
Abstract
Objective:
To present a case of successful repair of a spontaneous cerebrospinal fluid leak in a previously unreported anatomic site.
Methods:
Retrospective chart review.
Results:
A 48-year-old woman developed a spontaneous cerebrospinal fluid leak from the optic nerve sheath and underwent a multilayer endoscopic closure with no damage to the optic nerve.
Conclusion:
Endoscopic surgeons can successfully repair cerebrospinal fluid leaks from the optic nerve sheath without causing loss of vision.
Introduction
Cerebrospinal fluid (CSF) rhinorrhea is caused by a defect in the normal bony and mucoperiosteal barrier separating the intracranial space from the paranasal sinuses, arising from a traumatic or atraumatic origin. Common locations for CSF leaks include the lateral lamella of the cribriform plate in the ethmoid skull base and the lateral sphenoid sinus. Here, we present a rare case of spontaneous CSF rhinorrhea in a previously healthy, obese, 48-year-old female arising from a defect in the right optic canal, a location that has not been previously reported as a source of CSF rhinorrhea in the literature. We review this literature, the anatomy of the subarachnoid space of the optic nerve sheath, and the proper management and workup of suspected spontaneous CSF rhinorrhea.
Case report
A previously healthy, obese, 48-year-old female presented with a 1-year history of clear fluid draining from the nose and associated dull headaches. The patient had no other signs of increased intracranial pressure (ICP) such as vision changes or papilledema on history and physical exam. Beta-2 transferrin testing of the fluid was positive, indicating a CSF leak. Computed tomography (CT) scan of the sinuses showed near-complete opacification of the sphenoid sinus with an air fluid level, small amount of fluid in the posterior nasal cavity, and a small focal bony dehiscence of the optic canal in the superior sphenoid sinus with adjacent pneumocephalus (Figure 1). Coronal T2-weighted magnetic resonance imaging (MRI) also showed the site of leak at the optic canal in the right sphenoid and did not show encephalocele or meningoencephalocele (Figure 2). She underwent endoscopic repair of the CSF leak via a unilateral transsphenoidal approach.

Non-contrast coronal CT of bony defect in optic canal and opacification in right sphenoid sinus.

Pre-operative coronal T2-weighted MRI showing CSF leak without meningoencephalocele from the right optic nerve canal in the right sphenoid sinus.
A lumbar drain was placed to start the case for use post-operatively and to allow for the use of intrathecal fluorescein in case the defect could not be visualized intraoperatively. However, fluorescein was not needed due to endoscopic confirmation of the site of the leak as the optic canal in the sphenoid roof (Figures 3 and 4). Surrounding mucosa was removed and bone edges were prepared carefully with a diamond drill. Preparation of the bone was performed in a delicate manner with blunt-tipped instruments given the sensitive position of the defect adjacent to the optic nerve. Repair was performed in a multilayer fashion with a small piece of abdominal fat, mucoperiosteal free graft from the middle turbinate, and packing with bovine microfibrillar collagen, compressed gel foam, and merocel sponge packing. Patient was noted to have normal vision immediately after surgery. Lumbar drain was removed on post-operative day #2 without complications. Her post-course was uneventful. She returned to work 6 weeks after surgery. She remains free of CSF rhinorrhea 24 months after surgery and continues to have normal vision. No post-operative imagine was performed due to our ability to monitor the right sphenoid cavity endoscopically, which continues to show no evidence of recurrent CSF leak.
