
Abstract
Objective:
Although the lymphatic complications such as lymphocele sometimes occur after surgery for varicose veins, the lymphatic function of such patients has not been evaluated. In this case report, we present a case of lymphocele after ligation surgery for varicose vein. We also detected subclinical dysfunction in lower limb using indocyanine green (ICG) lymphography.
Case report:
A 76 year- old female underwent ligation surgery for right lower leg varicose vein, and she noticed the squashy lesion in the medial side of the right knee. Three years later, she consulted our clinic and we performed ICG lymphography. We observed dermal backflow around the mass, which indicated lymphatic dysfunction. After injecting additional ICG around the knee, we punctured and drained the clear, yellow fluid from the mass and it was contrasted with ICG during the examination and the involvement of the lymphatic system was proven.
Introduction
The lymphatic complications such as lymphocele, lymphedema, or lymphatic fistula sometimes occur after surgery for varicose veins. 1 Although the risk of lymphatic complications was reported to be 2.2%, and lymphocele was the most frequent, the lymphatic function of the patients who have lymphatic complications has not been evaluated. 2 On the other hand, Suzuki et al. 3 investigated the lymphatic function before and after the surgery for varicose vein and reported that the impaired lymphatic function could recover with surgery for varicose vein.
In this case report, we present a case of lymphocele which was found after ligation surgery for varicose vein. We also detected subclinical dysfunction or lymphatic stasis in lower limb using indocyanine green (ICG) lymphography.4–6 This information may be able to enlighten the possibility of injury of lymphatic system and subsequent lymphedema during and after the treatment of varicose vein.
Case
A 76-year-old female underwent ligation surgery for right lower leg varicose vein in another hospital. Ligation was performed at one site in the medial knee and two sites in the lower leg. Soon after the surgery, she noticed the squashy lesion in the medial side of the right knee, which located close to the horizontal scar of the varix surgery. As the lesion gradually got larger and swelled out, she consulted the surgeon and underwent puncture of the lesion. Lymph-like yellow fluid was drained and the lesion got plain, which swelled again in a few days. She consulted our clinic 3 years after the surgery for detailed investigation of the lesion. At the first consultation, we found a subcutaneous mass which was 5 cm in diameter (Figure 1(a)). The mass was not accompanied by pain or redness, and did not have a history of inflammation. After 3 months, the mass got larger, and the skin above it thinned down, almost to be ulcerated. She had a history of diabetes mellitus and was under medical treatment. She was not allergic to any food or medicine.
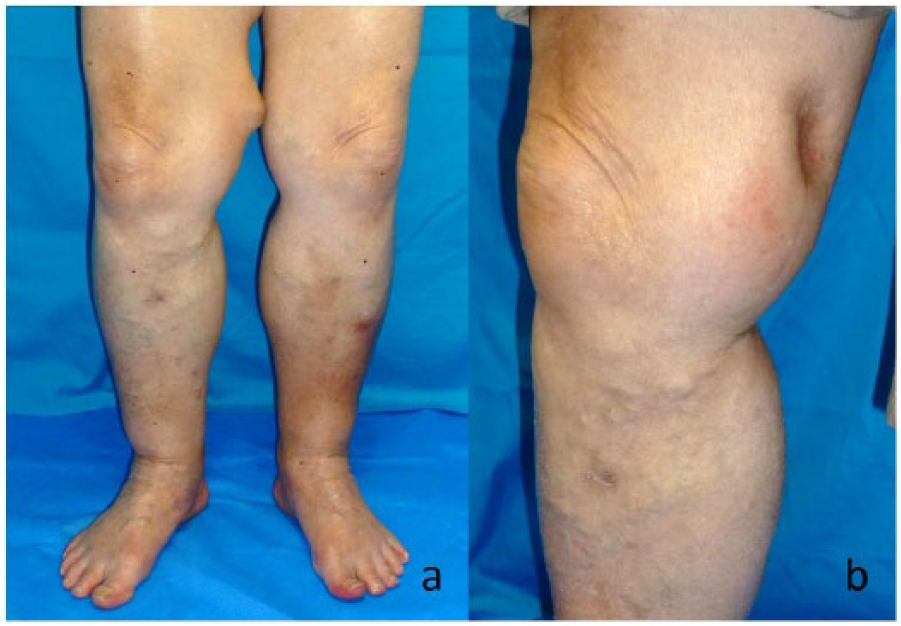
The clinical photograph of the patient: (a) the patient had 5 cm subcutaneous mass in her right thigh and (b) the site where the mass located formed depression after puncture and drainage of the content fluid.
