
Abstract
Synovial chondromatosis is a benign disease which most commonly appears in large joints and only rarely affects the temporomandibular joint. The diagnosis is quite difficult due to the fact that a large swelling in the preauricular area and the radiographic findings may be misdiagnosed as other benign or malignant diseases. We report an unusual case of intra- and extracapsular chondromatosis of 25 osteochondral loose bodies in the right temporomandibular joint.
Introduction
Synovial chondromatosis (SC) is a rare benign lesion which includes osteochondral loose bodies and normally occurs in large joints such as the knee, elbow or hip. The temporomandibular joint (TMJ) is the rarest location of this disease. 1 The current literature review reveals only around 200 previous cases of SC affecting the TMJ.2,3 We report an unusual case of intra- and extracapsular chondromatosis of 25 osteochondral loose bodies in the right TMJ.
Case report
A 63-year-old woman was referred by her general medical practitioner to our Department for Oral and Maxillofacial Surgery. The patient noticed an increasing painful swelling in the right preauricular region during the past 2 years. The dental situation included a prosthetical insufficient treated status and a strong abrasion of the teeth most likely due to a supposed craniomandibular dysfunction. There was no previous history of trauma. One year before there had been an excision of a malignant melanoma (pT1a, cN0, cM0), in the skin of the left knee. The patient suffered from no severe disease besides arterial hypertonia and rhinoconjunctivitis allergica.
Performing an extraoral examination, there was a marked facial asymmetry with deviation of the chin to the left side and a remarkable bony hard swelling in the right condylar region. Mouth opening was possible with no pronounced clicking or crepitus.
The patient wore partial dentures with 5 own remaining teeth in the upper jaw and 9 remaining teeth in the lower jaw. The occlusion was an Angle Class I with correct denticulation but seemed to be a skeletal mandibular protrusion in the side profile clinically because of a prominent chin. The condyles itself looked similar in size and form (Figure 1).

Praeoperative orthopantomography of a 63-year-old patient with synovial chondromatosis of the right temporomandibular joint.
In the first sonography, unsharp circumscribed possibly calcified lesions could be seen in the cranial of the right caput mandibulae. There was no increased vascularisation to be found. Beside this, the TMJs on both sides were in a symmetric degenerative status.
The full extent of these lesions on the right side was defined more precisely by a computed tomography (CT) scan (Figure 2). Diverse loose calcified bodies which appeared to be within and outside of the right capsule could be recognized in form of a remarkable saculation to the medial direction.

Praeoperative CT scan of the lesion in the right temporomandibular joint.
In a separate performed magnetic resonance imaging (MRI), lesions could furthermore be described as a cystical diagnostic finding (Figures 3 –5). The suspected radiological differential diagnoses after CT and MRI was therefore an (ectopic) adenoma of the right parotid gland or a saculation of the joint capsule with calcifications. An evidence for a malignant lesion could not be pointed out in CT and MRI. Therefore, no further medical imaging was performed.

Preoperative MRI. Axial T2-weight slide. Praeoperative lesion surrounding the right temporomandibular joint.

Preoperative MRI: coronal slide, contrast-ehanced T1-weight—cranio-lateral surrounding of the TMJ by the lesion.

Preoperative MRI: Sagittal T2-weight-slide of the right TMJ showing the high intensity lesion.
Afterwards, a sonographically supported aspiration biopsy was performed to verify the final diagnosis: The cytological survey did not show any correlation to a malignant melanoma metastasis. The cells were suspected to be of benign tumor origins and most likely to stand in correlation to a pleomorph adenoma of the right parotid gland.
In view of these findings and the progressive swelling in the right TMJ, an open operative exploration was performed. The access was obtained by a right preauricular approach in order to gain enough exposure of the numerous small particles in the temporomandibular region. Twenty five loose bodies of different size were retrieved from the synovial space and interior of the capsule (Figure 6).

