
Abstract
Immunoglobulin G4-related disease characteristically involves multiple organs including the heart and coronary arteries. Immunoglobulin G4-related coronary artery disease is thought to be due to periarteritis and histopathologically is characterized by marked thickening of the adventitia and periarterial fat with infiltration of immunoglobulin G4-positive plasma cells. Although comprehensive diagnostic criteria require a biopsy for a definite or probable diagnosis of immunoglobulin G4-related disease, obtaining a coronary artery biopsy is difficult and risky. However, imaging findings including coronary angiography and intravascular ultrasound might be useful tools to establish a diagnosis of immunoglobulin G4-related coronary artery disease. We report a case of a 63-year-old man with a history of immunoglobulin G4-related disease who presented with exertional chest pain. We found unique angiographic and intravascular ultrasound features of immunoglobulin G4-related coronary artery disease that distinguished it from those of arteriosclerotic coronary artery disease and suggest that coronary angiography and intravascular ultrasound might be useful tools in the diagnosis of immunoglobulin G4-related coronary artery disease.
Keywords
Introduction
Immunoglobulin G4-related disease (IgG4-RD) is a systematic condition characterized by IgG4-positive (IgG4+) plasma cell infiltration in an affected organ and an elevated serum IgG4 concentration. 1 The concept of this disease was established through the extensive evaluation of extrapancreatic lesions in patients with autoimmune pancreatitis (AIP). 1 IgG4-RD characteristically involves multiple organs and has been formerly diagnosed as AIP, Mikulicz’s disease, fibrosing mediastinitis, hypertrophic pachymeningitis, Riedel’s thyroiditis, tubulointerstitial nephritis, prostatitis, and retroperitoneal fibrosis.
Recently, IgG4-related immune-inflammation has been shown to affect the cardiovascular system, 2 with reports of inflammatory abdominal aortic aneurysms (IAAAs), periaortitis, and periarteritis. Other investigators have reported involvement of the coronary arteries.3 –5 The reported clinical features of IgG4-related coronary artery disease (CAD) include inflammatory pseudotumor, periarterial fibrosclerotic thickening, coronary artery aneurysm, and coronary artery stenosis.2,6 IgG4-related CAD is thought to be due to periarteritis and histopathologically demonstrates marked thickening of the adventitia and periarterial fat with infiltration of IgG4+ plasma cells. 7
Although the comprehensive diagnostic criteria, proposed by research groups organized by Japan’s Ministry of Health, Labor, and Welfare, 8 require a biopsy for a definite or probable diagnosis of IgG4-RD, obtaining a coronary artery biopsy is difficult and risky. Therefore, imaging findings including coronary angiography (CAG) and intravascular ultrasound (IVUS) might be useful tools to assist in establishing a diagnosis of IgG4-related CAD. There have been several previous reports describing the findings of coronary computed tomography angiography (CCTA) and positron emission tomography (PET) in patients with IgG4-related CAD,2,9 but none describing CAG and IVUS findings in these patients.
We report a case of a 63-year-old man with a history of IgG4-RD who presented with exertional chest pain. We found significant differences in the angiographic features of his coronary artery lesions in comparison with those seen in patients with arteriosclerotic CAD.
Case report
A 63-year-old man (height: 176 cm, weight: 69 kg) presented to a nearby hospital complaining of exertional chest pain. He had experienced similar pain a month earlier, 2 h after his evening meal. Blood examination, chest radiography, electrocardiogram (ECG), and computed tomography (CT) showed no specific abnormalities, and he was referred to our hospital for further evaluation. A 12-lead ECG at our facility showed T-wave inversion in leads V1 through V3. Transthoracic echocardiography showed severe hypokinesis from the antero-septal wall to the mid-apex. He was admitted to our hospital to undergo CAG for suspected myocardial ischemia. The patient had a history of hypertension, chronic kidney disease, sudden deafness, and smoking. He had no history of dyslipidemia, diabetes mellitus, or alcohol consumption, and there was no history of ischemic heart disease in his family. Although he was diagnosed with IgG4-RD 1 year prior, he had not received any treatment for that condition. At that time, pathological examination of a submaxillary gland showed an infiltration of small lymphocytes, acidophilic leukocytes (acidocytes), and plasma cells, particularly IgG4+ plasma cells. The IgG4+/IgG+ plasma cell ratio was >40%. Four months previously, he had also been diagnosed with IgG4-related nephritis on the basis of a renal biopsy.
