
Abstract
Introduction
High quality nursing documentation and clinical reasoning competence are essential for safe and effective nursing practice, and interprofessional collaboration represents a key care process. This study examined the relationships among nurses’ quality of nursing documentation, interprofessional collaboration, and clinical reasoning competence.
Methods
A cross-sectional, descriptive, correlational, quantitative study was conducted among nurses working in multiple hospitals in Hue, Vietnam. Participants were recruited using convenience sampling. Data were collected from March to July 2025 using online and paper-based questionnaires. The Nurses Clinical Reasoning Scale, Interprofessional Collaboration Scale, and the Student Survey on Writing Nursing Care Plans were used. Descriptive statistics, Pearson correlation, and mediation analyses were performed.
Results
A total of 239 nurses were included in the final analysis. Correlation analysis showed that the quality of nursing documentation was positively associated with interprofessional collaboration (p < 0.001) and clinical reasoning competence (p < 0.001), and interprofessional collaboration was positively correlated with clinical reasoning competence (p < 0.001). Interprofessional collaboration significantly mediated the relationship between quality of nursing documentation and clinical reasoning competence (indirect effect β = 0.02, 95% CI [0.01, 0.04]), accounting for 11.5% of the total effect.
Conclusion
Interprofessional collaboration partially mediated the relationship between quality of nursing documentation and clinical reasoning competence, indicating that high-quality documentation enhances clinical reasoning both directly and indirectly through improved collaborative practice. These findings highlight the importance of strengthening documentation practices and interprofessional collaboration to support nurses’ clinical reasoning competence.
Introduction
Nursing documentation is a fundamental component of professional nursing practice and a key mechanism for ensuring patient safety, care quality, and continuity of care.1–3 It involves the systematic recording of patient information and nursing care activities across all stages of the nursing process, including assessment, diagnosis, care planning, implementation, and evaluation. 3 As a routine clinical practice, nursing documentation provides essential evidence of patient health status and nursing care, thereby improving the clarity, completeness, and consistency of clinical records. 4 In recent years, implementation of nursing documentation has increasingly incorporated standardized nursing languages, including diagnoses from NANDA International, the Nursing Outcomes Classification, and the Nursing Interventions Classification.3,5 These standardized terminologies facilitate structured care planning and contribute to improving the quality and consistency of documentation. Through the integration of these standardized terminologies, nursing documentation facilitates efficient information exchange and supports the accurate and systematic recording of patient care. 6 Beyond its legal and professional functions, nursing documentation promotes effective communication and information flow among interdisciplinary healthcare providers, thereby supporting coordinated, safe, and continuous patient care. 7 Comprehensive documentation of the nursing process, particularly the capture of nurses’ clinical reasoning, is essential for informed clinical decision making and patient safety.5,8 High quality documentation further contributes to improved patient outcomes by enhancing clarity, accountability, and consistency in clinical decision making.3,5
Clinical reasoning competence is essential for effective practice in dynamic healthcare environments, where growing clinical complexity requires nurses to continuously refine their reasoning processes to address evolving patient care demands.9,10 Clinical reasoning involves a complex cognitive process in which nurses collect and interpret patient information, recognize clinical cues, analyze possible explanations, and make informed decisions regarding patient care.10,11 Strong clinical reasoning enables nurses to prioritize patient problems, anticipate potential complications, and respond effectively to emerging clinical situations. Empirical evidence indicates that integrating clinical reasoning enhances nursing performance and supports timely, appropriate responses to complex patient situations, thereby improving the quality of care and patient outcomes.10,12 Moreover, examining clinical reasoning across health professions highlights variation in decision making approaches and underscores its potential to strengthen shared understanding and promote effective interprofessional collaboration. 13
