
Abstract
In recent years, some authors have reported accessory anterolateral talar facet impingement with flatfoot including peroneal spastic flatfoot. Conversely, to our knowledge, no case report has been published about accessory anterolateral talar facet impingement with tibialis spastic varus foot. We report the first case in a 22-year-old man with intellectual disability, bilateral cleft hands and type 1 diabetes mellitus. Since spraining his left ankle over a year earlier, he experienced left sinus tarsi pain while standing and walking. Physical examination revealed that his left foot was in the varus position with spasm of the anterior tibial muscle, tenderness in the sinus tarsi and lateral hindfoot pain upon attempted passive hindfoot eversion. He could not stand on his left toes. His pain decreased after lying down and receiving a massage on his anterolateral lower leg at night. Radiographs and computed tomography scans revealed the absence of tarsal coalition and the presence of accessory anterolateral talar facet in both feet. Magnetic resonance imaging demonstrated abutting bone marrow edema between the talus and calcaneus around the accessory anterolateral talar facet. We diagnosed the patient with accessory anterolateral talar facet impingement and tibialis spastic varus foot. After conservative treatment failed, resection of accessory anterolateral talar facet achieved good results with short-term follow-up.
Introduction
Accessory anterolateral talar facet (AALTF) was first described by Sewell 1 in 1904. AALTF is a small accessory articular surface on the anterior segment of the talar lateral process in continuity with the posterior facet articular surface.1,2 Sewell identified this facet in 10.2% of 1006 Egyptian tali. Sarrafian et al. reported the incidence of AALTF as 34% in 100 cadaver specimens. 2 Although AALTF may be a normal anatomic variant, it can be associated with talo-calcaneal impingement. In 2008, Martus et al. first reported an association between rigid flatfoot and AALTF during adolescence. A search of the PubMed database showed that 53 feet with AALTF impingement including 39 flatfeet have been reported;3–6 however, there is no report of AALTF impingement with tibialis spastic varus foot (TSVF).
Case report
The patient was a 22-year-old man with intellectual disability, bilateral cleft hands and type 1 diabetes mellitus. His body mass index was 26.3 kg/m2. His job consisted of replenishing goods on shelves at a grocery store. Since spraining his left ankle over a year earlier, he experienced left foot pain while standing and walking. He had visited some doctors; however, no diagnosis was made. He was referred to our department in September 2016.
Physical examination revealed that his left foot was in the varus position with spasm of the anterior tibial muscle (Figure 1). Tenderness was located in the sinus tarsi and the pain increased when attempting passive hindfoot eversion. He could not stand on his left toes. His family noted that the pain improved after lying down and receiving a massage on his anterolateral lower leg at night.

Preoperative macroscopic findings: (a) the photograph of the anterior aspect of the feet with the patient in a standing position showed pes cavus of the left foot (black arrows). (b) The photograph of the posterior aspect of the lower legs with the patient in a standing position showed varus deformity of the left heel. (c and d) The longitudinal arch of the left foot was higher than that of the right foot (black arrow). (e) Spasm of the left anterior tibial muscle was observed (black arrowheads).
On the weight-bearing lateral radiographs, Meary’s angle (lateral talo-first metatarsal angle) and calcaneal pitch angle in his left foot were 6.1 degrees and 23.5 degrees, respectively. Those in the right foot were −7.5 degrees and 21.2 degrees, respectively. On the weight-bearing anteroposterior radiographs, talonavicular coverage angle was 29 degrees in the right and 28 degrees in the left. On the hindfoot alignment view, the right calcaneus was 6.1 degrees in valgus and the left was 11.8 degrees in varus. Radiographs and computed tomography (CT) scans revealed the absence of tarsal coalition and the presence of AALTFs in both feet (Figures 2 and 3). Bone sclerosis was observed in the dorsal aspects of both calcaneal necks. Dorsal talar beaking was not observed and the angles of Gissane were not small in both feet. Magnetic resonance imaging (MRI) using short TI-inversion recovery (STIR) sequences demonstrated abutting bone marrow edema between the talus and calcaneus around the AALTF (Figure 4).