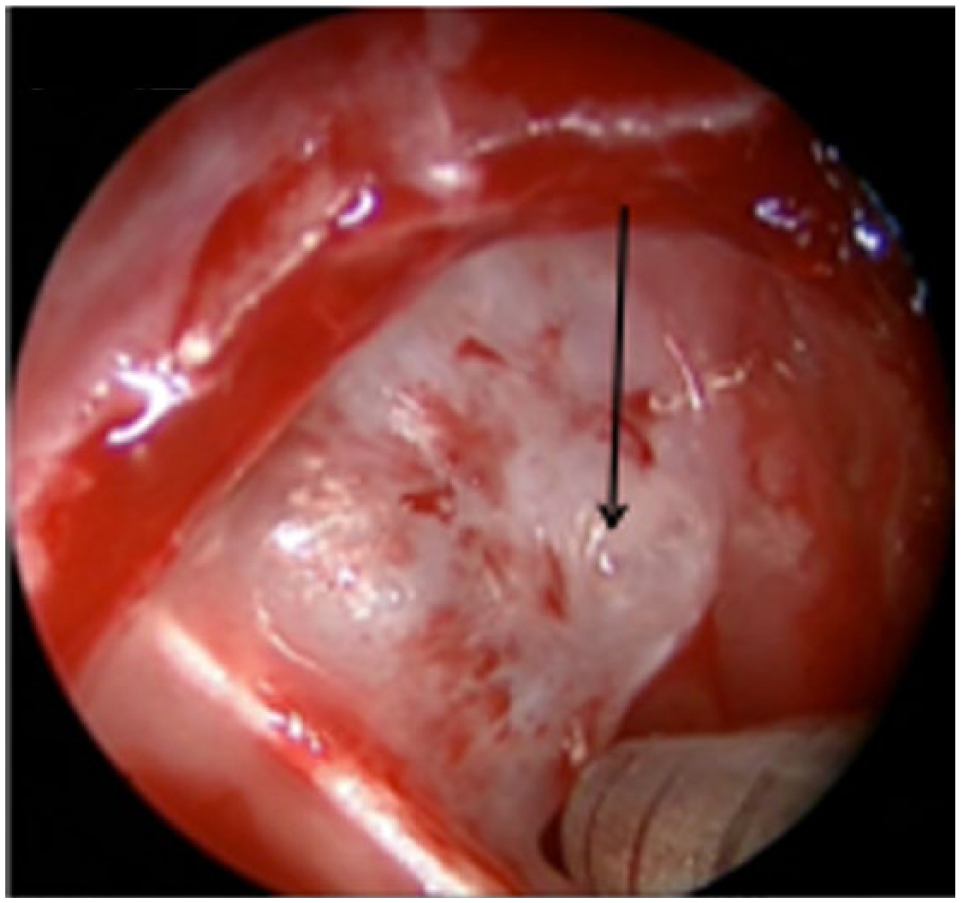
Intraoperative endoscopic view of right sphenoid sinus with hydrodissection of sphenoid mucosa off of the bone by the CSF leak. There was no encephalocele.
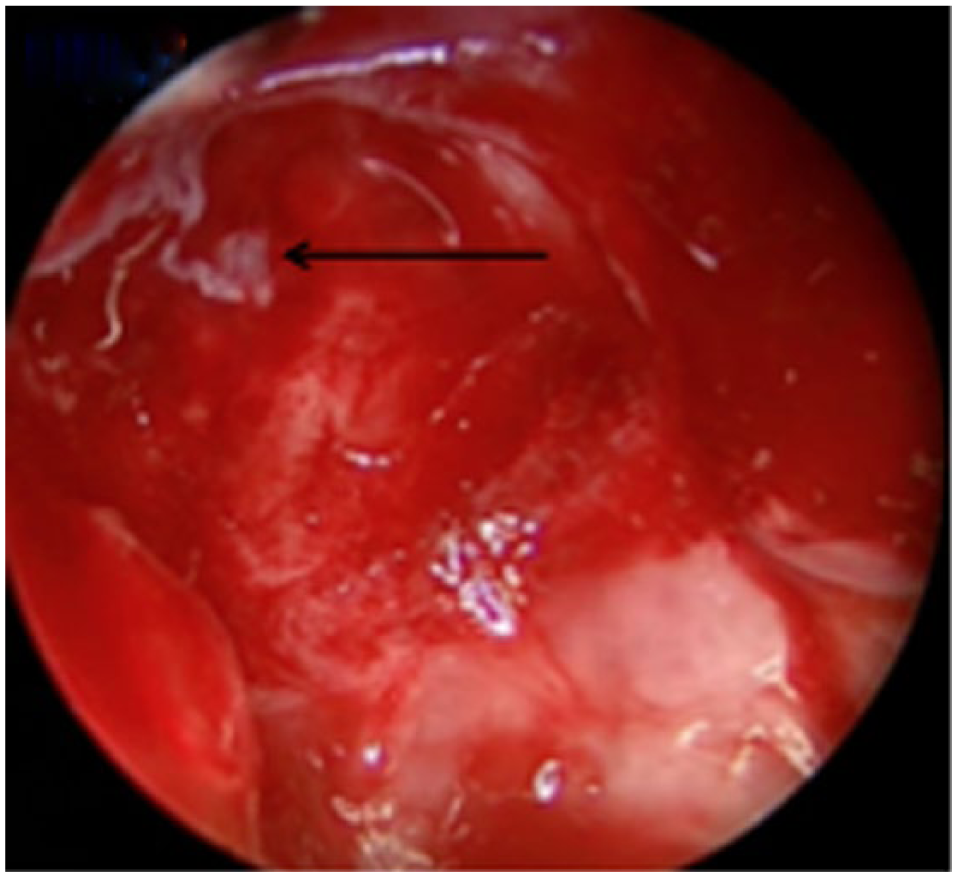
Endoscopic view of defect in optic canal in right sphenoid sinus after removal of mucosa. Small bone defect without encephalocele.