In complex healthcare environments, effective care delivery requires the involvement of multiple professionals who contribute diverse areas of expertise and clinical perspectives. 14 Through these collaborative interactions, nurses have opportunities to exchange information, consider diverse professional perspectives, and integrate shared knowledge while gathering and analyzing patient information and evaluating its clinical significance, thereby supporting the development of their clinical reasoning. 10 Thus, effective clinical decision making increasingly depends on collaborative practices that enable healthcare providers to integrate diverse knowledge and address the unique and evolving needs of individual patients. 15 A previous study reported that interprofessional collaboration enables nurses to engage in shared decision making and coordinated care, providing access to diverse clinical perspectives that support the development and application of clinical reasoning competence. 16 Through collaborative interactions, nurses are better positioned to synthesize patient information, evaluate clinical priorities, and make sound judgments in complex situations. Consequently, interprofessional collaboration among healthcare providers, particularly nurses, has been consistently associated with improved patient outcomes, enhanced healthcare efficiency, and greater professional satisfaction.17,18
The Donabedian Model of Healthcare Quality, proposed by Donabedian, provides a systematic framework for evaluating healthcare quality through three interrelated components, including structure, process, and outcomes. 19 In the present study, this model was used as a conceptual framework to explain the relationships among quality of nursing documentation, interprofessional collaboration, and clinical reasoning competence. Within this model, structure refers to the organizational and informational resources that support care delivery, including the quality of nursing documentation practices. Process represents the interactions and communication among healthcare professionals during the provision of care, operationalized in this study as interprofessional collaboration. Outcome reflects the results of these processes, including professional competencies such as nurses’ clinical reasoning. This model provides a theoretical basis for understanding how the quality of nursing documentation influence nurses’ clinical reasoning competence through collaborative processes. Therefore, interprofessional collaboration might function as a mediating mechanism through which the quality of nursing documentation contributes to the development of nurses’ clinical reasoning competence. Therefore, this study was conducted to examine the relationships among quality of nursing documentation, interprofessional collaboration, and clinical reasoning competence. Understanding this relationship is critical for informing educational strategies, clinical practice improvements, and organizational policies aimed at strengthening nursing performance and patient safety.
Methods
Study design and participants
This cross-sectional, descriptive, correlational, and quantitative study was conducted among nurses working across multiple hospitals in Hue, Vietnam. Participants were recruited using convenience sampling. The inclusion criteria were: registered nurses currently working in clinical departments, direct involvement in patient care, at least one year of working experience in the hospital, and willingness to participate in the study. The exclusion criteria included nurses in administrative or managerial positions without direct patient care responsibilities.
Based on the G*Power sample size calculation for Pearson correlation analysis (α = 0.05, power = 0.90, effect size r = 0.30), a minimum of 111 participants was required. To compensate for an anticipated dropout or incomplete response rate of 20%, the target sample size was increased to 133 nurses. A total of 259 nurses were initially recruited for the study. Twenty questionnaires (7.7%) were excluded due to missing or incomplete responses on key study variables. Because the proportion of missing data was relatively small (<10%) and occurred across multiple variables without a systematic pattern, a complete-case analysis approach was adopted. No data imputation was performed. The final analytic sample consisted of 239 participants (92.3% of the initially recruited sample). The final sample size exceeded the minimum required sample size, thereby ensuring adequate statistical power.
Instruments
The self-designed questionnaire was distributed to collect demographic and clinical characteristics of participants in this study.
Clinical reasoning competence was measured using the Nurses’ Clinical Reasoning Scale developed by Liou and colleagues. 20 This instrument comprises 15 items rated on a five-point Likert scale and an original version demonstrated strong internal consistency, with a Cronbach’s alpha of 0.92. 20 For the present study, the scale was translated from English into Vietnamese using a standardized forward-backward translation procedure. 21 A pilot test was subsequently conducted with 15 nurses to evaluate the reliability of the translated version. The Vietnamese version demonstrated good internal consistency, with a Cronbach’s alpha of 0.85.
