
Abstract
Background:
Patient prognosis has been shown to directly correlate with the severity of coronary artery disease diagnosed by coronary computed tomography angiography (CCTA). Although the presence of coronary artery calcium has been associated with increased incidence of ischemic stroke, there are no data on the incidence of ischemic stroke based upon the severity of coronary artery disease by CCTA. Therefore, we sought to investigate the rate of major adverse cardiovascular events, including ischemic stroke, based upon the severity of coronary artery disease by CCTA over a 6-year period in a high-volume single military center.
Methods:
We performed a retrospective chart review of all CCTA studies to evaluate the incidence of all-cause mortality, non-fatal myocardial infarction, ischemic stroke, and late revascularization (>90 days following CCTA) from January 2005 until July 2012. We reviewed 1518 CCTA reports, dividing patients into groups with obstructive (≥50% stenosis), non-obstructive (<50% stenosis), and no coronary artery disease (no angiographic disease). Subsequent major adverse cardiovascular events data (incidence of all-cause mortality, ischemic stroke, non-fatal myocardial infarction, and late revascularization) were obtained.
Results:
Over a review period of 6 years with a resultant median follow-up period of 22 months (interquartile range = 13–34 months), the major adverse cardiovascular events rate was significantly higher with obstructive coronary artery disease compared to both non-obstructive coronary artery disease and no coronary artery disease (8.9% vs 0.7%, p < 0.001; 8.9% vs 1.6%, p < 0.001). The incidence of ischemic stroke alone was also significantly higher in those with obstructive coronary artery disease compared to those with no coronary artery disease (3.8% vs 0.4%, p < 0.001).
Conclusion:
Being free of disease on CCTA was associated with excellent cardiovascular prognosis. Obstructive coronary artery disease was associated with a significantly increased incidence of ischemic stroke. There was also a direct correlation between the severity of coronary artery disease on CCTA and cardiovascular prognosis over the follow-up period of 24 months.
Keywords
Introduction
The rapid growth of coronary computed tomography angiography (CCTA) technology in the past decade has led to improved resolution of epicardial coronary vasculature and, thus, the more accurate detection of obstructive coronary artery disease with high sensitivity (>90%) and specificity (>90%). 1 A meta-analysis in 2011 by Hulten et al. 2 showed a higher major adverse cardiovascular events (MACE) rate with obstructive disease versus no disease. This was replicated by another meta-analysis by Bamberg et al., 3 demonstrating that obstructive coronary artery disease (CAD) was an independent predictor of future MACE. Similar results were also published by the CONFIRM registry group, in their 24,000-patient population. 4 In each of these studies, the absence of disease is associated with a very favorable prognosis.
Atherosclerosis is a generalized process and ischemic stroke and CAD share many of the same risk factors. A close association between coronary artery calcification and extra-coronary plaque burden has been reported. 5 Additionally, a graded association between coronary calcification by electron-beam computed tomography and the incidence of ischemic stroke was previously described. 6 Prior CCTA studies have evaluated all-cause mortality, non-fatal myocardial infarction (MI), and late revascularization only. 7 There are no data on the incidence of ischemic stroke based upon an individual’s burden of coronary atherosclerosis.
Therefore, we attempted to evaluate the rate of MACE, including ischemic stroke, based upon the severity of CAD in a single military center with high-volume CCTA over a span of 6 years with reliable follow-up based on Department of Defense electronic healthcare repository in conjunction with the social security death index (SSDI).
Methods
Patient selection
We performed a retrospective chart review of symptomatic adults at least 18 years of age who underwent 16-, 64-, or 128-slice CCTA between January 2005 through July 2012 at a single-center, tertiary referral hospital (San Antonio Military Medical Center, Joint Base San Antonio-Fort Sam Houston, TX, USA). The indication for the study for the great majority of our cohort was a chest pain syndrome, although there were a small minority that underwent the study for dyspnea as part of a “triple rule-out” protocol, or evaluation for anomalous coronary anatomy as part of a syncope evaluation. We included patients with known coronary artery disease who underwent CCTA for graft patency (compromised a small subset of the study). Exclusion criteria included studies uninterpretable due to motion artifact and coronary artery calcium (CAC) scores > 1000, if it affected the scan interpretation. Patients at risk of stroke requiring evaluation for neurovascular events were excluded to include CCTA performed for pulmonary vein isolation (PVI) mapping for atrial fibrillation. Any segment that was deemed uninterpretable by the first reader was adjudicated by a level III imaging cardiologist (senior author). If the segment was unable to be read, then the study was deemed uninterpretable to decrease bias in results. Patients with history of MI or ischemic stroke were excluded as well. Institutional review board approval was obtained.
