
Abstract
Percutaneous endoscopic gastrostomy tubes are often placed in patients with head and neck malignancy for long-term nutritional support. Though rare, head and neck squamous cell carcinoma can metastasize to the percutaneous endoscopic gastrostomy tube site and may initially present as a developing mass or as bleeding at the percutaneous endoscopic gastrostomy site. Patients with head and neck squamous cell carcinoma should be evaluated diligently before and after percutaneous endoscopic gastrostomy placement in order to avoid this rare but life-threatening complication. We present a case of tongue squamous cell carcinoma that metastasized to the percutaneous endoscopic gastrostomy tube site causing gastrointestinal bleeding.
Introduction
Head and neck squamous cell carcinoma (HNSCC) is a leading cause of cancer in the world, and its incidence is predicted to increase by 30% by 2030. 1 Although it is largely considered a locoregional disease, HNSCC has the potential to metastasize, with the lungs being the most common site for metastasis, followed by bone and liver. 2 One of the most common long-term sequelae of HNSCC treatment is dysphagia following chemoradiation, which generally warrants enteral nutrition support via percutaneous endoscopic gastrostomy (PEG) placement. 3 HNSCC patients account for about 5% of all PEG tube placements in the United States. 4 It is generally a safe and effective feeding modality in patients requiring long-term nutritional support. 5 In rare cases, HNSCC may metastasize to the PEG tube site, although the exact mechanism remains unclear. Patients with PEG tube metastasis generally have a poor prognosis, with 1-year survival estimated at 35.5% and an overall mortality rate of 87.1%. 6
Case presentation
A 55-year-old female patient with a history of diabetes mellitus, hypertension, and stage IV squamous cell carcinoma (SCC) of the right tongue presented with 2 days of bleeding from her PEG tube site. The patient initially presented with a right tongue mass 1 year prior and was subsequently diagnosed with SCC of the tongue with metastases to the liver, lungs, and vertebrae. She underwent near total glossectomy, right radial neck dissection, left modified neck dissection, radiation therapy, and ongoing chemotherapy. She had a PEG tube placed for nutritional support 6 months prior to this presentation.
Computed tomography (CT) angiogram of the abdomen revealed a fluid collection abutting the anterior wall of the stomach, extending into the subcutaneous fatty tissues measuring 6 cm × 5 cm with peripheral enhancement (Figure 1). Esophagogastroduodenoscopy (EGD) images from the initial PEG tube fistula opening can be seen in Figure 2(a). A repeat EGD was performed to rule out alternate causes of bleeding and to evaluate the fistula site, which revealed circumferential mucosal changes with slight oozing of blood noted in the fistula, concerning for malignancy (Figure 2(b)). The mass was subsequently biopsied and pathology results revealed metastatic SCC. The PEG tube was removed and a jejunostomy tube (J-tube, Cook Medical) was placed surgically. Given the extent of metastatic disease and poor functional status, the patient was transitioned to hospice care and passed away shortly after.

CT angiogram of the abdomen revealed a fluid collection abutting the anterior wall of the stomach, extending into the subcutaneous fatty tissues measuring 6 cm × 5 cm with peripheral enhancement (red arrow).
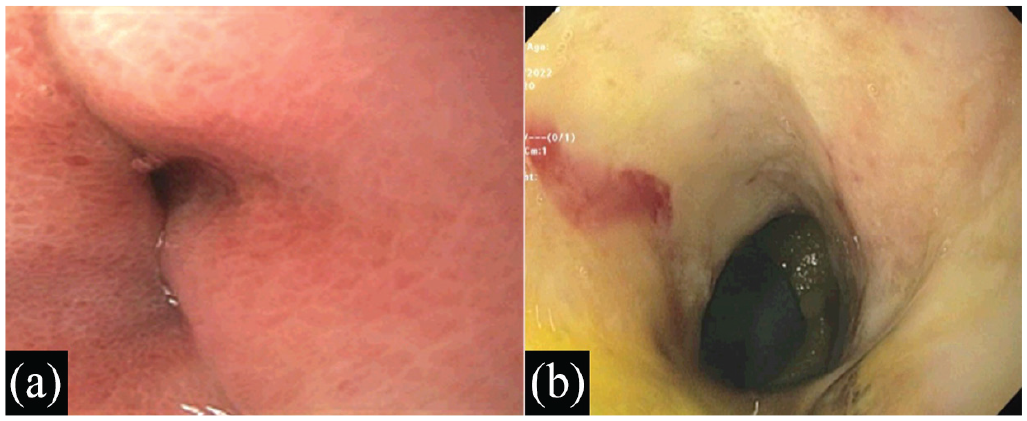
(a) Prior PEG tube fistula opening at the gastric body. (b) EGD, at the time of diagnosis, revealing circumferential mucosal changes within the fistula tract, concerning for malignancy.