Interprofessional collaboration was assessed using the Interprofessional Collaboration Scale developed by Kenaszchuk and colleagues. 22 This self-administered instrument includes 13 items categorized into three domains: communication, accommodation, and isolation. Responses are recorded on a four-point Likert scale, with options ranging from 1 (“strongly disagree”) to 4 (“strongly agree”). 22 For the present study, the scale was translated from English into Vietnamese using a standardized forward-backward translation process to ensure linguistic accuracy and conceptual equivalence. 21 A pilot test was conducted with 15 nurses to evaluate clarity, cultural appropriateness, and reliability of the Vietnamese version. The instrument demonstrated good internal consistency, with a Cronbach’s alpha of 0.82, indicating its suitability for use in the study population.
The quality of nursing documentation was assessed using the Student Survey on Writing Nursing Care Plans developed by Salvador et al., which evaluates the clarity, completeness, and clinical logic of written nursing care plans. 23 The instrument encompasses five dimensions, including data gathering, identifying clients’ problems, formulating sustainable goals, providing appropriate interventions, and recognizing clients’ outcomes which a fundamental component of nursing documentation. Each item is rated on a five-point Likert scale ranging from 1 (poor) to 5 (excellent), yielding a total possible score ranging from 25 to 125, with higher scores indicating better quality of nursing documentation. 23 In the original study, the instrument demonstrated excellent internal consistency, with a Cronbach’s alpha coefficient (α) of 0.935. 23 Although originally developed for students, the instrument required no substantive modification for use with practicing nurses, as it reflects core care planning competencies. A pilot test was conducted with 15 nurses to evaluate the clarity, cultural appropriateness, and reliability of the Vietnamese version of the instrument. Participants were invited to provide feedback regarding item wording, clarity, and relevance to clinical practice. Based on their feedback, minor wording revisions were made to improve comprehension and contextual suitability. In the present study, the tool was subsequently administered to nurses working in a hospital setting, and the overall scale demonstrated good internal consistency, with a Cronbach’s alpha coefficient of 0.89.
Data analysis
Statistical analyses were conducted using SPSS version 24.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics, including means, standard deviations, and frequencies, were used to summarize participant characteristics and study variables. Pearson’s correlation analysis was performed to examine the relationships among key variables. To assess the mediating role of interprofessional collaboration, multiple linear regression analyses were conducted using the PROCESS Macro for SPSS.
Prior to statistical analysis, the dataset was screened for completeness and accuracy. The extent and pattern of missing data were examined. Questionnaires with substantial missing responses on key study variables were excluded from the analysis (n = 20). No statistical imputation procedures were performed because the level of missing data was below the commonly accepted threshold of 10%, minimizing risk of biased parameter estimates. All subsequent analyses were conducted using data from the 239 participants with complete responses.
Ethics statement
This study was approved by the Institutional Ethics Committee of Hue University of Medicine and Pharmacy (Approval No. H2025/061) and conducted in accordance with the Declaration of Helsinki. Participation was voluntary, and written informed consent was obtained from all participants prior to data collection. Confidentiality and anonymity were ensured by removing all identifying information, and data were used solely for research purposes.
Data collection procedure
Data were collected from March to July 2025 using both online and paper-based questionnaires. The online survey was administered via the Google Forms platform and did not collect any identifiable information. Prior to data collection, the researcher met with the chief nurse of each participating hospital to provide an overview of the study. Participants were recruited through head nurses, who disseminated the online survey link to eligible staff via email and Zalo groups, a widely used social networking application in Vietnam. The survey link provided access to the participant information sheet, informed consent form, and questionnaire. For participants who preferred paper-based questionnaires, the principal researcher distributed hard copies and placed secure collection boxes in each unit for the return of completed questionnaires.
Results
Characteristics of participants (n=239).