Noninvasive coronary artery analysis by CCTA
All scans were analyzed by a cardiologist with level III Society of Cardiovascular Computed Tomography (SCCT) experience. From January 2005 through December 2007, images were obtained using a 16-slice CT scanner (Brilliance-16®, Phillips, Amsterdam, The Netherlands). Scans were performed in accordance with SCCT guidelines. 8 From January 2008 to March 2011, images were obtained using a retrospective helical protocol with a 64-slice CT scanner (Somatom Definition CT®, Siemens, Erlagen, Germany). From March 2011 to March 2012, studies were obtained utilizing a prospective sequential protocol with 60%–80% image acquisition window. In March 2012, 128-slice dual head scanner with a single heart beat image acquisition of the complete coronary when a heart rate of less than 60 was achieved (Somatom Definition Flash CT®, Siemens, Erlagen, Germany).
CCTA stenosis severity assessment
Initial analysis was performed by a level II imaging cardiologist and adjudicated by a level III imaging cardiologist as per method, where the severity of the disease was determined on a per-patient and per-vessel basis using the SCCT 18-segment model in accordance with SCCT guidelines for interpretation. 9 The major epicardial coronary arteries (left main, left anterior descending, left circumflex, and right coronary arteries) were visually graded for evidence of coronary calcification and presence and severity of coronary atherosclerosis. The posterior descending artery was included in the left circumflex or right coronary artery groups depending on its origin. We categorized these patients based upon the severity of CAD, defined as obstructive CAD (>50% stenosis), non-obstructive CAD (<50% stenosis), or no CAD (vessels free of angiographic evidence of disease), respectively.
Follow-up
The primary endpoint was composite MACE, defined as all-cause mortality, ischemic stroke, non-fatal MI, and late revascularization (defined as revascularization performed at least 90 days after CCTA). We also compared the incidence of each MACE outcome individually based upon the severity of CAD. International Statistical Classification of Diseases and Related Health Problems (ICD)-9 codes for all-cause mortality (798.1, 798.2, 798.9, and V12.53), ischemic stroke (434.00, 434.01, 434.10, 434.11, 434.90, 434.91, 997.02, and V12.54), non-fatal MI (410.0–410.9), and late revascularization with percutaneous coronary intervention (PCI) (92980, 92981, 92982, 92995, and 92996) or coronary artery bypass grafting (CABG) (33510-33514, 33516, and 33533-33536) were used for initial data extraction followed by Department of Defense outpatient and inpatient electronic medical records (EMRs) verification of events. We determined mortality using the SSDI followed by re-verification using EMRs for last visit date as well as Tricare healthcare informatics division verification. All events identified by ICD-9 code were adjudicated and events were confirmed in subject’s EMRs.
Statistical analysis
Statistical analysis was performed using IBM SPSS version 19.0 (IBM, Arnock, New York). Continuous variables are presented as means ± standard deviation and medians with interquartile range (IQR), as appropriate. All continuous variables were assessed for normality prior to hypothesis testing in SPSS. Cox proportional hazard models were developed to assess for variables associated with clinical outcomes. Univariable predictors with a significance level p < 0.10 were evaluated for inclusion in the final Cox model. Categorical variables are presented as frequencies with percentages. Comparison of means was performed using one-way analysis of variance (ANOVA) with post hoc Bonferroni correction, with p-values < 0.05 considered significant. Event-free survival was assessed by the Kaplan–Meier method and the log-rank test used to analyze the difference in mean survival times. Hazard ratios (HRs) for variables associated with MACE by risk factors for CAD and obstructive CAD were computed and compared by Cox proportional hazards models.
