
Abstract
Objective:
With regard to limitation in national budget, the relevant authorities of healthcare and treatment throughout the globe are seeking the use of available resources in a way that no wastage of money or time—which is, of course, convertible to money—is acceptable. This study sought the opinions of hospital doctors and nurses on those activities at work that wasted their time.
Methods:
A questionnaire designed to identify activities that waste time during hospital care was completed based on the review of previous studies and including hospital wastes items. The authors designed a questionnaire, which was filled out by 209 nurses and 30 doctors in the surgery wards in hospitals affiliated to Shiraz University of Medical Sciences (SUMS). The items for time wasting activities were extracted from previous studies, and the reliability of the questionnaire was more than 0.785 using Cronbach’s alpha. The response rate was more than 60%.
Results:
The mean age of the participating nurses and doctors was 30.24 ± 6.85 and 32.77 ± 7.05 years. In all aspects, more time was wasted during the morning and evening shifts in comparison with the night shifts. The activity that was thought to waste time in hospital care the most was paper-based documentation. Preventable wasted time during the shift was 16%–30% in the nurses’ view and 18%–34% in the doctors’ view. For both nurses and doctors, the highest-rated preventable wasted time was related to time spent waiting in ward for lab data responses, transfer of patients, or delivery of care.
Conclusion:
Hospital working environment is complex, and opportunities for improvement of the efficiency of the nurses’ and doctors’ workload should be analyzed, case by case, in each hospital and work group. Process change (for the decrease in the wasted time for waiting in wards), simple innovative ways (for the decrease in the wasted time for searching the needed equipment), using hospital information system technology for documentation, communication, and the better design of the wards (to decrease the wasted time due to transfer between the ward and restroom) could be helpful for improving efficiency and for a safer and acceptable delivery of care.
Keywords
Introduction
Hospitals are important treatment service providers. According to the latest study of the National Health Accounts (NHA) by Ministry of Health (MOH) and Statistical Center of Iran (SCI), 24.1% of the total health expenditures (THEs) corresponding to healthcare and treatment were related to hospital costs. The aforementioned costs are known as the sixth factor for healthcare costs of a family (7.7%). 1 With regard to limitation in national budget, the relevant authorities of healthcare and treatment throughout the globe are seeking the use of available resources in an efficient way. Apparently, no wastage of money or time—which is, of course, convertible to money—is acceptable. Therefore, identifying the causes of such wastage and proposals for solutions to prevent it is highly desirable. Indeed, due to large contribution of the healthcare and treatment costs of the hospitals, as well as the importance of hospitals in the healthcare system, an investigation on the kinds and hospital wastes (treatment and non-treatment) has attracted the attention of scientists. Hospital wastage comprises various types and has different causes, which includes not only financial costs but also time and dissipated energy. Different groups play a role in hospital waste, including nurses, doctors, and so on.
Nurses are an important group that provides healthcare services in hospitals. In a study, it was shown that the largest fraction of the nurses’ time (75% of the elapsed time) is allocated to activities related to nursing measures, while the rest of the elapsed effective time is devoted to patient care activities, documentation, and the coordination of patient care, respectively. 2 On average, the time nurses spend with patients is only 31% of their total time. 3 A study on the causes of the nurses’ time wastages showed that the positioning characteristics of a related ward affected the nurses’ movements between the wards, as well as the frequency in which the nurses enter the patients’ rooms or the nurses’ station. 4 An effective cause of wasted time (for nurses and doctors) and duration of patients’ hospitalization is difficulty in making a connection between the patients and healthcare workers. In the United States, it is estimated that more than US$12 billion is wasted annually because of the inefficiency in making a connection between healthcare service providers.
Also, the effect of hospital information systems (HISs) on hospital wastes has been investigated. In a study, in order to analyze the effect of computer-based documentation of hospital information, hospital employees had a less positive attitude toward computer-based documentation. 5 Up to now, the studies that have been carried out on hospital wastes are far few, have only evaluated limited aspects of waste, and are heterogeneous from different health systems.