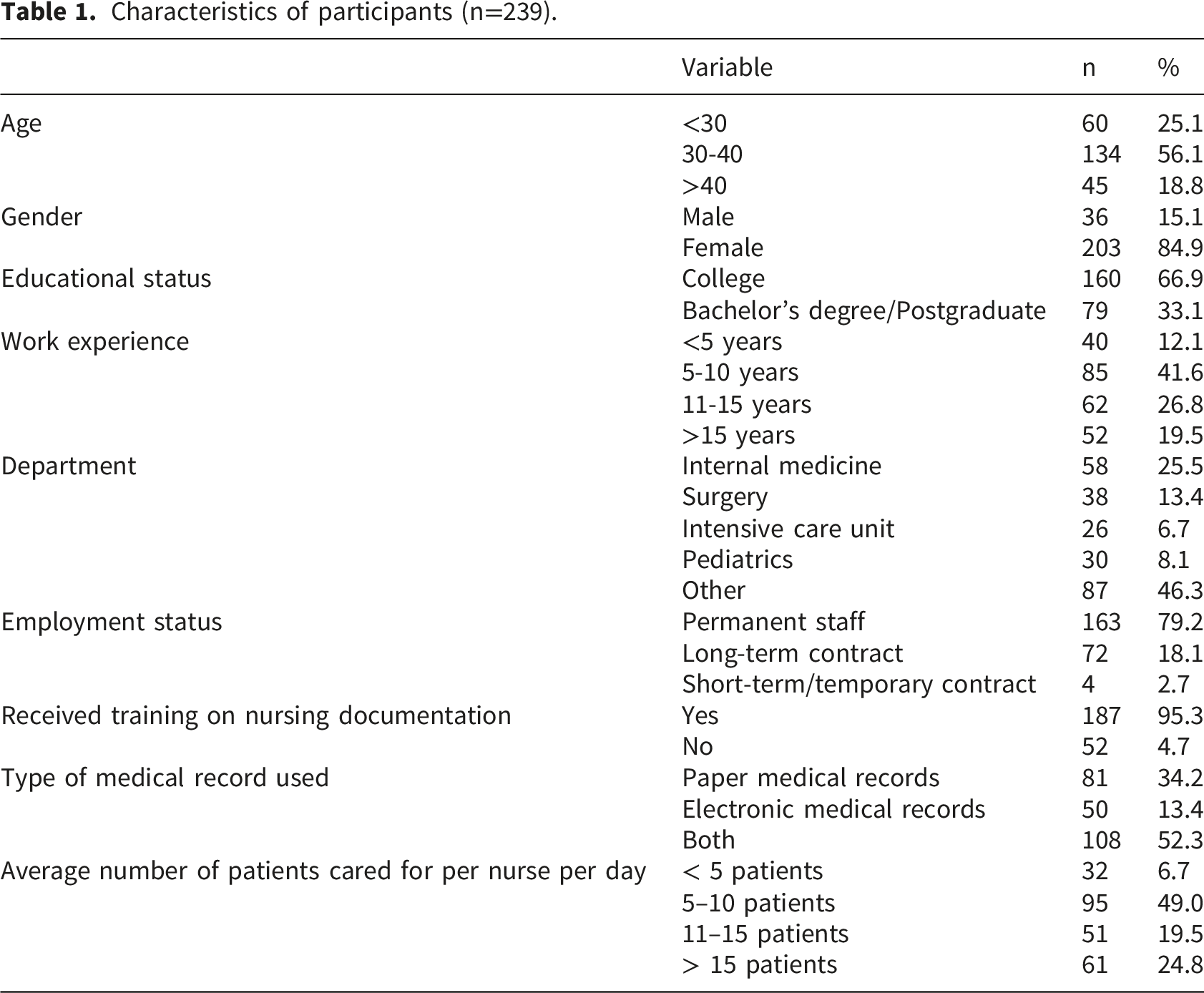
Participants were drawn from a range of clinical departments, with 25.5% working in internal medicine, 13.4% in surgery, 6.7% in the intensive care unit, and 8.1% in pediatrics, while 46.3% were from other departments. Most nurses were permanent staff (79.2%), with smaller proportions employed on long-term (18.1%) or short-term contracts (2.7%). Nearly all participants reported receiving training on nursing documentation (95.3%). More than half of the nurses used both paper and electronic medical records (52.3%), whereas 34.2% used paper records only and 13.4% used electronic records. In terms of workload, approximately half of the nurses reported caring for 5–10 patients per day (49.0%), while 24.8% cared for more than 15 patients, 19.5% for 11–15 patients, and 6.7% for fewer than five patients.
