
Abstract
Meticulous history taking and careful examination should always be performed in all patients because a common symptom, such as sore throat, could be a presentation of an unusual problem. Sore throat from an ingested foreign body can perforate the mucosa and migrate extraluminally penetrating vital structures of the neck. Rare documentation of such cases involves sharp objects and, if untreated, may result in life-threatening complications. This article presents a case of a patient with a 3-week history of sore throat, and diagnostic work-up revealed a sharp metallic foreign body (needle pin) in the hypopharynx, which migrated extraluminally through the posterior pharyngeal wall. There were no signs or lesions on endoscopy to help point the exact entry point and location of the foreign body. Intraoperative imaging using C-arm was used to identify the exact position of the foreign body, which was at the level of C4, 0.5 cm deep to the right lateral posterior pharyngeal wall mucosa, and oriented lateral to the vertebra. The needle pin was subsequently extracted.
Keywords
Objectives
(a) To present a rare course of foreign body ingestion;
(b) Increase awareness for diagnostics and treatment modalities of extraluminal foreign bodies.
Methods
(a) Study design: case report;
(b) Setting: tertiary private university hospital;
(c) Subjects, participants, patients, or population: patient.
Literature search from scientific journals consisting of original research articles, review articles, and case reports from NCBI, MEDLINE, MESH, PubMed, ScienceDirect-Elsevier, HERDIN, and PJO-HNS using the search terms “foreign body” and “migrating foreign body” has shown a cumulative of 3588 search results and only 67 cases of ingested foreign body that migrated extraluminally. This study being the 68th case and the first in the Philippines.
Introduction
Foreign body ingestion can imitate symptoms of other conditions and cause delay in management that may lead to debilitating and life-threatening complications. Foreign bodies can become lodged in the tonsil, base of tongue, pyriform sinus, and cervical esophagus. However, there has been rare documentation of foreign bodies penetrating the mucosa wall of the aerodigestive tract and migrating into the soft tissue and viscera of the neck. 1
Case description
The patient is a 57-year-old, male, farmer with no known co-morbidities, from Laguna Province, Philippines, who consulted after 3 weeks history of odynophagia. Before he consulted in our institution, the patient has sought previous consult and was diagnosed and treated for pharyngitis. Despite his compliance with oral antibiotics prescribed by his previous physician for 2 weeks, his odynophagia persisted. A week prior to admission the patient consulted an otorhinolaryngology outpatient clinic. At that time, the patient was signed out as a case of acute tonsillopharyngitis. He was advised to continue antibiotics and follow up closely if symptoms persisted or progressed. Due to the persistence of symptoms, the patient was instructed to consult in a tertiary hospital and was thus referred to our institution. A thorough history was taken and a detailed examination was done. It was only after this the patient recognized that a needle pin was missing and might have been accidentally incorporated in a cooking pot in their home. It was after eating from that cooking pot that he started feeling the sharp pain he felt during swallowing, which persisted up until his eventual admission.