Up to now, there are few researches that have assessed the attitude of nurses on the main causes of wastes, or their opinions as to how situations could be improved by implementing a better management. It is possible to reduce the amount of wastage through consultation with authorities and using management methods, specifically the process of improvement. To this end, this study sought the opinions of hospital doctors and nurses on those activities at work that wasted their time
Methods
This cross-sectional study was conducted within all surgery wards of the Shiraz hospitals affiliated to Shiraz University of Medical Sciences by Health Policy Research Center in the year 2015. A pre-defined questionnaire was distributed among all the nurses and doctors that work in these wards. Nurses and doctors who consented to participate in the study filled in the questionnaires and submitted them. A total of 209 nurses and 30 doctors submitted the questionnaires, and the response rate of which was more than 60%.
Considering the fact that there had been no previous questionnaire that covers all the aspects of hospital wastage, the questionnaire was, therefore, prepared through a review of previous studies, together with experts’ opinion. The content and face validity of this questionnaire was approved by a group of faculty members of the Health Policy Research Center who had practical experience in hospitals.6,7 After conducting the questionnaire on 30 people, the reliability of the questionnaire was calculated using Cronbach’s alpha, and the required improvements were applied with respect to the nurses’ and doctors’ responses. The calculated Cronbach’s alpha for all the scales was higher than 0.785.
The questionnaire includes demographic characteristics of participants as well as two scales: important sources for wastage in hospital and total preventable wasted time (PWT) (as percentage of shift time). We asked the nurses to score the important sources of wastage in the hospital (money, time, etc.) among 17 possible causes that include Hospital information system (HIS), Paper-based documentation, Elective surgery cancelation, Unnecessary operations, Search for equipment, Lack of the required equipment in the ward, Waiting for lab data preparation, Waiting for service delivery, Intra-unit patient transport, Intra-unit travel of staff, Communication problems (with patients), Non-compliance of patients, Low health literacy of patients and visitors, Irrational use of medication and antibiotics, Nosocomial infections, Attendance at physician rounds and in nurses rounds (for nurses), and Transfer between the wards and the restroom (for doctors). We asked the participants to score each item if they agreed that the item was an important source of hospital wastage, from 0 as the lowest to 4 as the highest rate. Each participant could rate several items and also it was possible to add their suggestions for further item. Then, we ordered the mean score of each item to understand important sources of wastage in each hospital.
For better understanding of the PWT as the percentage of the shift time, we asked the participant to answer the three questions (four questions for doctors) with a description: in each shift how much time (hour) do you spend for each of the following options? Keep in mind that this time could be prevented with better management:
Time spent for waiting in the ward (time waiting for lab data responses, transfer of patients, or delivery of care);
Time wasted by searching for the required equipment;
Time wasted by transferring in ward between the patients’ room or between the patient’s room and the nursing station;
Time wasted by transferring between ward and restroom (only indicated for doctors).
Then, the answers were converted to percentage of each shift, and mean score ± standard deviation (SD) was calculated for each question by hospital scale, subspecialty versus general hospital and nurse versus physician view. We also asked a complementary question about the view of the staff regarding HIS use (whether the usage of HIS would decrease/increase/I have no opinion about its effect on the wastage of time, the wastage of money, error, and phone call).
The input criteria included the nurses working in the surgery wards and doctors (consisting of a doctor and nurse who were continuously providing services for 6 months), and also willingness to fill out the questionnaire. To make it more trustable, we distributed the questionnaire among all members of staff during the morning, evening, and night shifts.
Doctor in this study is defined as a general medical doctor who works in the hospital. He or she has the work experience from less than 6 months to several years (in this study, 28 years).
After gathering the data, the data were entered into SPSS software and analyzed using descriptive and analytical statistics. Average and SD were calculated within the descriptive statistics, and Mann–Whitney U test was implemented within the analytical statistics. p < 0.05 was considered statistically significant for the analyses.