Correlation analysis of clinical reasoning competence, interprofessional collaboration, and quality of nursing documentation (n=239).

Note. * p<0.001.
Before conducting the regression and mediation analyses, the assumptions of linear regression were examined. Visual inspection of histograms and normal probability plots of standardized residuals indicated approximate normality. Homoscedasticity was assessed using scatterplots of standardized residuals against standardized predicted values, which showed no evident pattern or funnel shape, suggesting constant variance of errors. Multicollinearity was evaluated using variance inflation factor and tolerance statistics. All variance inflation factor values were below 2.0, and tolerance values exceeded 0.50, indicating no concerns regarding multicollinearity. These findings support the appropriateness of the regression models used in this study.
Mediation model for quality of nursing documentation and clinical reasoning competence.
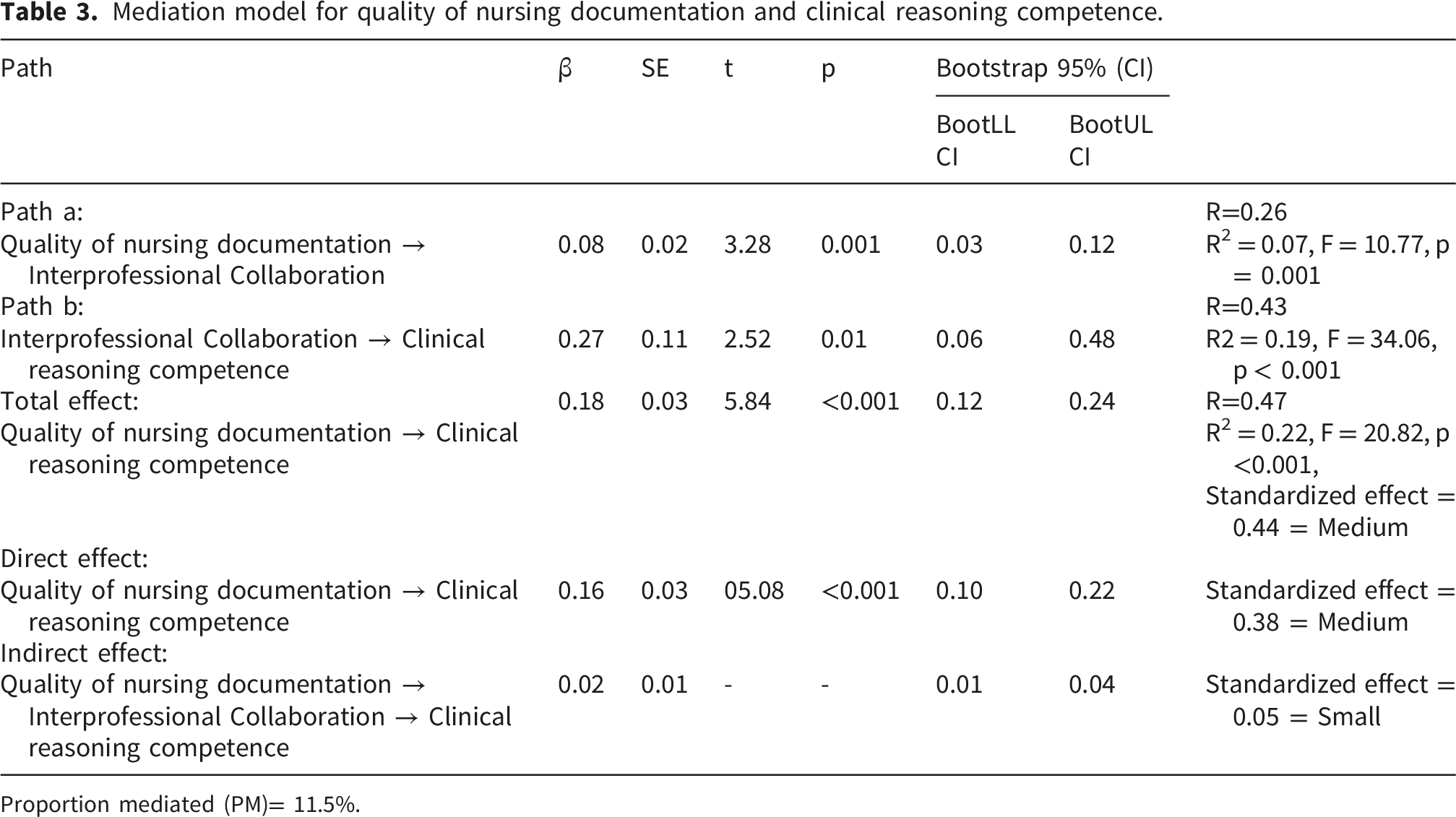
Proportion mediated (PM)= 11.5%.