Results
Clinical and CCTA characteristics of the study cohort
After reviewing 1757 CCTA studies, 239 did not meet the inclusion or exclusion criteria either due to image limitation or being used for PVI planning prior to atrial fibrillation. Of the 1518 subjects with interpretable studies, only nine patients were examined on the 16-slice scanner, the average age was 53 ± 14 years with 60.5% male predominance and no loss to follow-up in EMRs. The mean age increased as the severity of CAD increased, with a statistically significant difference between obstructive CAD and no CAD (61 ± 11 vs 47 ± 14; p < 0.001). Overall, hypertension was present in 36.9% of the patients and hyperlipidemia was present in 30.8%. The proportion of patients with diabetes mellitus type 2 was low (4.1%). There was a statistically significant difference in the percentage of patients with diabetes, hypertension, and hyperlipidemia among those with obstructive CAD compared to those with no CAD (Table 1). The majority of patients had either non-obstructive or no CAD (Figure 1).
Baseline characteristics based upon severity of CAD by CCTA.

CAD: coronary artery disease; CCTA: coronary computed tomography angiography; CABG: coronary artery bypass grafting.
Values are % (n) or mean ± standard deviation. Severity of CAD was classified as obstructive (>50% stenosis), non-obstructive (<50% stenosis), and no CAD (no angiographic disease).
p-value < 0.05 considered significant.

Breakdown of the severity of CAD by CCTA per coronary vessel
CCTA characteristics associated with MACE
Over a mean follow-up period of 24 months (median of 22 months and IQR of 13–34 months), there was a statistically significant difference in MACE between obstructive and no CAD (8.9% vs 0.7%, p < 0.001) as well as between obstructive and non-obstructive CAD (8.9% vs 1.6%, p < 0.001) (Figure 2). Between non-obstructive and no CAD, there was no significant difference in MACE (1.6% vs 0.7%, p = 1.000) (Table 2). There was a significant difference in the mean survival from MACE between obstructive and no CAD, with those without CAD with longer mean survival times (1572 ± 62 days, 95% confidence interval (CI): 1450–1693 vs 1977 ± 17 days, 95% CI: 1944–2012; p < 0.001) (Figure 3). There was no significant difference in mean survival time between non-obstructive and no CAD (Table 3). The difference in mean MACE-free survival time was also seen on a per-vessel basis (Figure 4). The mean MACE-free survival was significantly longer when no CAD was compared to one-, two-, and three-vessel obstructive CAD (Table 4). Univariable risk factors associated with MACE were age (HR = 1.067, 95% CI: 1.037–1.097; p < 0.001), hypertension (HR = 2.135, 95% CI: 1.085–4.203; p = 0.028), and obstructive CAD on CCTA (HR = 7.084, 95% CI: 2.969–16.905; p < 0.001) (Table 5). Cox proportional hazards multivariable regression analysis demonstrated that age (HR = 1.055, 95% CI: 1.021–1.091; p = 0.001) and obstructive CAD by CCTA (HR = 3.742, 95% CI: 1.396–10.030; p = 0.009) were independent risk factors associated with MACE (Table 6).

Overall incidence of MACE (all-cause mortality, ischemic stroke, non-fatal MI, and late revascularization) and isolated cardiovascular outcomes according to CAD severity by CCTA.
Annualized incidence of composite MACE and isolated endpoints of all-cause mortality, ischemic stroke, non-fatal MI, and late revascularization based upon severity of CAD.
