
Abstract
The third-generation thienopyridine prasugrel has much stronger antiplatelet effect compared to other current antiplatelet inhibitors and exhibits practically zero resistance in healthy people. Prasugrel is used as a pre- and post-treatment in percutaneous coronary or neurovascular interventions with parallel aspirin regime. However, as there is a higher reported bleeding with intraluminal interventions and meticulous technique is recommended, there is nearly non-existent international experience of open surgery under full prasugrel treatment. We present, herein, a case of open carotid endarterectomy with the eversion technique in an asymptomatic patient with carotid stenosis, who was receiving dual antiplatelet therapy with aspirin and prasugrel, due to a previous insertion of two newer drug-eluting stents at the left anterior descending artery and the right coronary artery. The resistance test to prasugrel showed complete inhibition of platelet function. Open surgery was performed under continuation of prasugrel treatment and interruption of aspirin for 3 days before surgery. No perioperative and postoperative neurologic or cardiologic event occurred. No bleeding at the cervical or cerebral area was noted.
Introduction
Patients with occlusive arterial disease, especially those experiencing acute coronary syndrome, require a potent and effective antiplatelet treatment; particularly, when a percutaneous coronary intervention (PCI)—balloon angioplasty and stenting—is anticipated, pre- and post-procedural antiaggregant treatment is the cornerstone of endo-revascularization strategy. 1 Prasugrel is a potent, rapid, and constant inhibitor of the P2Y12 chemoreceptor for adenosine diphosphate (ADP), which inhibits strongly ADP-induced platelet aggregation and exhibits nearly zero resistance in healthy individuals.2–4
Prasugrel is a potent antiplatelet agent and particularly is 10 times more potent than clopidogrel and not just “strong.” 5 Thus, prasugrel is preferred more than clopidogrel as the one component of the dual antiplatelet regimen, which is usually given in patients following coronary or neurovascular interventions; the other component is aspirin. 6 The much stronger antiaggregant potential of prasugrel is accompanied by an increased risk of hemorrhage, 7 and due to special characteristics of prasugrel and the high risk for severe hemorrhagic consequences, there is no international experience concerning open surgery under prasugrel treatment. The only experience about prasugrel comes mainly from cardiologic interventions and complications from sites of insertion of catheters, with increased bleeding. 8 The up to now international experience on bleeding is accumulated from the endoluminal interventions and has often been noticed at anatomic areas of catheter insertions (e.g. groin area). Cardiologists now prefer the treatment of their patients with prasugrel, and there is plenty of literature about the guidelines of American College of Cardiology/American Heart Association concerning prasugrel and PCIs. The obvious advantages are as follows: much potent antiplatelet activity, much quicker onset of action, more consistent patient response, and lack of drug interaction.9–12
As there is no worldwide experience with open surgery under full prasugrel treatment, we present, herein, a case of a patient who was under dual antiplatelet regimen, due to previous coronary stenting, and he underwent an eversion endarterectomy for a high degree asymptomatic carotid stenosis.
Report of the case
A 65-year-old woman presented for surgical treatment of an asymptomatic right internal carotid artery stenosis up to 85%. The patient had undergone insertion of two drug-eluting stents—Everolimus Eluting Platinum Chromium Coronary Stent System—(DES second-generation) PROMUS PREMIER (Boston Scientific) into the left anterior descending artery and the right coronary artery, because of unstable angina, 6 months ago. Following stenting, she was under dual antiplatelet therapy with aspirin 100 mg and prasugrel 10 mg, once daily. The test of the patient’s resistance to prasugrel showed complete inhibition of platelet function (Figure 1) and no aspirin’s resistance. A magnetic resonance imaging (MRI) of the brain was performed without pathological findings. To perform surgery, aspirin was stopped for 3 days without any interruption of prasugrel treatment.
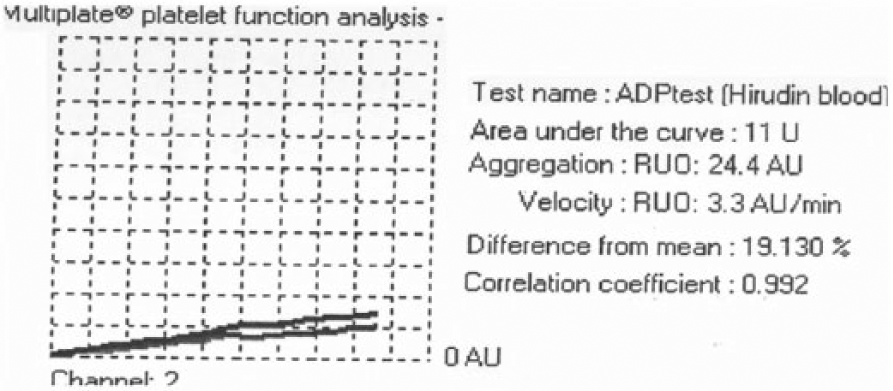
The test of the patient’s resistance to prasugrel showed complete inhibition of platelet function.
Under general anesthesia, a lateral cervical incision was performed, and the right common, external and internal carotids were prepared. After intravenous administration of heparin 5000 UI, eversion endarterectomy followed and the anastomosis was performed with polypropylene 6.0 suture. The aspirin was given to the patient 2 h after the surgery while she continued treatment with prasugrel. The patient followed a smooth postoperative course, without any neurological or cardiological event, cervical, cerebral, or other bleeding or thrombosis, and was discharged on the second postoperative day. The histopathology exam of the atheroma, length of 3.2 cm, removed from the right internal carotid artery showed atherosclerotic lesions.
Discussion