Discussion
Chronic malnutrition affects approximately 20%–57% of patients with HNSCC. 7 Weight loss and malnutrition prior to and during cancer treatment portend poor outcomes and treatment difficulties. Enteral nutrition in the management of head and neck cancers is vital for treatment success. Since it was first described by Gauderer et al. 8 in 1980, PEG tube placement and utilization rate has increased from 15,000 per year in the United States to 200,000 per year and has become the preferred route in patients requiring long-term nutrition support. 9 Despite this increase, the incidence of PEG site metastasis from oral cancer remains low, estimated at 0.5%–3%. 4
In 1989, Preyer et al. 10 described the first case of PEG site metastasis from an oropharyngeal primary HNSCC. Since then, the complications of incidental seeding of the gastric or abdominal wall following PEG have become a developing concern. Patients can present with abdominal pain, grossly evident tumor emanating from the abdominal wall, bleeding from the PEG tube site, ulceration and constipation. Due to paucity of cases, the exact pathogenesis remains unknown, but several theories have been proposed. Among the potential mechanisms of metastasis are direct implantation of malignant cells at the time of tube placement, hematogenous spread in which circulating tumor cells select traumatized tissue of the PEG site, and physiological shedding of cancer cells into the alimentary tract with seeding the PEG site after tube placement.4,11
To avoid PEG tube seeding, many procedural recommendations have been made based on the proposed pathogenesis theories. PEG tubes are usually placed through the “pull technique” or “push technique.” Both the methods involve pulling or pushing the tube through the oropharynx in the stomach using an endoscopically placed guide wire, which runs from the mouth through the stomach and anterior abdominal wall to the stomach. 12 As the majority of reported cases of PEG site metastasis are associated with the Gauderer–Ponsky technique (96.6%), the authors have suggested the use of alternate techniques. 12 These techniques include Russell (transabdominal introduction of gastrostomy tube under endoscopic visualization), Sacks-Vine (blind pulling of the feeding tube through the abdominal wall via the mouth under nasogastric stomach insufflation), or radiologic-assisted to avoid passage of the feeding tube or endoscope past the site of the tumor. 12
In addition to alterations in the technique, procedure timing changes should be considered. Changing the timing of PEG tube placement in relation to HNSCC therapy has been analyzed as a potential strategy for preventing stomal metastases. A study by Keim et al. 13 analyzing peristomal recurrence of SCC following total laryngectomy found that the sole significant risk factor for the occurrence with direct stoma implantation of tumor cells is pre-laryngectomy tracheostomy. This theory can be further extended to early PEG tube placement in patients with HNSCC. Further research into deferring PEG placement until after starting radiotherapy is warranted.
Conclusion
This case emphasizes that PEG tube site masses should be evaluated carefully as they can be the first sign of metastasis. Given the associated morbidity and mortality, clinicians should be aware of this life-threatening complication in order to initiate timely and appropriate management.
Footnotes
Acknowledgements
None to report.
Author contributions
Hunza Chaudhry and Humzah Iqbal reviewed the literature, drafted the manuscript, revised it for important intellectual content and were involved in the final approval of the version to be published. Amitpaul Gill, Alakh Gulati, and Juliana Yang revised the article for important intellectual content and were involved in the final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient’s legally authorized representative for their anonymized information to be published in this article for all cases.