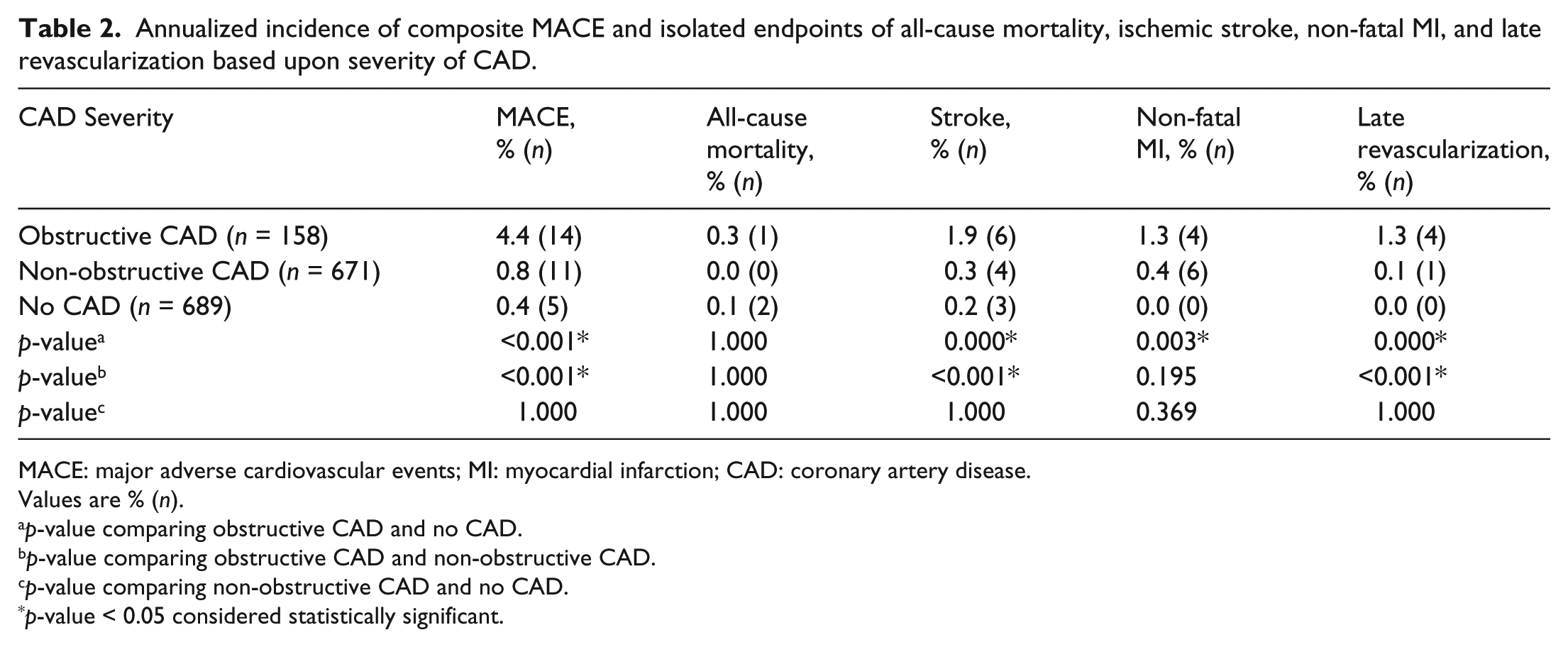
MACE: major adverse cardiovascular events; MI: myocardial infarction; CAD: coronary artery disease.
Values are % (n).
p-value comparing obstructive CAD and no CAD.
p-value comparing obstructive CAD and non-obstructive CAD.
p-value comparing non-obstructive CAD and no CAD.
p-value < 0.05 considered statistically significant.

Kaplan–Meier curves comparing event-free survival from composite MACE stratified by severity of CAD.
Per-patient mean survival times with Mantel–Cox p-values comparing mean survival time from MACE between obstructive and non-obstructive with no CAD.

MACE: major adverse cardiovascular events; CAD: coronary artery disease; SE: standard error; LCI: lower confidence interval; UCI: upper confidence interval.
p-values use no CAD as the reference comparator.

Kaplan–Meier curves comparing event-free survival from composite MACE between one-, two- and three-vessel obstructive, non-obstructive, and no CAD.
Per-vessel mean survival times with Mantel–Cox p-values comparing mean survival from MACE between one-, two-, three-vessel obstructive, and non-obstructive CAD with no CAD.