Patients with the systemic disease of atherosclerosis already have different levels of inflammation resulting in platelet activation. Additionally, when an acute vascular syndrome takes place by a disrupted fibrous cap from a vulnerable plaque, immediate—if possible—vessel remodeling is needed along with major antigreggant medication, which leads to better ischemic outcome.6,13 Thus, the mainstay of acute coronary syndromes management involves medications that strongly inhibit platelet activation. Dual antiplatelet regimens have been elaborated in pre- and post-coronary balloon angioplasty and stenting. The initial dual component therapy included aspirin and clopidogrel. 8 Newer inhibitors to P2Y12, a protein observed mainly on the surface of blood platelets which is a receptor for ADP, overcome the observed resistance up to 30% of patients to clopidogrel and show much more potent antiaggreggant function. 7 Prasugrel is a third-generation thienopyridine inhibiting the P2Y12 chemoreceptor and along with aspirin exert more potent effects on the activity of the platelets, by reducing thrombotic episodes.2,13 The experiments of Niitsu et al. 14 show that prasugrel exerts stronger inhibitory activity of platelets by 10 and 300 times, compared with clopidogrel and ticlopidine, respectively; as a result, the time for arterial occlusion and the duration of arterial patency are increasing. Moreover, prasugrel is considered especially effective when administered in combination with aspirin in patients with acute coronary syndrome, undergoing pecutaneous coronary nterventions (PCIs). However, an increased chance of bleeding has been observed, and unfortunately, there is no clinical evidence that small doses of prasugrel for maintenance, to avoid bleeding, is sufficient to adequately suspend the platelets. 15
The percutaneous transluminal coronary angioplasty (PTCA) is associated with acute occlusion and restenosis of the affected vessel, and to avoid complications, intracoronary stents (ICS) are used, resulting in reduced risk of thrombosis. So, the American College of Cardiologists (ACC) proposes the granting of dual antiplatelet therapy for 14 days after balloon angioplasty, 30 days for bare metal stent (BMS), and 365 days after drug-eluting stent (DES). 16 DESs, used mainly for the reduction of restenosis events and to promote revascularization, in order to prevent stent thrombosis, require dual antiplatelet therapy. The second-generation stents DES, the endeavor zotarolimus-eluting stent (E-ZES), and the Xience-V everolimus-eluting stent (EES) cause intimal coverage in 3–4 months with less likelihood of thrombus development.17,18 The patient, we have managed, had two second-generation stents into the left anterior descending artery and the right coronary artery due to previous unstable angina. Although she was asymptomatic, the degree of the carotid stenosis was high, and she was very anxious about her disease. In case of elective surgery, the operation should be postponed in patients with coronary stent(s), until the recommended time with dual antiplatelet therapy is completed. Surgery can be performed within 12 months, following intervention for old generation DES and within 6 months for newer generation DES. 19 When the bleeding risk is not high, the continuation of dual antiplatelet therapy or discontinuation of one antiplatelet drug in the perioperative period have both been proposed. However, this recommendation comes from observations following therapy with aspirin/clopidogrel combination. With the aspirin/prasugrel regimen, there is no world experience in relation to continuation of both antiplatelets in open surgery. In particular, with continuation of prasugrel, high bleeding rate is anticipated. Thus, it is important, prior to surgery, that an interdisciplinary consultation to be done among the cardiologist, anesthesiologist, and the surgeon for the patient management, due to the substitution difficulty of thienopyridines. 16 Current guidelines (Class IIa recommendation) in asymptomatic patients do not forbid endarterectomy of carotid stenosis > 70%–99% and patient’s age < 70 years, with a good life expectancy,20,21 while in symptomatic patients with carotid stenosis, prasugrel has to be avoided thus the discussion with the patient was based in the probability of a future cerebrovascular event during prasugrel treatment and the accompanied possible brain bleeding risk.
In the case we present, the patient showed no resistance to prasugrel, so we decided to continue prasugrel regimen and to interrupt aspirin for only 3 days before surgery, to protect the stents, and to reduce the risk of bleeding. The decision for the treatment was tailored for the patient based on consensus among the cardiologist, anesthesiologist, surgeon, and the patient. There was no perioperative coronary event and an open eversion endarterectomy took place. We observed no unusually higher tendency to bleed at the area during the neck dissection. We have chosen to perform an eversion endarterectomy based on the color Doppler ultrasound of carotids and vertebral arteries (Figure 2) and the angiographic image of digital subtraction head and neck angiography (DSA) (Figures 3–5), in order to avoid using a synthetic patch (higher bleeding risk of the suture line), in case of narrowing if a usual longitudinal endarterectomy and closure would be performed in a woman’s carotid. Before the dermal closure we always put a negative pressure closed suction which we remove the first postoperative day. The patient left hospital on the second postoperative day with no neck hematoma or any other bleeding.

