
Abstract
Cancer-related fatigue is a common symptom in cancer patients which commonly occurs in relation to sleep disturbance. We report a case of a 35-year-old breast cancer survivor, in whom polysomnography and multiple sleep latency testing were utilized to objectively quantify the contribution of excessive daytime sleepiness to the patient’s cancer-related fatigue.
Keywords
Introduction
Fatigue is commonly reported in cancer patients during treatment. 1 Although validated surveys exist, fatigue may be subjective and difficult to quantify. The persistence of fatigue not relieved with rest is consistent with cancer-related fatigue (CRF), and it may precede, coexist, or develop after cancer diagnosis and therapy. 2 Criteria for the diagnosis of CRF includes exclusion of concomitant metabolic or psychiatric abnormalities, functional limitations, and other symptoms. 2 Hypersomnia and insomnia are contributors to CRF. 3 We present a case in which the primary complaint was daytime sleepiness with subsequent confirmatory testing and treatment.
Report of case
A 35-year-old woman with a history of breast cancer presented with severe fatigue and excessive daytime sleepiness (EDS). The patient did not report these symptoms prior to her diagnosis with a T2N1M0 triple negative invasive ductal breast carcinoma. The patient received neo-adjuvant chemotherapy consisting of four cycles of paclitaxel and four cycles of FAC. After neo-adjuvant therapy, the previous 3 cm by 2 cm mass was imperceptible on mammography and a single enlarged lymph node had reduced in size by 55%. She had a segmental mastectomy with axillary node dissection and received radiation therapy. The right breast was treated with a dose of 50 Gy in 25 fractions. CRF was initially evaluated at a designated Fatigue Clinic at MD Anderson Cancer Center, 4 years after treatment. Sleep schedule was regular, consistent, and between 7 and 9 h per night. She denied snoring, witnessed apneas, restless legs, hypnopompic and hypnogogic hallucinations, sleep paralysis, and cataplexy. Epworth Sleepiness Scale (ESS) score was 14, consistent with moderate EDS.
She continued working full time with good social support. Past medical history was significant for hypothyroidism and hypertension. She did not smoke or drink alcohol, and she denied any pain, anxiety, or depression. Her CRF had been managed with daily exercise therapy (30 min) and modafinil (100 mg). Physical examination was unremarkable aside from a body mass index (BMI) of 31 kg/m2. Laboratory studies revealed no anemia, and thyroid-stimulating hormone (TSH) was normal (3.74 µIU/mL). The patient’s Brief Fatigue Inventory (BFI) score was 6.3 (0–10), congruent with moderate fatigue, and ESS score was 14 (0–24) and supported hypersomnia.4,5
The patient was referred to the Sleep Center at MD Anderson Cancer Center 1 month later for persistent hypersomnia. After cessation of her stimulant medication for 2 weeks, polysomnography (PSG) and multiple sleep latency test (MSLT) were performed. The PSG is a tool that can be used to evaluate sleep quality and diagnose sleep disorders which may fragment and impair sleep such as sleep apnea or periodic limb movement disorders. It revealed a total sleep time of 483 min with 4% N1 sleep, 69% N2 sleep, 27% rapid eye movement (REM) sleep, but no N3 sleep. Sleep efficiency was 97%, latency to persistent sleep was immediate, and latency to REM sleep was normal (77 min). There were no apneas, hypopneas, desaturations, or limb movements consistent with the diagnosis of sleep apnea or periodic limb movement disorder.
The images represent the results of the MSLT and sleep onset latency. The MSLT consisted of four naps which began 2 h after waking and continued at 2-h intervals throughout the day. The MSLT demonstrated sleep in all four naps; however, sleep onset REM periods did not occur (Figure 1(a)). MSLT confirmed hypersomnia with a mean sleep latency of 4.4 min, well below the threshold for the diagnosis of hypersomnia (Figure 1(b)).