MACE: major adverse cardiovascular events; CAD: coronary artery disease; SE: standard error; LCI: lower confidence interval; UCI: upper confidence interval.
p-values use no CAD as the reference comparator.
Univariate regression analysis using Cox proportional hazard model for prediction of composite MACE.

MACE: major adverse cardiovascular events; CAD: coronary artery disease; HR: hazard ratio; SE: standard error; LCI: lower confidence interval; UCI: upper confidence interval.
p < 0.05 considered statistically significant.
Cox proportional hazards regression analysis for prediction of composite MACE.
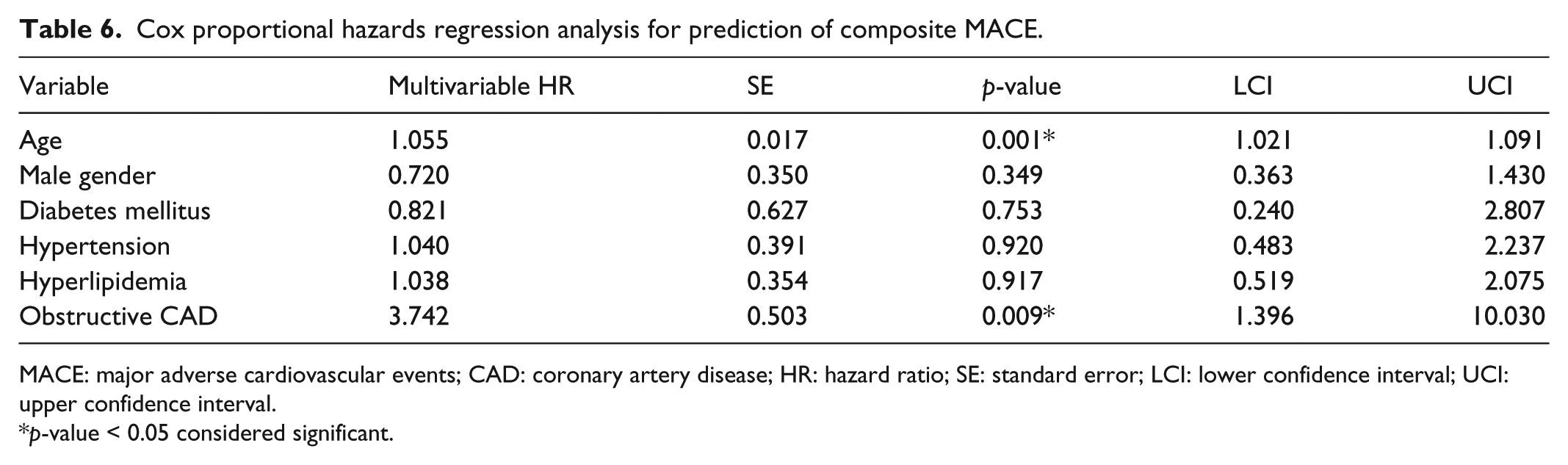
MACE: major adverse cardiovascular events; CAD: coronary artery disease; HR: hazard ratio; SE: standard error; LCI: lower confidence interval; UCI: upper confidence interval.
p-value < 0.05 considered significant.
CCTA characteristics associated with all-cause mortality, non-fatal MI, or late revascularization
The difference in all-cause mortality was not significant between the three groups (Table 2). However, the two deaths recorded in the normal cohort were not related to CAD. One patient suffered a peri-procedural complication and another expired from complications with aortic regurgitation secondary to a prior traumatic aortic root dissection. Between obstructive and no CAD, there was a significant difference in non-fatal MI (2.5% vs 0%, p < 0.001) and late revascularization (2.5% vs 0.0%, p < 0.001). Between obstructive and non-obstructive CAD, there was a significant reduction in late revascularization only (2.5% vs 0.1%, p < 0.001). However, there was a trend toward a significantly increased incidence of non-fatal MI between obstructive and non-obstructive CAD (2.5% vs 0.9%, p = 0.195). There was no significant difference in the rate of non-fatal MI or late revascularization between non-obstructive and no CAD. Of note, there was no occurrence of non-fatal MI or need for late revascularization in patients without CAD by CCTA (Figure 2).