Results
The characteristics of 209 nurses and 30 physicians (of 35 wards) who participated from 9 (of 13 hospitals) hospitals are presented in Table 1. The most important causes of wastage in hospitals among 17 possible causes in the nurses’ view were paper-based documentation, elective surgery cancelation, attendance in physician rounds, waiting for service delivery, and low health literacy of the patients and visitors. In the physicians’ views, they were paper-based documentation, nosocomial infection, transferring between wards and the restroom, and antibiotic overuse. Mean score ± SD of the most important sources of hospital wastage in the nurses’ and physicians’ view is presented in Table 2.
Characteristics of the participants (209 nurses and 30 physicians).

SD: standard deviation.
The most important sources for wastage in the hospital, as viewed by nurses and physicians.
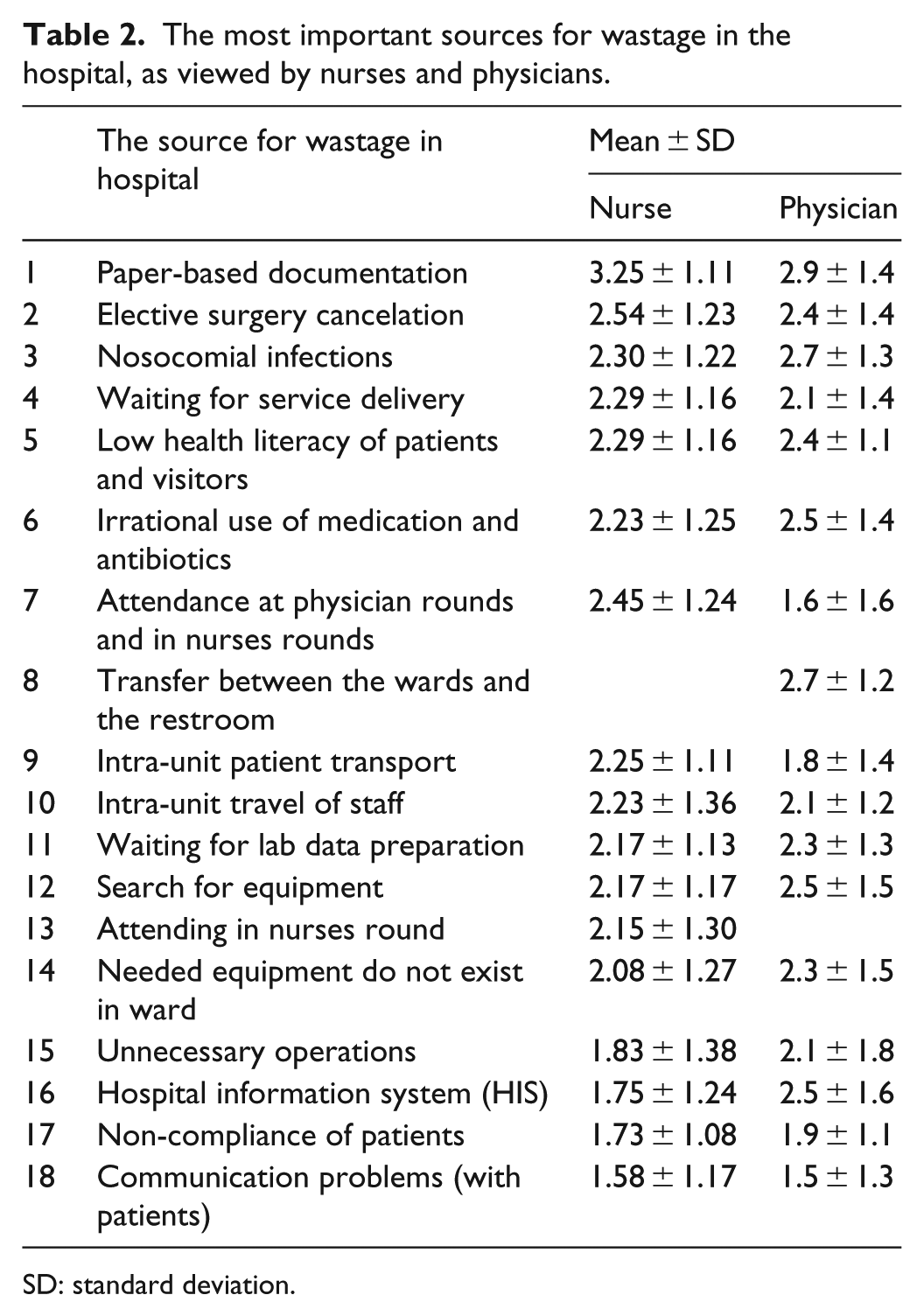
SD: standard deviation.
