry revealed focal positivity for HMB45 (Figure 4(a)) and showed weak smooth muscle actin positivity (Figure 4(b)). Ki67 proliferative marker was more than 30% (Figure 4(c)). These tumour cells were negative for epithelial membrane antigen (EMA), S100, CD10, CD34 and CD117.
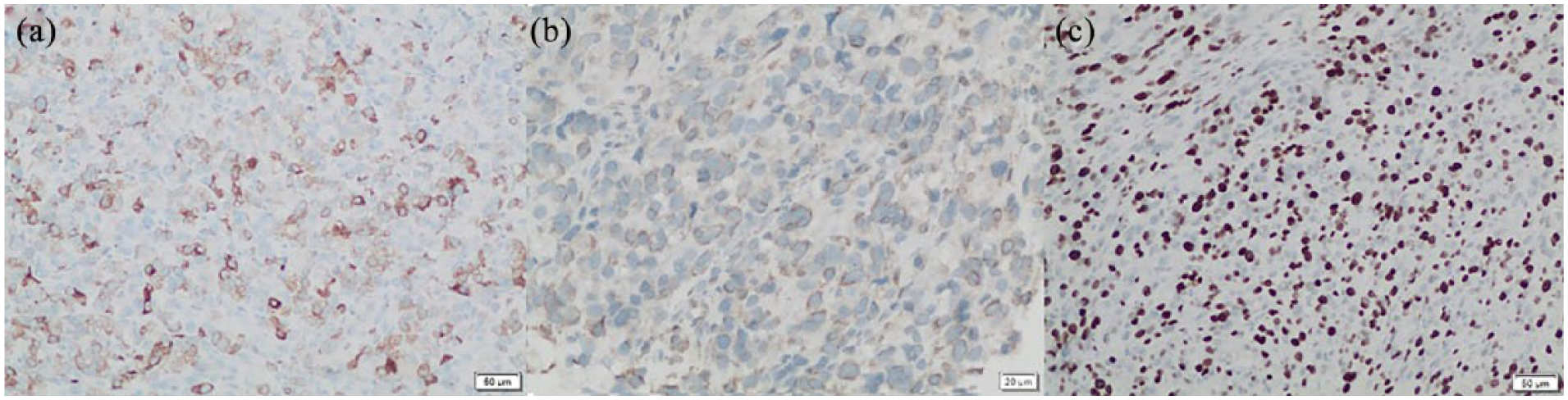
(a) Tumour cells showing positivity for HMB45 (original magnification: 10× objective), (b) smooth muscle actin; SMA (original magnification: 20× objective) and (c) high Ki67 proliferative index (original magnification: 10× objective).
These findings were compatible with metastatic PEComa.
Discussion
The World Health Organization Classification of Tumours of Soft Tissue and Bone (2013) defines PEComa as part of a family of mesenchymal tumours composed of distinctive perivascular epithelioid cells. 4 They are known to develop from various anatomical sites although the cell of origin is still unknown. 5 The malignant potential of PEComa correlates closely with the pathology of the primary tumour irrespective of the site of origin. Any combination of markers for an aggressive tumour such as infiltrative growth, marked hypercellularity, hyperchromatic nuclei, high mitotic activity, atypical mitotic figures, coagulative necrosis and a high Ki67 index suggests that the primary PEComa is likely to be malignant.1,4
Based on risk stratification guidelines for malignant PEComa as laid out by Bleeker et al., 1 primary tumour site > 5 cm and a high mitotic rate (1/50 hpf) were associated with recurrence following resection at the primary site. However, the time taken for occurrence of recurrence or metastasis in these patients is not well established due to its rare nature. Early identification of patients who are at risk as well as early detection of recurrence or metastasis based on the above criterion may improve outcomes for these patients.
The common sites for metastasis of PEComa includes the lung, bone, liver and lymph nodes.1,4,7 Brain metastasis of PEComa was not known to occur until it was first reported by Parfitt et al. 3 describing much on immunohistochemical findings. Furthermore, it has also been postulated that the reason for the sparing of the central nervous system could be due to the blood–brain barrier, which prevents free migration of tumour cells.
The primary duodenal PEComa in our patient was diagnosed using a positron emission tomography (PET) scan retrospectively after the discovery of the lung lesion by a chest CT, since her initial presentation was due to respiratory symptoms. PET scan, which is useful in identifying occult metastasis, did pick up the primary site of tumour in this case. Unfortunately, the naturally increased uptake of fluorodeoxyglucose (FDG) in the grey matter of the brain renders PET scan insensitive in picking up brain metastasis. 6 At the time of presentation, it is unknown whether the brain lesions were already present in our case, considering the fact that most patients with brain metastasis may remain asymptomatic. The presence of other extracranial metastasis (the lung lesion in this case) should alert the clinician to actively look for possible cranial metastases by including a CT/MRI of the brain as a routine screening tool along with the PET scan. Early diagnosis of brain metastasis is imperative as it affects the outcomes of patients undergoing adjuvant therapy post resection.
Conclusion
Metastatic PEComa to the brain is extremely rare. However, patients who are stratified as high risk should undergo an early MRI/CT of the brain in addition to a whole-body PET scan, to allow for early detection and management of these tumours.
Footnotes
Acknowledgements
All the authors have contributed equally in preparing this article with no other assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for her anonymized information and images to be published in this article.