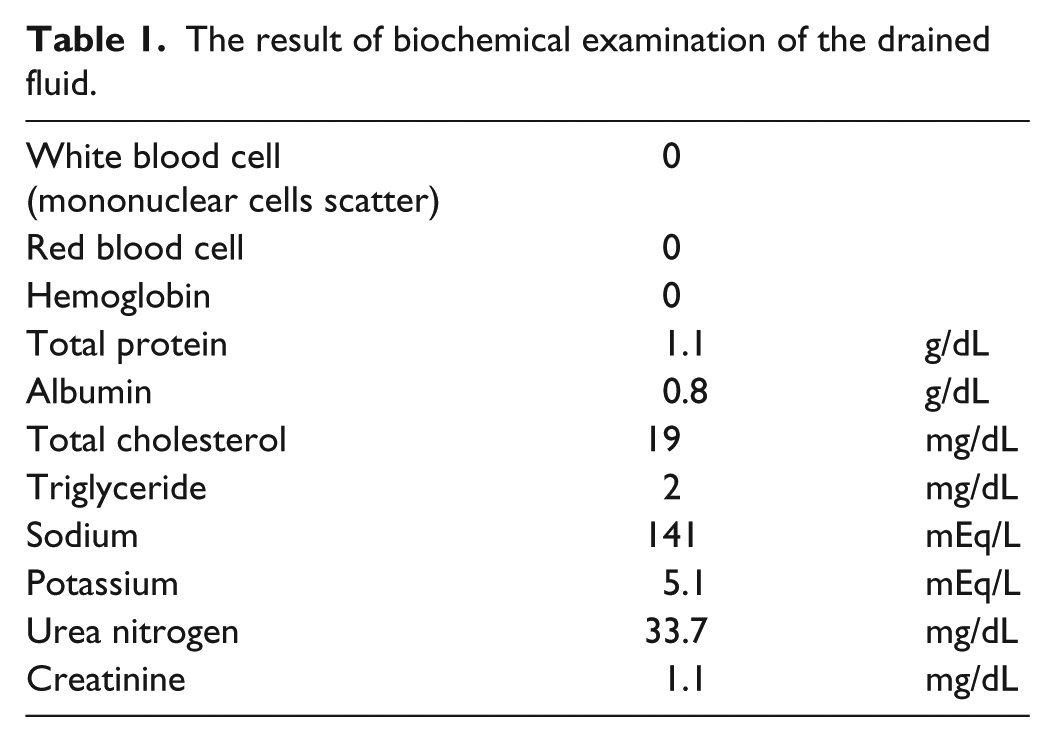
At first, we performed ICG lymphography to detect the involvement of lymphatic system to her lesion. After cannulating 22G catheter to the subcutaneous mass, we injected 0.1 mL of ICG (0.5% diagnogreen; Daiichi Pharmaceutical, Tokyo, Japan) subcutaneously into the first interdigital space of the bilateral feet. Lymphatic function was evaluated using an infrared camera system (Photodynamic Eye; Hamamatsu Photonics, Hamamatsu, Japan). Although we observed normal linear pattern from dorsum of the foot to the middle of the lower leg, stardust pattern, a kind of dermal backflow, was found around the mass, which indicated lymphatic dysfunction (Figure 2). After injecting additional ICG around the knee, we drained the clear, yellow fluid from the mass and observed it with Photodynamic Eye system (PDE, Hamamatsu Photonics KK, Hamamatsu, Japan). The fluid was contrasted with ICG during the examination, and the involvement of the lymphatic system was proven (Figure 3). Dermal backflow was not observed in the proximal thigh area. The result of biochemical examination of the drained fluid is shown in Table 1. We diagnosed the mass as lymphocele based on the examinations. Although the site where the mass had located formed depression after puncture (Figure 1(b)), it reoccurred in a few days. Although we planned lymphatic ligation and lymphaticovenous anastomosis (LVA) for this region, compression therapy after next puncture was effective, and the patient did not require surgical therapy.