Discussion
CSF rhinorrhea is divided into traumatic and atraumatic categories based on the etiology of the leak, with traumatic leaks being most common. 1 Spontaneous leaks, a type of atraumatic leak as presented in this case report, are most commonly due to skull base defects in the ethmoid bone or the lateral wall of the sphenoid sinus such as the pneumatized spheno-pterygoid recess. 2
Spontaneous CSF leak originating from the optic canal is a rare site which has not been previously reported in the literature. Although the etiology of spontaneous CSF leaks is likely due to a combination of bony anatomy and functional processes, it has been noted in the literature that there are many similarities between the demographic of patients presenting with spontaneous CSF leaks and those with disorders associated with increased ICP like pseudotumor cerebri and empty sella syndrome. 3 It is known that the meninges extend anteriorly through the optic canal and fuse with the sclera of the eyeball such that the intracranial subarachnoid space is contiguous with the intraorbital subarachnoid space. Thus, the subarachnoid space extends anteriorly along the optic nerve sheath where it terminates as the dura and arachnoid fuse with the periosteum of the orbital cavity. This fact has been further characterized by showing dilated optic nerve sheaths on MRI in patients with idiopathic intracranial hypertension. 4 This subarachnoid space along the optic nerve sheath is the site of the CSF leak in this report. CT confirmed a small bony defect, and MRI confirmed that there was no encephalocele or meningoencephalocele.
The workup for a suspected CSF rhinorrhea should include an initial attempt to document CSF within the paranasal sinuses, such as by testing for Beta-2 transferrin. Second, for a confirmed case of CSF rhinorrhea, or when testing remains negative in the face of high clinical suspicion, a high-definition CT scan of the head remains the imaging modality of choice. The greater soft tissue detail provided by MRI can be useful if the involvement of a soft tissue defect like meningocele is suspected. The indications for the use of a lumbar drain remain controversial, but we have found that it is a valuable tool when a suspected CSF leak cannot be localized and the use of intrathecal fluorescein is desired, or in patients with a high likelihood for post-operative increased ICP who may benefit from a period of CSF diversion.3,5 For the repair of spontaneous CSF rhinorrhea, we prefer a multilayer closure with mucosal free graft with or without abdominal fat graft as a first line option, preserving a nasoseptal flap for instances of leak recurrence or for large defects.
CSF rhinorrhea originating in the optic canal presents challenges both in terms of delicate preparation of surrounding bone and in limited intracranial space that can be involved in repair. For example, grafts used for optic canal defects must be overlaid on the defect to avoid optic nerve compression instead of placed partially within the defect as with the more common dumbbell or underlay graft repair, as is commonly employed for ethmoid skull base and lateral sphenoid skull base defects. Finally, it is important to include a thorough ophthalmologic evaluation along with standard post-operative follow-up for patients undergoing surgical repair of defects involving the optic canal.
Conclusion
Spontaneous sphenoid sinus CSF leaks typically arise from the lateral pterygoid recess or the planum sphenoidale. Spontaneous CSF leak from the optic canal has not been previously reported, but represents a unique cause of CSF rhinorrhea requiring careful surgical management to prevent a persistent leak or iatrogenic damage to vision. This case report presents a strategy for successful repair of a CSF leak involving the optic canal with the use of a mucosal free graft and multilayer closure with packing which resulted in closure of the defect and avoidance of injury to the optic nerve.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for case reports
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.