The total self-stated PWT (percentage of shift time) as a mean ± SD is shown in Table 3. Also, self-stated PWT (percentage of shift time) as a mean ± SD (median) for general and subspecialty hospitals separately, in the nurses’ and physicians’ views, are available in Appendices (Supplemental Tables 1–4, respectively).
Total self-stated PWT as the percentage of the shift time for the nurses and physicians separately.

PWT: preventable wasted time.
Data presented as mean ± SD.
Comparison between self-stated PWT of physicians and nurses.
Time spent for waiting in ward (time waiting for lab data responses, transfer of patients, or delivery of care).
Time wasted by searching for needed equipment.
Time wasted by transferring in ward between patients room or between patients room and nurse station.
Only indicated for physicians, Time wasted by transferring between ward and restroom.
There was no significant difference between the age (p value = 0.41), job experience (p value = 0.26), or PWT. There was no significant difference between different job roles (nurses’ aides, nurse in charge, head nurses, and supervisors), not only for the total PWT (p value = 0.44) but also for the subsets of PWT: the waiting time spent in the ward (p value = 0.48), searching for the required equipment (p value = 0.57), and by transferring to the wards (p value = 0.57).
There was no significant difference in various types of job recruitment, not only in total PWT (p value = 0.18) but also for the subsets of PWT: the time spent waiting in the wards (p value = 0.22), searching for the required equipment (p value = 0.41), and by transferring to the wards (p value = 0.41). 41.2% (68) of the nurses stated that HIS could save time and 51.7% (77) believed that it could decrease medical errors and unnecessary phone calls (50.4% (70)).
Discussion
The top stated cause of wastage of time in the hospital among 17 possible causes, from the nurses’ and physicians’ views, was paper-based documentation. This source of wastage should be taken into consideration because it may lead to resistance to documentation. In some circumstances where there was resistance to documenting the data, this could be influenced by extrinsic (environmental factors) and intrinsic factors, or cognitive and psychosocial factors (lack of confidence about written documents, impossibility of writing the reports due to the nature of nursing practice). 8 Interestingly, neither nurses nor physicians stated that this task (paper-based documentation) was a suitable method for PWT, possibly because this task is a time-consuming activity rather than time wasting one, or perhaps, they had a positive attitude toward paper-based documentation as prevention against lawsuits, or they were not aware of the potentials of HIS because of poor user participation. 9 HIS in Shiraz hospitals is simply a way for documenting, accelerating, tracing, and performing the administrative and financial tasks rather than an efficient method of recording and communicating the patients’ medical and clinical information.