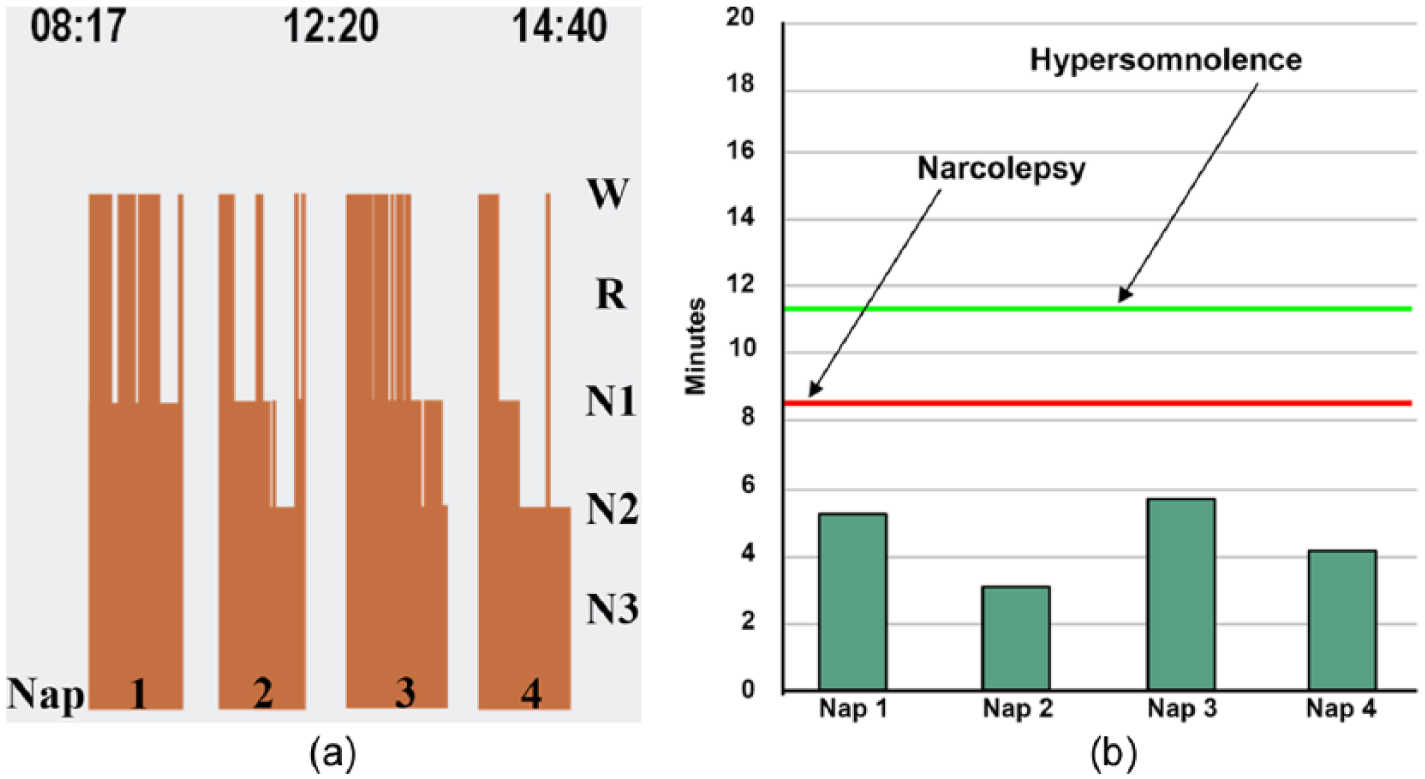
(a) During the multiple sleep latency test, four naps were conducted at 2-h intervals 2 h after the patient awoke from nocturnal sleep. Results demonstrated sleep onset in all 20-min nap periods from the morning into the mid-afternoon. Sleep-onset REM periods (SOREMPs) were not present. (b) The mean sleep latency was 4.4 min and below the diagnostic threshold for narcolepsy (8 min) or idiopathic hypersomnia (11 min).
Modafinil was increased with significant symptomatic improvement and after 3 months, the BFI score decreased to 2, and Epworth Sleepiness Score decreased to 4.
Discussion
We present a case of CRF with EDS with subsequent confirmatory testing. Although not standard in the routine diagnosis of CRF, PSG and MSLT allowed diagnosis and quantification of hypersomnia as well as the exclusion of other primary sleep disorders. Resolution of symptoms with treatment further confirmed the diagnosis.
CRF is a distressing, persistent subjective sense of physical, emotional, and/or cognitive tiredness or exhaustion related to cancer or cancer treatment that is not proportional to recent activity and interferes with normal functioning. 1 The etiology of CRF is multifactorial and is related to cancer and cancer treatments such as chemotherapy and radiation, particularly when targeting the central nervous system, but even when systemic. 2 Opioids and other sedating medications, hypothyroidism, physical deconditioning, medical and psychiatric comorbidities, and other psychosocial factors are commonly involved in CRF. 2 The evaluation of a patient with CRF should include an assessment of sleep quality. 6 Sleep disturbance may be a major contributor to CRF, but this has been difficult to objectively measure. 7 In fact, it is difficult to discriminate between the subjective symptoms of CRF and EDS. MSLT offers a means by which to measure daytime sleepiness with shorter mean sleep latency indicating greater sleepiness. 8
In our case, CRF and EDS were coincident and related. This relationship is not surprising, as it is postulated that aberrant circadian rhythms and inflammation may be a common mechanism for fatigue and hypersomnia in oncologic patients.9,10 In a select population, PSG with possible MSLT may provide a definitive diagnosis.
Conclusion
EDS may contribute to CRF, and its effect can be objectively measured by MSLT. In addition, PSG is helpful in ruling out primary sleep disorders in patients with CRF. Finally, evaluation of sleep disturbance should be considered in patients with CRF.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.