CCTA characteristics associated with ischemic stroke
Obstructive CAD was associated with a significantly higher incidence of ischemic stroke compared to non-obstructive CAD (3.8% vs 0.6%, p < 0.001) and no CAD (3.8% vs 0.4%, p < 0.001) (Table 2). In a separate Kaplan–Meier survival analysis of ischemic stroke based upon the severity of CAD, the mean ischemic stroke-free survival time was significantly shorter with obstructive CAD when compared to no CAD (1706 ± 44 days, 95% CI: 1621–1792 vs 2001 ± 10 days, 95% CI: 1969–2008; p < 0.001) (Figure 5). There was no difference in event-free survival between non-obstructive and no CAD. In the per-vessel analysis for ischemic stroke, the mean ischemic stroke-free survival time was significantly shorter when one-, two-, and three-vessel obstructive CAD was compared to no CAD (Figure 6). Cox proportional hazards multivariable regression analysis showed age (HR = 1.055, 95% CI: 10.55–1.108; p = 0.031) and obstructive CAD (HR = 3.742, 95% CI: 1.396–10.030; p = 0.009) to be independent risk factors associated with ischemic stroke (Table 7).

Kaplan–Meier curves comparing ischemic stroke-free survival stratified by severity of CAD.

Kaplan–Meier curves comparing ischemic stroke-free survival between one-, two- and three-vessel obstructive, non-obstructive, and no CAD.
Cox proportional hazards regression analysis for prediction of ischemic stroke.

CAD: coronary artery disease; HR: hazard ratio; SE: standard error; LCI: lower confidence interval; UCI: upper confidence interval.
p-value < 0.05 considered significant.
Discussion
Prognostic value of CCTA for ischemic stroke
Our goal was to investigate the implication of the severity of CAD on long-term cardiovascular prognosis, including ischemic stroke, in our single-center experience with CCTA. Apart from one study that investigated the association between CAC and ischemic stroke, there are no data on the prognostic value of CCTA for ischemic stroke. Our data demonstrate that the likelihood of ischemic stroke is directly proportional to the overall severity of CAD as well as the number of vessels with obstructive disease. Furthermore, the risk of ischemic stroke is significantly reduced and the mean ischemic stroke-free survival significant longer when free of disease by CCTA compared to those with obstructive CAD. When stratified by CAD, the pattern of event-free survival for ischemic stroke closely mirrored that of MACE-free survival, with nearly identical hazards for MACE. Given the prior associations between the degree CAC with extra-coronary plaque burden and ischemic stroke, not only are these findings not surprising but they further support cerebrovascular disease as a risk factor for CAD and vice versa. And now, our data add to the current literature on the prognostic application of CCTA, as a potential risk assessment tool for ischemic stroke.
Prognostic value of CCTA for MACE
Our main result is that patients who were free of disease by CCTA had excellent prognosis over a mean follow-up of 24 months, as demonstrated in the Kaplan–Meier MACE-free survival. Among the patients who were free of disease by CCTA, not only was the mean survival time significantly higher, there were no non-fatal MIs or need for late revascularization. With a normal CCTA study, these patients have a veritable intermediate-term (2-year) warranty from a standpoint of cardiovascular disease. Symptomatic patients without CAD by CCTA have a very low event rate, which provides these patients and their provider confidence regarding cardiovascular risk, to include ischemic stroke, as well as future military deployments and assignments. In our own military system, we have successfully utilized CCTA to expeditiously evaluate chest pain syndromes in our soldiers, sailors, marines, and airmen. Coupled with a reduced invasive coronary angiography referral rate and lower false-positive rate compared to myocardial perfusion imaging, 10 the excellent prognosis associated with a normal CCTA study has allowed for rapid return to duty or worldwide deployment.