The findings of indocyanine green (ICG) lymphography and the clinical photograph. Red circle: injection site of ICG (a) linear pattern can be seen in the dorsum of the foot, which indicates normal lymphatic function; (b) dermal backflow is observed around the knee and the subcutaneous mass (arrow), which means there is lymphatic dysfunction in this area; (c) collateral lymphatic vessels are developed around the subcutaneous mass (arrows); and (d) clinical photograph of the same site as (c).

The findings of indocyanine green (ICG) lymphography with color mapping mode: (a) green, blue, pink, and red colors indicate the existence and the relative concentration of ICG. Green color indicates lower concentration, and red color indicates higher concentration; (b) photograph of the drained yellow fluid; and (c) the drained fluid presents green color, which indicates the existence of ICG leaking from the lymphatic system.
The result of biochemical examination of the drained fluid.
Discussion/conclusion
In this case report, we presented a case who experienced lymphocele after varicose vein surgery. We demonstrated the presence of lymphatic dysfunction around the lymphocele using ICG lymphography.
There have been several papers to report the occurrence of lymphatic complications after varicose vein surgery.1,2 On the other hand, one paper reported that lymphatic function improved after varicose vein surgery. 3 In this case report, we showed that there was dermal backflow pattern in ICG lymphography around lymphocele, which means there was not only stasis of lymph but also lymphatic dysfunction or obstructive mechanism. This indicates that lymphatic function may decrease if there formed lymphocele after varicose vein surgery.
It is reported that there may be lymphatic dysfunction in the legs with varicose vein. Although there is a possibility of lymphatic dysfunction due to varix itself in this case, the dermal backflow in ICG lymphography was most severe around the lymphatic cyst, and the cyst located close to the incision. The cyst occurred after the varix surgery. Considering the timing of varix occurrence and location of the abnormality in ICG lymphography, the lymphatic dysfunction in this patient seems to be due to the surgery for varix.
In this case, we injected ICG in multiple sites. Of course, single-site ICG injection such as in the web space in the foot may be ideal, from the perspective of avoiding artifact. However, ICG injected in the web space sometimes does not reach to the area of concern in sufficient quantities because of the low lymphatic function or the dominancy of collateral lymphatic pathways. In such cases, multiple injection of ICG is beneficial to evaluate the lymphatic function in the area of concern. In this case, although ICG injected in the web space reached to the knee region, the discharge did not enhance, possibly because of the low lymphatic function. We injected additional ICG at the distal site of the cyst and could see ICG drainage from the cyst.
There are several reports to use ICG lymphography navigation for the treatment of lymphorrhea.7–9 As a treatment for such a condition in this patient, we recommended LVA to the patients. LVA is recently applied to lymphedema of the extremities.10–13 It was reported that LVA was effective for pelvic lymphocele after gynecologic cancer treatment. 14 The mechanism of LVA for lymphocele is preventing lymphatic influx into lymphocele and bypass the lymphatic flow to subcutaneous veins. There are various reports of treatment for lymphorrhea, such as sclerotherapy, lymphatic ligation, or resection of the cyst.15–17 It is reported that incidence of lymphedema is greater in patients with pelvic lymphocele after gynecologic cancer treatment, 18 and it is estimated that lymphedema is more incident in patients with lymphocele after varicose vein treatment. Therefore, LVA seemed to be ideal treatment for this case if the cyst re-occurs after puncturing once or twice.
In this case, although the patient experienced the recurrence of lymphatic cyst without compression therapy after the first puncture, could resulted in cure with compression therapy after the second puncture. Compression therapy seemed to be necessary to induce adhesion inside of the cyst.
It is only a case report about a rare complication after varix operation, and future accumulation of similar cases will be hoped. Also, although it is preferable to perform additional ICG lymphography to evaluate the lymphatic function after the cure of lymphatic cyst, it is difficult because the patient hopes to finish follow-up because the cyst had healed. Next examination may be performed when the patient consults us about the edema of her leg.
In this case report, we reported a case with postoperative lymphocele accompanied by lymphatic dysfunction which was demonstrated with ICG lymphography.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from Institutional Review Board (Saiseikai Kawaguchi General Hospital Ethical Review Board, approval code: 22-12).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.