The color Doppler ultrasound of carotids and vertebral arteries showed atherosclerotic plaque, which causes stenosis of right internal carotid artery up to 70% with peak systolic velocity up to 338 cm/s.

The digital subtraction head and neck angiography (DSA) of right common carotid artery showed kinking and marked stenosis of the right internal carotid artery.

Selective angiography of right common carotid artery.

Selective angiography of left common carotid artery showed greater blood flow than right common carotid artery.
As the only reported experience with prasugrel treatment comes from percutaneous interventions 22 , 23 , there is no world experience with open surgery. We think that this report might be useful in order to encourage open surgery—at least no abdominal—in patients under full prasugrel medication, although the discontinuation of aspirin for only 3 days was not formal. As many patients with systemic manifestations of the same disease—atherosclerosis—suffer from coronary disease and need prasugrel, and may need a carotid endarterectomy, we propose eversion endarterectomy (Figure 6) under full prasugrel treatment.

Eversion endarterectomy under full prasugrel treatment, posterior wall anastomosis.
Conclusion
Given the lack of evidence-based guidelines for the management of dual antiplatelet therapy involving prasugrel in patients with coronary stents, who have to undergo open surgery, 15 we present, herein, the case of a woman, who had an eversion endarterectomy under complete treatment with prasugrel, without complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.