Preoperative radiography findings: (a and b) On weight-bearing lateral radiographs, dorsal talar beaking was not observed and the angles of Gissane were not small in both feet. The longitudinal arch of the left foot was higher than that of the right. Bone sclerosis was observed in the dorsal aspects of both calcaneal necks (black arrowheads). (c and d) Weight-bearing posterior-anterior radiographs showed the left calcaneus in varus and the right in valgus.

Preoperative CT image findings: (a and b) three-dimensional CT scans revealed the presence of AALTFs in both feet. Tiny sulci at AALTFs and dorsal aspects of the calcaneus were identified (black arrowheads).

Preoperative MRI findings. Unfortunately, MRI performed at the other hospital did not include a good view of the AALTF. (a and b) MRI on T1-weighted images showed a low signal area indicating bone sclerosis on the radiograph (black arrowheads). (c) MRI using STIR sequences demonstrated abutting bone marrow edema between the talus and calcaneus around the left AALTF (black asterisks).
We diagnosed the patient with AALTF impingement and TSVF. Injection of lidocaine in the sinus tarsi resulted in a temporary resolution of pain and deformity. As his family did not wish to apply a walking cast because they thought he could not tolerate it, a short-leg splint was applied immediately after injection. Two weeks later, his pain decreased significantly and he could stand on his left toes; however, the spasm recurred immediately upon standing without a splint.
Surgical treatment was performed in January 2017. Under general anesthesia, tibial spasm disappeared and we could manipulate the foot in the valgus position. An open resection was performed for AALTF with a 3 cm oblique skin incision along the Langer line. A continuous articular cartilage from the posterior facet of the talus to the AALTF was observed (Figures 5(a) and 6). The anterior aspect of the cartilage was degenerated. Cartilage was also observed on the opposite site of the calcaneal neck. It was thinner than the talar cartilage and also degenerated. After AALTF resection, no talo-calcaneal impingement with eversion of the calcaneus was noted (Figures 5(b) and 7). After surgery, the foot was immobilized in a short-leg splint in the valgus position. Weight-bearing was permitted as tolerated 1 week postoperatively. The splint was removed at that time because the patient could not tolerate it. He went back to work 2 months after surgery. At follow-up 10 months later, the deformity did not recur and there was no pain or spasm.
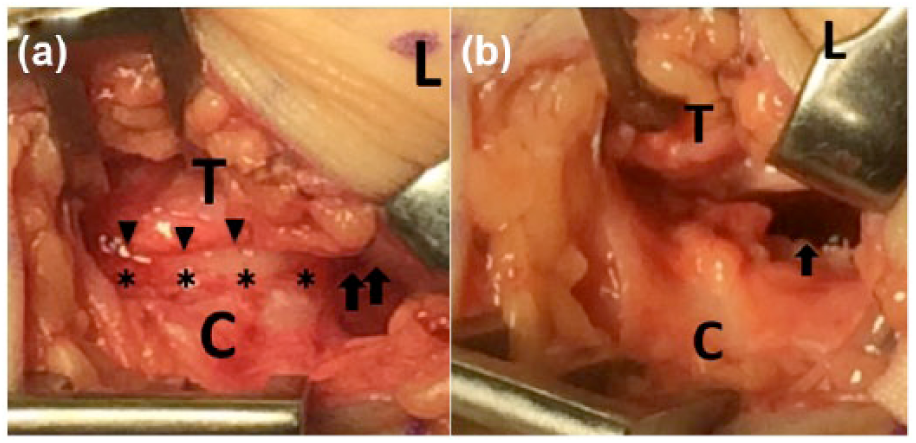
Intraoperative findings: (a) a continuous articular cartilage (black asterisks) from the posterior facet (black arrows) of the talus to AALTF was observed. The superior border of the articular cartilage of AALTF was identified (black arrowheads). (b) After AALTF resection, no talo-calcaneal impingement with eversion of the calcaneus was noted. Black arrow showed the posterior facet (L: lateral malleolus; T: talus; C: calcaneus).

Resected AALTF findings. The views showed medial (a) and plantar aspects (b) of the resected AALTF. A continuous articular cartilage from the talar posterior facet (black asterisks) to AALTF was observed. Black arrowheads showed the anterior boarder of the posterior facet. The anterior aspect of the cartilage of AALTF was degenerated (white asterisks).