Twenty five loose bodies of different size retrieved from the synovial space and the inner TMJ-capsule.
Closure was performed in multi-layers and a mini suction drain was inserted. The macroscopic examination of the findings resulted in biggest pieces of 14 mm x 6 mm and all bodies seemed to be of chondroid origin. This was verified by the microscopic examination which revealed all bodies to be of calcified chondral origin with regressive changings with characteristics most likely of a SC (Figure 7).
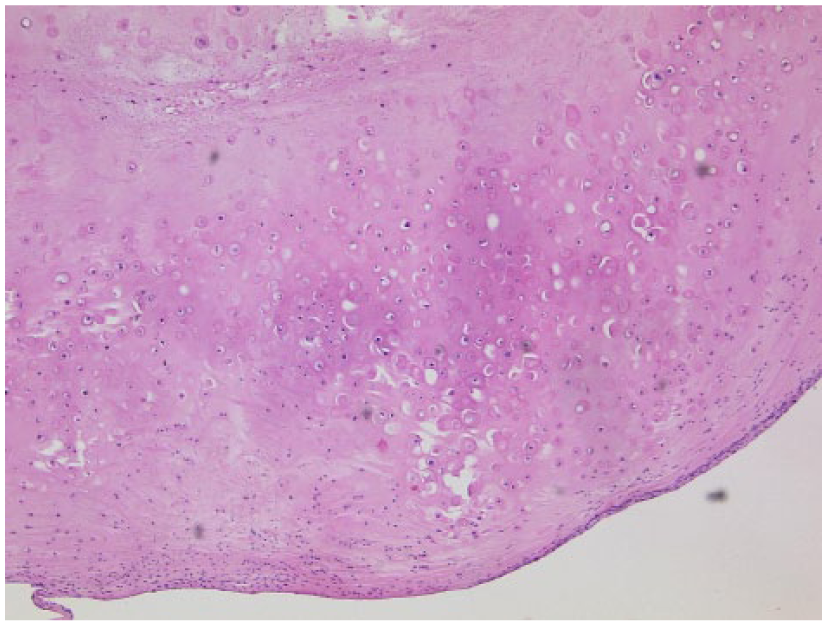
Calcified chondral bodies with regressive changings most likely to correlation to a synovial chondromatosis.
Discussion
The literature about SC has its origin in a first description by Ambroise Pare in 1558, followed by Lannec in 1813. 2 It was reported as a monoarticular, metaplastic change of the synovium with final formation of hyaline cartilage nodules in a joint, in particular the knees (35%) and the elbows (22%). 4
With only 3% of all reported cases, SC is uncommon in the TMJ.3,5 This first discovery of the SC in the TMJ was made by Axhausen 6 in 1933. Since then, only around 200 cases of SC affecting the TMJ were reported in the literature. In general, women are affected more frequently by SC than men.2,7,8
Milgram classified this disease histopathologically into 3 types: (1) a lesion without detached bodies, (2) a lesion with synovial metaplasia and presence of loose bodies, and (3) a lesion with loose bodies and intact synovium. 9
In our case, there was an expanded joint space surrounded by 25 loose calcified bodies. No bony destruction of the condyle, glenoid fossa or temporal bone could be found. According to histological and CT findings, our case could be classified as type 2 of Milgram’s classification.
The usual symptoms of SC include painful preauricular swelling, decreased range of motion and crepitation. Often, it is misdiagnosed as internal derangement of the TMJ because of its low incidence and atypical clinical features. 7
Diagnostics of the SC with an identification of the calcified cartilaginous bodies and bony erosions can be done by CT and MRI. Initial radiographic findings are mostly not visible with panoramic radiography.10,11
The advantage of the MRI is the detection of cartilaginous nodules at an early stage even if they are not calcified. Also the evaluation of the disk, the intra-articular lesion and the extra-articular extension is possible. 12
In our case, the numerous calcified bodies could also be clearly detected in the CT. Nevertheless, CT and MRI do not always lead to a correct diagnosis because of possible minimal calcification of the loose bodies and their low intensity.
There have also been several reported cases in which CT and MRI were not effective in diagnosis but retroscopy was.13,14 Therefore, and to rule out malignant lesions sometimes, positron emission tomography (PET)-CT, gadolinium- or technetium-scintigraphy is recommended in the actual literature. 3
The differential diagnosis of calcified loose bodies found within TMJ includes SC, chondrosarcoma and other benign inflammatory diseases such as osteoarthritis, rheumatoid arthritis and avascular necrosis. 15 SC and synovial chondrosarcoma have many similarities in clinical, radiographic and histological features.
By a description of Bertoni et al. 16 the following histological criteria for the diagnosis of SC in differentiation from synovial chondrosarcoma can be seen: loss of clustering growth pattern, myxoid changes in the matrix, presence of necrosis, hypercellularity and perrmeation of the trabecular bone. In our case there was no histological evidence of necrosis but the chondrocytes showed clustering of the periphery with cellular atypia like enlarged nuclei and binucleated cells and focal increased cellularity (Figure 5).
The final therapy, however, is open arthrotomy according to McCain and De la Rua 17 if loose bodies are larger than 3 mm. Undoubtedly, thoroughly complete removal of the loose bodies provided by the surgeon’s experience is decisive for the final result.
Recurrence is likely if cartilaginous foci or hyperplastic synovium are incompletely removed but unlikely even after sparing extracapsular particles, provided total synectomy and disectomy are performed.3,18 So once diagnosed, removal of loose bodies and the synovium with or without condylectomy is the recommended and accepted treatment to prevent recurrence because the condition does not undergo spontaneous resolution. Malignant transformation of SC to chondrosarcoma has very rarely been reported in the knee joint 19 but may also be possible in the TMJ.
Almost all cases of SC of the TMJ reported monoarticular occurrence. Some authors hold the opinion that SC of the TMJ has a prediction for the right side. Our reported case is in accordance to these descriptions. Nevertheless, this is the focus of discussion. The early stage of SC of the TMJ is manifested not necessarily by abnormality or spreaded calcification of the loose bodies but by smaller processes that are not obvious in CT scans. Therefore, it is understandable why SC of the TMJ so very often presents so-called unilateral prediction. Especially as we know cases with bilateral occurrence. 20
So it seems to be elementary not to overlook checking the contralateral TMJ region and even in case of no abnormality to be found to carry out a long-term follow-up.
Conclusion
The diagnosis to a SC is challenging due to the fact that a large swelling in the preauricular area and the radiographic findings may be misdiagnosed as other benign or malignant diseases and the fact a SC is a rare finding in that area. The open surgical removal of loose bodies and the synovium with or without condylectomy is the recommended and accepted treatment which leads to very low recurrence rates. A malignant transformation to a chondrosarcoma has very rarely been reported in the knee joint but may also be possible in the TMJ.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors disclaim any financial or non-financial interests or commercial associations that might pose or create a conflict of interest with information presented in this manuscript.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.