Pathway of interprofessional collaboration in the relationship between quality of nursing documentation and clinical reasoning competence.
Discussion
This study examined the relationships among clinical reasoning competence, interprofessional collaboration, and quality of nursing documentation among clinical nurses working across multiple hospitals. The findings indicate that nurses demonstrated moderate to high levels across all three variables, suggesting that nurses are generally able to apply cognitive decision - making skills, engage in collaborative practices with other healthcare professionals, and maintain acceptable standards of documentation in routine clinical care.
Nurses demonstrated a moderate to high level of clinical reasoning competence, that they were generally able to integrate patient assessment findings, clinical knowledge, and contextual information to support effective clinical decision-making. These findings are broadly consistent with previous research conducted in different healthcare contexts. Noh and Kang (2024) reported a mean clinical reasoning competence score of 59.72 ± 8.01 among Korean oncology nurses. 12 Liu et al. (2025) found that clinical reasoning competence among nurses ranged from 56.24 ± 7.29 to 64.65 ± 6.69. 24 In a European context, Notarnicola et al. (2024) reported a higher mean score of 62.98 among Italian registered nurses. 25 Although some variation exists across countries and clinical settings, overall findings suggest that nurses generally demonstrate moderate to high levels of clinical reasoning competence. This competence enables nurses to effectively interpret patient conditions, prioritize care needs, and implement appropriate interventions in complex clinical situations. In addition, the relatively high level observed in this study could be related to recent developments in healthcare systems, particularly the increasing adoption of electronic health record systems in many hospitals. In Vietnam, healthcare institutions have increasingly implemented electronic health information systems to improve management of clinical information. In particular, nursing documentation has progressively incorporated standardized nursing languages within the nursing process. Such developments could strengthen the systematic recording of patient care and facilitate clearer communication of nursing assessments, interventions, and outcomes, thereby supporting more informed clinical decision-making in increasingly complex healthcare environments.
Furthermore, digitalization of clinical information has the potential to strengthen interdisciplinary communication and facilitate information sharing among healthcare professionals. When nurses could readily access updated patient information from multiple sources within an electronic system, they might be better positioned to interpret patient conditions and participate more actively in collaborative decision making processes. Electronic records could therefore function as a shared informational platform that supports coordinated care and mutual understanding among members of the healthcare team. However, despite these technological advancements, challenges related to interprofessional collaboration still persist in some healthcare settings. For example, a study conducted at the primary care level by Huyen et al. (2024) reported that healthcare providers from different professional disciplines frequently experienced a “lack of collaborative practice”. 26 These findings suggest that structural and organizational barriers, including hierarchical professional relationships, unclear role delineation, and limited opportunities for structured interprofessional communication, continue to hinder effective collaboration.