Postoperative radiography and CT image findings. Postoperative radiograph (a) and three-dimensional CT scans (b and c) revealed the absence of AALTF postoperatively (black asterisks).
Discussion
We searched the PubMed database on 20 April 2017 for all case reports of AALTF impingement and identified four such clinical reports.3–6 In 53 previously reported feet, 39 flatfeet were included. In all, 46 of 53 feet were treated surgically. In 2008, Martus et al. 3 reported seven pediatric feet of rigid flatfoot with AALTF impingement. All of them were treated surgically. Niki et al. 4 reported 31 adult feet including 18 flatfeet in 2014. They also reported 14 feet with peroneal spastic flatfoot (PSFF) in adolescents in 2015. 5 Seven feet underwent AALTF resection. In 2016, Neumann et al. 6 reported one foot treated with arthroscopic AALTF resection; however, they did not describe the presence of foot deformity in their case. To our knowledge, there is no report of AALTF impingement with TSVF.
Martus et al.3,7 reported that AALTF was associated with male sex and the incidence of bilateral AALTF was 27%. The current patient was also male and had bilateral AALTFs.
Martus et al. believed in two etiologies for talo-calcaneal impingement: a primary impingement caused by the presence of AALTF in a pediatric or young adult rigid flatfoot deformity due to increasing body weight and activity duration, and a secondary impingement due to acquired subtalar joint subluxation seen with advanced acquired adult flatfoot deformity.
Both PSFF and TSVF are considered escape responses to pain, but the exact mechanisms are unclear.8–12 The differences in the etiologies of TSVF and PSFF also remain ambiguous. In fact, with the same diagnosis, for example, in talar coalitions, both PSFF and TSVF cases have been reported.8–12
Martus reported that AALTF was associated with a smaller angle of Gissane and dorsal talar beaking. On the contrary, Hirano et al. 13 found no cases of dorsal talar beaking in adult cadavers. They believed that there is no relationship between dorsal talar beak and the presence of AALTF in adulthood. Hattori et al. 14 measured the talar infero-lateral surface angle rather than the angle of Gissane in adult cadavers and found it was significantly larger in AALTF-positive samples than in negative ones. In the current case, there was neither a smaller angle of Gissane nor dorsal talar beaking, but the facet was large.
MRI demonstrated abutting bone marrow edema between the talus and calcaneus.3–6,15 This was localized to AALTF and the adjacent calcaneus anterior to the posterior facet. CT scans and MRI were useful for diagnosis in the current case.
Hirano et al. 13 classified AALTF into four groups: (1) joint type with articular cartilage on both the talus and calcaneus, (2) talar type with articular cartilage on the talus only, (3) calcaneal type with articular cartilage on the calcaneus only and (4) non-joint type with no articular cartilage on either the talus or calcaneus. The current case was classified as type 1 although there was thinner cartilage on the calcaneal side than on the AALTF.
The histologic evaluation of an excised AALTF in the series reported by Martus et al. 3 was consistent with impingement and consequent early degeneration of the hyaline cartilage of the facet. In the current case, degenerated cartilages were observed in both the facet and the opposite site of the calcaneal neck.
Surgical intervention is offered when pain persists despite non-operative treatment. In patients with contractures, a gastrocnemius recession and/or peroneal lengthening are performed.3,4,14 Remaining planovalgus deformity is corrected with a medial displacement calcaneus osteotomy and/or lateral column lengthening with calcaneocuboid distraction arthrodesis.3,4,14 Niki et al. 5 reported that AALTF resection alone is beneficial for PSFF caused by facet impingement when peroneal spasms are restored by local anesthesia injection. Recurrence of PSFF was not observed in any of their patients who underwent surgery. They also reported that AALTF resection was performed within a thickness of 5 mm, caused no postoperative functional problems and did not affect the adjacent joint. A good result was achieved after resection of AALTF in our case. However, the long-term outcome is unclear after AALTF resection because postoperative follow-up periods were short in all reports.3–6
Conclusion
In conclusion, we report an extremely rare case of AALTF impingement with TSVF. AALTF impingement should be considered for patients with not only PSFF but also TSVF. Surgical resection of AALTF achieved a good result with short-term follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed consent was obtained from the patient and his family.