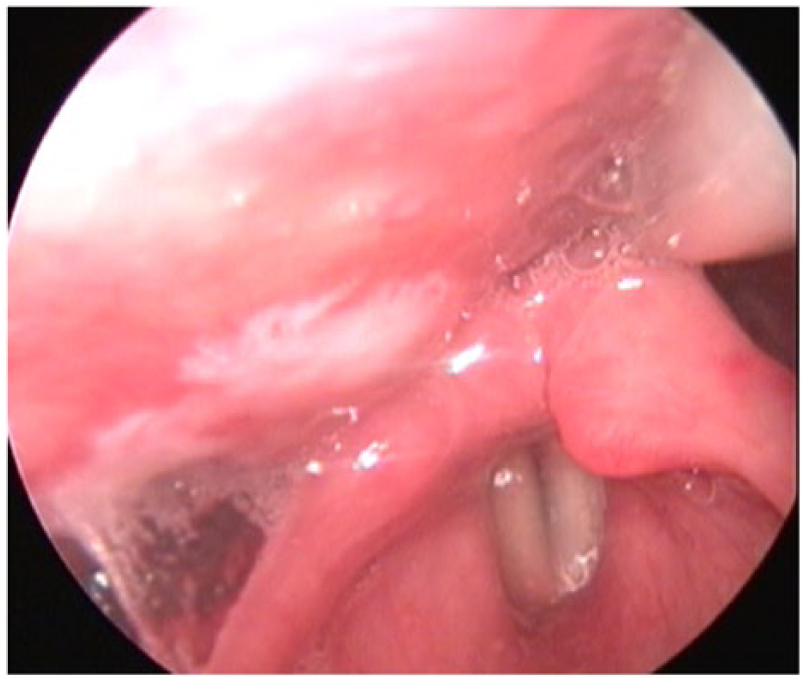
Upon admission, cervical X-ray was done and both anteroposterior (AP) and lateral views were studied to determine the current location of the foreign body (Figure 1). The radiograph revealed the foreign body at the right paramedian region at the level of the C4 vertebral body, located just above the pyriform sinus oriented superolateral. Rigid video laryngoscopy was also done where no mucosal lesion was noted even at the supposed location of the foreign body at the right posterior pharyngeal wall above the pyriform sinus where the foreign body was located in the radiologic examination (Figure 2). There is no pooling of saliva in the pyriform sinus, no signs of irritation, or infection in the hypopharyngeal mucosa. Arytenoids are non-hyperemic and non-edematous, and true vocal folds are symmetric with sharp edges.

Lateral and anteroposterior (AP) radiograph upon admission.

Video laryngoscopy, postoperatively exploring the hypopharynx with emphasis on right posterolateral pharyngeal.
The patient was immediately scheduled for emergency direct laryngoscopy, possible rigid esophagoscopy with foreign body extraction under general anesthesia. Antibiotics cefuroxime 750 mg/amp, 1 amp q12, and metronidazole 500 mg/amp, 1 amp q8 were started.
Upon insertion of the laryngoscope intraoperatively, the hypopharynx was explored. Difficulty was encountered, as there were no identified signs or lesion in the pharyngeal lumen indicating the point of entry or location of the foreign body. With the aid of the C-arm positioned AP to the supine patient, the level and laterality of the foreign body was identified at the level of C4 oriented at right lateral posterior pharyngeal wall and lateral to the vertebra (Figures 3 and 4). The posterior pharyngeal wall was incised with 1 cm length and 0.5 cm depth. The head of the foreign body (needle pin) was visualized and was extracted using laryngeal forceps. Nasogastric tube (NGT) was inserted and patient was placed in nil per os (NPO)/nothing through the mouth postoperatively.

Intraoperative view of C-arm fluoroscopy directed lateral to the patient.

Intraoperative view of C-arm fluoroscopy directed anteroposterior to the patient.
A cervical spine X-ray postoperatively was taken showing the absence of any foreign body. At the 3rd post-op day, repeat chest X-ray was done and repeat video laryngoscopy showed granulation tissue at the right pharyngeal wall at the level above pyriform sinus where the incision was made (Figure 5), there was no bleeding or hematoma. Arytenoids were non-hyperemic and non-edematous with full and equal true vocal fold (TVF) movement. Patient was then started on clear liquid diet per orem. NGT was removed and diet was progressed. Patient was then discharged.
Post-operative video laryngoscopy.