The present study found that clinical reasoning competence was significantly and positively correlated with both interprofessional collaboration and quality of nursing documentation. In framework of Donabedian model, quality of nursing documentation represents a critical component of care process that structures how clinical information is collected, interpreted, and communicated. High-quality nursing documentation support initial stages of this process by structuring patient information in a systematic and accessible format, thereby facilitating the noticing and interpretation of clinically relevant cues. Consistent with this perspective, previous research has shown that structured documentation systems could enhance nurses’ clinical reasoning by improving the organization and accessibility of patient information during care planning and evaluation. 27 Beyond these individual cognitive processes, the findings also suggest that documentation contributes to clinical reasoning through interpersonal mechanism. The mediating role of interprofessional collaboration indicates that well-structured documentation enhance clarity and accessibility of clinical information shared among healthcare professionals. Clear documentation provides a common informational platform that facilitates communication and discussion within interprofessional teams. Through collaborative interpretation of documented patient information, nurses encounter diverse professional perspectives, alternative interpretations of clinical data, and shared problem-solving approaches, which broaden their understanding of patient conditions and support more comprehensive clinical judgments. Evidence suggests that patient documentation serves as a catalyst for interprofessional collaboration, are actively involved in organizing patient care. 28 Moreover, interprofessional documentation has been recognized as an effective strategy for strengthening coordination and collaboration within interprofessional care teams. 29 From the perspective of Donabedian framework, improving documentation quality might therefore strengthen both the informational infrastructure that supports clinical reasoning and the collaborative processes through which clinical knowledge is exchanged in healthcare teams. These collaborative interactions promote reflective thinking and the integration of multidisciplinary knowledge into clinical decision-making. This finding supports the view that clinical reasoning is a socially situated and context-dependent competency, shaped through professional interactions as well as individual cognitive processes. 30
Limitations
This study has several limitations. First, the cross-sectional design limits the ability to establish causal relationships among quality of nursing documentation, interprofessional collaboration, and clinical reasoning competence. Although mediation analysis was used to explore potential pathways, the cross-sectional nature of the data does not permit temporal inference, and the findings should therefore be interpreted as associative rather than causal. Second, all variables were measured using self-administered questionnaires, which might introduce response-related biases such as social desirability bias. The reliance on a single data source may also increase the risk of common method variance, potentially inflating the observed associations among variables. Third, convenience sampling was used to recruit participants from a limited number of healthcare institutions, which may introduce sampling bias and limit the representativeness of the study population. Finally, other organizational and contextual factors not examined in this study also influence nurses’ clinical reasoning competence.
Implications for practice
These findings underscore the need to strengthen nursing documentation practices and interprofessional collaboration to enhance nurses’ clinical reasoning competence. High quality documentation should be recognized as a critical clinical communication tool that supports continuity of care and informed decision making, rather than as a purely administrative task. Healthcare organizations are encouraged to implement standardized documentation systems and provide ongoing training to improve documentation quality. The mediating role of interprofessional collaboration highlights the importance of cultivating collaborative practice environments through structured interdisciplinary communication and shared care planning. Nurse leaders and educators should embed documentation and collaboration competencies into clinical education, mentorship, and performance evaluation. Collectively, these strategies have the potential to strengthen clinical reasoning and promote safer, higher quality patient care.
Conclusions
This study found that the quality of nursing documentation was significantly associated with nurses’ clinical reasoning competence, with interprofessional collaboration mediating a small portion of this relationship. The findings suggest that effective documentation and collaborative team interactions are complementary factors that might support the development of clinical reasoning in nursing practice. Future longitudinal and multi-method research is needed to further clarify the mechanisms linking documentation, collaboration, and clinical reasoning competence.
Footnotes
Acknowledgments
The authors would like to extend their gratitude to all participants who contributed to this study.
Ethical considerations
This study was approved by the Institutional Ethics Committee of Hue University of Medicine and Pharmacy (Approval No. H2025/061) and conducted in accordance with the Declaration of Helsinki.
Consent to participate
Participation was voluntary, and written informed consent was obtained from all participants prior to data collection. Confidentiality and anonymity were ensured by removing all identifying information, and data were used solely for research purposes.
Consent for publication
Not applicable, as all data were anonymized and no identifiable information is included.
Author contributions
TTTH, BDH, Data curation: TTTH, Formal analysis: TTTH, Investigation: TTTH, Methodology: TTTH, BDH, Writing – original draft: TTTH, Writing – review & editing: TTTH, BDH.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.