His physical examination showed a blood pressure of 138/74 mmHg, a pulse of 48 beats per minute, a respiratory rate of 12 breaths per minute, and an oxygen saturation of 96% on room air. No cardiac murmurs or abnormal respiratory sounds in the lungs were detected with auscultation. Blood examination revealed elevated levels of creatinine (1.12 mg/dL; normal: 0.65–1.09 mg/dL), triglycerides (163 mg/dL; normal: 35–150 mg/dL), and brain natriuretic peptide (53.4 pg/mL; normal: 0.0–18.4 pg/mL), and a normal level of β2 (1.9 mg/dL; normal: 0.8–2.0 mg/dL). Immunological examination showed elevated levels of IgG (1896 mg/dL; normal: 739–1649 mg/dL), IgG4 (527 mg/dL; normal: 4–108 mg/dL), and soluble interleukin-2 receptor (sIL-2R; 751 U/mL; normal: 220–530 U/mL) and low levels of C3 (82 mg/dL; normal: 86–160 mg/dL) and IgM (29 mg/dL; normal: 46–260 mg/dL).
CAG showed a 90% stenosis in the mid-left anterior descending (LAD) coronary artery (Figure 1). The stenosis looked smoother than those seen in arteriosclerotic stenosis. No other lesions were detected. After a guide wire crossed the lesion, IVUS (View It; Terumo, Tokyo, Japan) catheter was inserted to visualize the characteristics of the LAD lesions. IVUS demonstrated a thickened black layer beneath the intima at the lesion and nearly normal vessel wall at the proximal and distal LAD (Figure 2). Compared to proximal and distal arteries, stenosis of the lesion consisted of thickened intima-media, especially black layer beneath the intima. The LAD lesion was treated with percutaneous coronary intervention (PCI) using a drug-eluting stent. PCI was successful with no complications, and the patient’s exertional chest pain resolved after treatment. Two months later, the patient was started on corticosteroid therapy for the treatment of sudden deafness. Follow-up CAG at 1 and 3 years later showed no de-novo lesions and no in-stent restenosis.
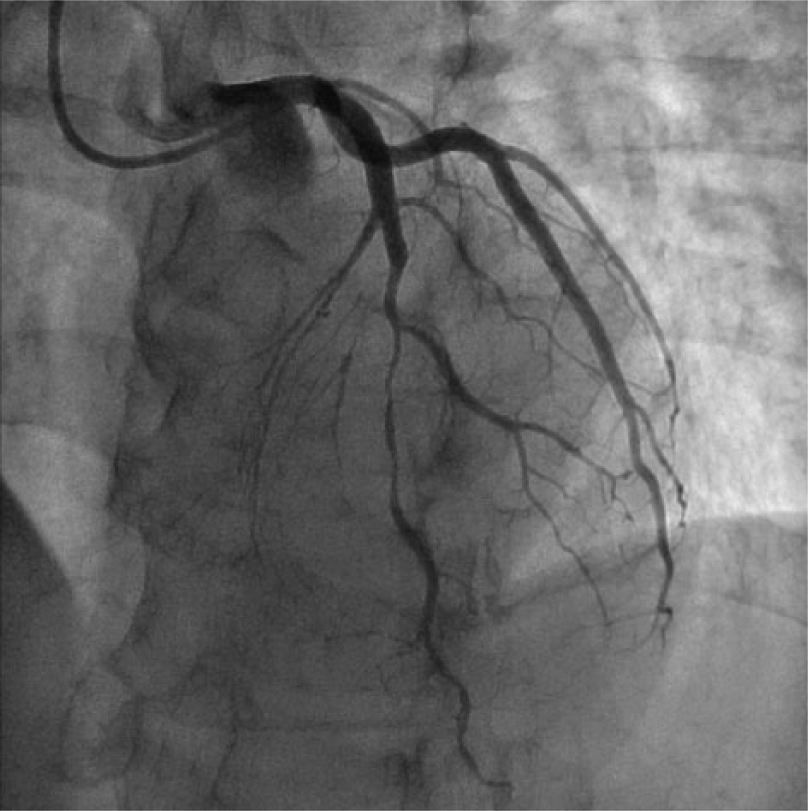
Coronary angiography (CAG) findings. CAG showed 90% stenosis in the mid-left anterior descending (LAD) coronary artery. The stenosis looked smoother than typical arteriosclerotic stenosis. No other lesions were detected.