There was an incrementally increasing association between the severity of CAD by CCTA and the rates of MACE as well as isolated endpoints of non-fatal MI, and late revascularization, consistent with the findings in prior prognostic studies. Our data demonstrated a significant increase in the incidence of MACE and ischemic stroke between both comparisons of obstructive versus non-obstructive CAD as well as obstructive versus no CAD. This is in contrast to some of the earlier works such as that by Elias-Smale et al., 11 where they evaluated 2153 asymptomatic subjects enrolled in the Rotterdam Study with a median follow-up of 3.5 years where asymptomatic disease burden in the setting of reclassified Framingham score based on degree of vascular bed calcification failed to predict incidence of stroke. Jensen et al., 12 in a much smaller study of 392 patients, evaluating the incidence of CAD on CCTA in between patients with acute ischemic stroke as compared to patients with acute chest pain, noted that there was a four-fold increased incidence of coronary plaque in the ischemic stroke group as compared to the risk factor matched cohort. Our study, however, evaluated the incidence of ischemic stroke based on degree of coronary disease burden in the setting of acute symptoms and its impact on future ischemic stroke event rates.
The difference in non-fatal MI between obstructive and non-obstructive CAD trended toward significance. Of the total three all-cause mortality cases in our patient cohort, there were two deaths recorded in patients with no angiographic disease and neither of which were related to coronary artery disease. Apart from this result, our findings are generally consistent with prior studies on the prognostic value of CCTA, with increased MACE outcomes directly proportional to the extent of CAD as well as the number of diseased vessels.2–5
Prior studies have shown significant differences in MACE outcomes between those with non-obstructive and no CAD.4,13 In our experience, there was no significant difference in composite MACE or the isolated endpoints of all-cause mortality, non-fatal MI, and late revascularization between non-obstructive and no CAD due to low power. However, there was a trend toward significance, with a higher incidence of MACE with non-obstructive versus no CAD.
Study limitations
This retrospective chart review is limited by the fact that this is a single, high-volume center experience with active duty military members included in our patient cohort, whose health status and physical fitness may not reflect the nation’s population as a whole. However, our military health system in San Antonio also provides medical care for dependents as well as enrolled retired military and their families, which helps diversify our study population to more closely mimic the general US population.
Furthermore, the presence of non-obstructive coronary atherosclerosis has been shown to predict cardiovascular mortality. 14 Therefore, the effect any post-CCTA medical treatment or risk factor control after detection of non-obstructive coronary plaques had upon the outcomes remains unknown.
Finally, our entire patient cohort comprised those with normal renal function, as a creatinine clearance of <60 prevented patients from undergoing CCTA in our institution. Patients with non-dialysis-dependent chronic kidney disease (CKD) as well as end-stage renal disease (ESRD) represent a population subset who have been shown to be at increased independent risk of cardiovascular mortality.14,15 Therefore, it remains unclear here what effect the presence of CKD or ESRD would have on MACE outcomes.
Future directions
Our data demonstrated excellent prognosis in patients free of disease by CCTA over an approximate follow-up of 24 months, which is similar to prior studies. With continued follow-up, we hope to better understand how severity of CAD impacts more distant cardiovascular prognosis using longer term studies. Additionally, we plan to assess how medical therapies and risk factor modification after the diagnosis of non-obstructive coronary atherosclerosis by CCTA affects cardiovascular outcomes.
Conclusion
The severity of CAD by CCTA is not only associated with increased incidence of MACE, it appears to be associated with increased incidence of ischemic stroke over 2 years, an association not previously made. The patterns of survival and risk factors for ischemic stroke identified here are nearly identical to those of MACE, supporting the close association between the cerebrovascular and cardiovascular atherosclerosis. Furthermore, with an average follow-up period of 2 years, we found that not only is intermediate-term cardiovascular prognosis closely related to the severity of CAD, being free of disease on CCTA was associated with very low risk of MACE. This 2-year cardiovascular warranty has the potential to reduce repeat cardiac studies and the cost burden affecting the medical industry.
Footnotes
Declaration of conflicting interests
The opinions in this manuscript do not constitute endorsement by San Antonio Army Medical Center, the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army, Department of Defense, or the US Government of the information contained therein. The authors declare that there are no conflicts of interest regarding the publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.