Discussion
Foreign bodies that have been ingested and perforated the mucosa of the aerodigestive tract and have migrated extraluminally are called “Migratory foreign bodies.” 1 Migratory foreign body is suspected based on the following: (1) suggestive history, (2) positive finding on lateral neck radiography, and (3) a negative finding on rigid endoscopy. 2 All of which are positive in the presented case. The presenting symptom of migratory or migrating foreign body ingestion could be misleading. Initial symptom varied from odynophagia, dysphagia, globus sensation, drooling and vomiting, drooling to respiratory symptoms of distress, shortness of breath, coughing, choking, and stridor to being completely asymptomatic. 3
Foreign bodies that are sharp and horizontally oriented have a higher chance of penetrating the mucosa of the aerodigestive tract. In a previous study by Remsen et al. 4 dating back to 1983, a series of 321 cases of penetrating foreign bodies were reviewed and 43 were found extraluminally. Their conclusion was that sharp foreign bodies have a higher risk of mucosal penetration and extralumen migration. Chee and Sethi 5 in 1999 reported 24 migrating foreign bodies in the neck; their findings were consistent in that all of the foreign bodies in their study were sharp and linear. These findings are also true in the case of this study, where the foreign body is a sharp and linear needle pin.
The phenomenon of migration of ingested foreign body from the aerodigestive tract lumen is caused by the repeated contraction of the hypopharyngeal and cricopharyngeal muscles during swallowing as they propel a food bolus into the esophagus. Complications of foreign body migration depend on the direction and site of migration. They may vary from inflammation, infection, deep neck abscess that could spread to the mediastinum, and damage to adjacent structures. All of which can lead to penetration of the major blood vessels causing fistulas, sepsis, blood vessel rupture, and death. 6
A thorough endoscopy and computed tomography (CT) scan of the neck with and without oral contrast are the gold standard for diagnosis. 7 Pre-operative imaging is tantamount in locating a foreign body that has migrated. X-rays of lateral neck are useful in determining the current location of a foreign body but do not establish if migration has occurred. 8 A CT scan can be used to localize the foreign body and assess the extent of damage the migrating foreign object has done. CT scan image of 1 mm cuts is the recommended investigation of choice of some studies because it can identify thin, small, and minimally calcified foreign bodies, which is difficult to identify by plain X-ray radiographs. CT scan also serves as a map which will aid the surgeon with the size, orientation, and relationship to other vital structures. The position of the neck during CT scan and surgery may not be the same because soft tissues of the neck are mobile in relation to the bony and cartilaginous structures so it should be kept in mind that the position of the foreign body may not be the same during surgery as seen on CT scan. Oral contrast can also be utilized to check if the foreign body is distinctly separate from the lumen. Barium swallow is useful in detecting esophageal leak but its value is limited in localizing the foreign body. 7 Use of C-arm to localize the foreign body in the neck intraoperatively is also recommended if the foreign body is not found where it is seen in pre-operative imaging. Intraoperative radiograph is useful especially in cases where the foreign body is embedded within the muscles.
The treatment of choice for airway and esophageal foreign bodies is endoscopic removal. 9 Exploration and early removal of the migrated foreign body via external approach is also recommended depending on how far from the lumen the foreign body has migrated into. 2 In this case, however, fluoroscopy enabled the surgical team to identify the embedded needle pin in real time. Suspension combined with fluoroscopy allowed for an image-guided minimally invasive technique performed under direct magnified visualization. This approach is favored over the open surgical technique. 10
Removal of these foreign bodies should be done with precise localization and visualization, and fluoroscopy and suspension should be considered prior to an external approach. Nasogastric tube must be placed in all cases to allow for healing of the perforation while allowing feeding to continue. Barium swallow should be done to check for persistent esophageal perforation before removing the nasogastric tube. 7
Conclusion
A high index of suspicion is needed to recognize a migrating foreign body. History and physical examination is important in establishing the diagnosis and early intervention is crucial in such cases to prevent complications. Migration of foreign body is facilitated by voluntary and involuntary movement of neck muscles and viscera during swallowing. A thorough endoscopy and CT scan of the neck with and without oral contrast are the gold standard for diagnosis. A careful and systematic approach during exploration of the neck is needed. Intraoperative radiography can be of great help in locating the foreign body.
Footnotes
Acknowledgements
To Jean Rochelle M. Alonso, MD for her invaluable contribution in the improvement and revisions of critically important intellectual content that led to this publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.