Intravascular ultrasound (IVUS) findings: (a, c) IVUS finding of normal coronary artery in our patient’s proximal and distal left anterior descending (LAD) arteries, (b) IVUS findings of our patient’s LAD lesion demonstrating a thicken black layer beneath the intima (arrowheads) and external elastic membrane which is the outside edge of the medial (arrow).
Discussion
We described the significant feature of angiographic and IVUS findings, compared to histopathological features. This is the first report describing the findings in an IgG4-related coronary artery stenosis detected not only by CAG but also by IVUS. In the present case, we noted that the CAG revealed a remarkably smoother stenosis than what is seen in a typical arteriosclerotic stenosis. Prior histopathological studies have demonstrated that patients with IgG4-related CAD have periarterial fibrosclerotic thickening, with marked thickening of the adventitia and media. 7 Coronary artery stenosis in these patients might be the result of narrowing of the lumen by the periarterial fibrosclerotic thickening or by the marked thickening of the adventitia and media directly. In the present case, IVUS showed marked thickening of black layer between intima and external elastic membrane, which was considered as hyaline fibrosis in histopathological studies.
IgG4-related immune-inflammation has been shown to affect the cardiovascular system, 2 and reports have demonstrated IAAAs, periaortitis, and periarteritis. IgG4-related IAAAs have been reported in the thoracic aorta (4 cases), abdominal aorta (11 cases), and abdominal aorta to iliac arteries (13 cases).2 –4 IgG4-related pathology has also been observed in the pulmonary artery (1 case), celiac artery, superior mesenteric artery (2 cases), renal artery (3 cases), inferior mesenteric artery (6 cases), splenic artery (1 case), subclavian artery, and iliac artery (5 cases).3 –5 A total of 18 patients have been reported with IgG4-related coronary artery involvement.2 –5 Eight of these patients experienced myocardial ischemia, one case had a myocardial infarction, and five cases experienced sudden death due to IgG4.5,6,10
According to the comprehensive diagnostic criteria, 8 we reached a definite diagnosis of IgG4-RD in the present case based on the elevated serum IgG4 concentration and the infiltration of IgG4+ plasma cells into the submaxillary gland and renal tissues on previous biopsies. However, we could establish a diagnosis of either definite or probable IgG4-related CAD, because obtaining a biopsy from a coronary artery was felt to be difficult and risky. Histological characteristics are required for a definitive or probable diagnosis of IgG4-RD, based on the comprehensive diagnostic criteria for IgG4-RD; 8 a diagnosis cannot be established without histological findings. Because several cases of sudden death due to IgG4-related CAD have been reported in the literature, we should consider the adoption of organ-specific diagnostic criteria that do not require tissue sampling.6,10 CAG and IVUS might be useful tools to aid in establishing a diagnosis of IgG4-related CAD.
Conclusion
We report unique angiographic features of IgG4-related CAD that were different from those seen with arteriosclerotic CAD. Several cases of sudden death due to IgG4-related CAD have been reported in the literature, and patients with a smooth stenosis in CAG should be evaluated for the possibility of IgG-RD. CAG and IVUS may be useful tools for establishing a diagnosis of IgG4-related CAD.
Limitation
We had no data of biopsy, and ECG-gated CT and Fluoro-deoxyglucose (FDG)-PET. Therefore, we could not diagnose these patients as IgG4-related CAD.
Footnotes
Acknowledgements
These data have already been presented at the 80th Japanese Circulation Society. Yusuke Kanzaki and Takashi Miura involved in drafting the manuscript. Koichiro Kuwahara involved in revising it critically. Naoto Hashizume, Tatsuya Saigusa, and Soichiro Ebisawa contributed to acquisition of data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.