One of the top resources of wastage in hospitals was low literacy levels of the patients and visitors. A strong association of low literacy ability with hospital admission and readmission and its high monetary burden has been shown in other studies. 10
However, except for paper-based documentation and nosocomial infection, the nurses and doctors differently scored the top source of hospital wastage. For instance, the doctors pointed that nosocomial infection and antibiotic overuse are a waste of time and/or resources in hospitals. This shows that doctors have a positive attitude when it comes to controlling and changing this issue. It is widely accepted that the control of nosocomial infection, because of the considerable cost it imposes on hospitals, is one of the most available cost-effective interventions in hospitals.11,12
Doctors also pointed to “Transferring between the wards and restroom” as one of the main sources of hospital wastage. More PWT was stated by the doctors compared to nurses, so that the time wasted by transferring between wards and the restroom contributed to a large amount of wastage in some hospitals, which should be considered when locating the physicians’ restroom near the ward. Better ward design not only decreases the wasted time but can also improve the effectiveness and satisfaction of the staff. 13 Besides the ward design, other environmental factors affect the effectiveness of the staff, such as “lighting levels and auditory or visual distractions,” which requires further studies. 13
Total PWT in the hospital staff’s view was almost one-third of the shifts. In general, more time was wasted during morning and evening shifts in comparison to night shifts. This was because more elective surgeries are performed in the morning, and in some cases, it continues into the afternoon. Therefore, there was more workload in the morning and afternoon than at night in surgical wards, while the stated wastage occurs more in the morning and evening than at night.
Nurses of general hospitals stated more total PWT time than subspecialty hospitals. However, in subspecialty hospitals, it seems that workload and the degree of critical status of patients influence PWT of the hospital. For example, a subspecialty hospital of trauma patients (R), which has more complicated and critical units, has more wastage than an orthopedics (C) subspecialty hospital or an Ear–Nose–Throat (ENT) subspecialty hospital (K) (Supplemental Tables 1–4 in Appendices).
Overcrowding of hospitals and emergency departments could be associated with a relative increase in the early mortality for 30% of patients, while nursing shortage accounted for higher mortality rate after 30 days for surgical patients, and more dissatisfaction and burnout of nurses, 14 which was independent from the confounding factors. 15 Although the effect of workload on the outcome of patients has been studied before, it seems that these effects should be reviewed in relation to wastage of time and resources. Even though high workload is inevitable, some aspects could be prevented by better managerial issues and change in the processes. For instance, in the case of excessive workload during mornings and in the evenings, it is suggested that in surgical wards, a selected number of surgeries should be performed during the evenings to ease the burden of workload for the morning shift. As a result, patients’ outcome, errors, and wastages will be influenced and healthcare workers can directly get involved by providing care as they are skilled and trained.
This study aimed to evaluate the main causes for wastage of resources, with particular focus on time wastage in hospitals from the point of view of hospital staff through an instructor-developed questionnaire. The participants’ views as found in this study can reveal other aspects of hospital management, for example, flaws in the processes. It is also feasible to implement this reliable and valid questionnaire in other hospitals, or it could be implemented periodically in a single hospital to make a comparison. However, there are other ways to evaluate the amount of time that each healthcare worker spends and wastes, but each of these methods has their own specific limitation in our setting. For example, in the observation method, if the person under observation changes his or her behavior, 16 then the data might become biased. Using accelerometers for tracing the wasted time is not feasible in all settings. 2 Therefore, this study failed to objectively evaluate the time really wasted by these hospital staff. Studies with more objective measures on potential sources of time wastage are highly recommended.
Conclusion
These findings indicate that the hospital working environment is complex and opportunities for improvement of the efficiency of nurses’ and physicians’ workload should be analyzed, case by case, in each hospital and work groups. Process change (for the decrease of the wasted time for waiting in the wards), simple innovative ways (for the decrease of the wasted time for searching the required equipment), using HIS technology for documentation, communication, and better design of wards (to decrease the wasted time due to transferring between the ward and restroom) could be helpful for improving efficiency and a safer and acceptable delivery of care.
Supplemental Material
appendix_2 – Supplemental material for What do hospital doctors and nurses think wastes their time?
Supplemental material, appendix_2 for What do hospital doctors and nurses think wastes their time? by Kamran Bagheri Lankarani, Sulmaz Ghahramani, Marjan Roozitalab, Mohammadreza Zakeri, Behnam Honarvar and Hengameh Kasraei in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank all the participants in this study. The authors also thank the research center and consultation, and Dr Nasrin Shokrpour for editing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Ethics Committee of Shiraz University of Medical Sciences.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by Deputy of Research of Shiraz University of Medical Sciences (research code: 94-01-62-9866).
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.