
Abstract
Introduction:
Patients with chronic conditions can improve their health through participation in self-care programs. However, awareness of and enrollment in these programs are generally low.
Objective:
We sought to identify factors influencing patients’ receptiveness to a referral for programs and services supporting chronic disease management.
Methods:
We analyzed data from 541 high-risk diabetic patients who completed an assessment between 2010 and 2013 from a computer-based, nurse-led Navigator referral program within a large primary care clinic. We compared patients who accepted a referral to those who declined.
Results:
A total of 318 patients (75%) accepted 583 referrals, of which 52% were for self-care programs. Patients who accepted a referral had more primary care visits in the previous year, were more likely to be enrolled in another program, expressed more interest in using the phone and family or friends for support, and were more likely to report recent pain than those who declined a referral.
Discussion:
Understanding what factors influence patients’ decisions to consider and participate in self-care programs has important implications for program design and development of strategies to connect patients to programs. This work informs outreach efforts to identify and engage patients who are likely to benefit from self-care activities.
Introduction
Chronic disease places an enormous burden on both the individuals affected and the health care system as a whole. Over 130 million Americans have been diagnosed with at least one chronic disease,1–3 and this number is increasing, including within the Veteran population.4,5 While the prevalence of chronic conditions increases, the supply of primary care providers (PCPs) and registered nurses (RNs) is dwindling, creating a gap in available health care. 2 One way the medical community is addressing this problem is through the patient-centered medical home (PCMH) model. The PCMH redesigns primary care into an efficient and comprehensive model of care. 6 It promotes programs and care activities that are patient driven and inclusive of patients and families and is accessible, continuous, coordinated, and team based7–9 with the primary care RN serving as the care coordinator. Additionally, PCMH incorporates health information technologies and patient registries for improved coordination of care. 9
In 2010, the Veterans Health Administration (VHA) began to implement the PCMH model, called Patient Aligned Care Teams (PACT), at all VHA primary care facilities nationwide. 10 In conjunction with that effort, Veterans Affairs Ann Arbor Healthcare System (VAAAHS) was selected as one of five national PACT Demonstration Laboratories charged with facilitating and evaluating implementation of the PACT model. 11 As part of this work, we developed and piloted a novel, computer-based, RN-delivered program called the Navigator, which was designed to connect patients to self-management programs, by offering program referrals based on patients’ needs and preferences. 12
The VAAAHS has a myriad of self-care programs available to patients with chronic disease. Generally, these programs are delivered by health care professionals who educate patients and families and provide them with the skills necessary to effectively manage their conditions. Evaluations of certain VHA-based programs have demonstrated some effectiveness in terms of improved patient–provider communication, 13 weight loss, 14 reduced hospital admissions,15,16 and improved self-care and clinical outcomes. 17 Past research has demonstrated that patients who are actively engaged in self-management activities experience improved health outcomes, better care, and a higher quality of life.18–24 However, patient enrollment in chronic disease management programs is low nationally, 25 due to multiple factors, including patients’ and even their providers’ lack of awareness of available programs or eligibility requirements.26–28
The Navigator was created as an RN-led platform to address barriers to program participation by identifying patients’ preferences and health care needs, by promoting interactions between patients and primary care nurses, and by increasing patient and provider awareness of available programs. This was accomplished through the use of a structured assessment, conducted over the phone, and an algorithm that identified programs that may fit with patients’ needs and preferences. 12 Importantly, the Navigator was aligned with PACT goals that emphasize team-based care, utilizing RNs in the management and coordination of patient care.
Aims
Although studies have examined how recruitment methods and patient characteristics can influence patient engagement and retention in self-management programs, 29 less is known about the factors affecting patients’ receptiveness to referrals for care management programs and services. To our knowledge, previous research has not studied patient-centered referrals, which are derived by matching patients to self-management programs. Understanding characteristics that may predict patients’ acceptance of a referral can help guide outreach efforts to engage patients in programs. Thus, we conducted a retrospective descriptive assessment of data collected as part of the Navigator program to identify factors associated with patients’ receptivity to referrals for care management programs and services.
Methods
Navigator program
A detailed account of the development, features, and assessment tools of the Navigator is previously published. 12 Briefly, the goal of the Navigator tool is to match patients with chronic diseases or conditions to self-care programs and to provide the patients with referrals to those programs. A primary care–based RN uses the tool to proactively call patients on the phone and guide them through an initial assessment covering 17 domains, including social support, cognitive status, depression, pain, self-efficacy, and technology use. 12 The Navigator tool utilizes the assessment information to identify programs that match the patient’s needs and care preferences. Guided by further discussion with the patient, the RN provides more information about available programs and offers a referral to those programs of interest to the patient. The patient can accept or decline the referral(s); however, patients were limited to two programs at a time to avoid too many patient contacts.
Through their conversations with patients, nurses using the Navigator often identified additional patient needs beyond self-management support programs. Thus, nurses also referred patients to other outpatient clinical resources, such as services provided by a nurse case manager, social worker, or clinical pharmacy specialist. These referrals, when accepted, were also recorded in the Navigator system. In this article, we included referrals to self-management programs and to clinical services, both of which represent different types of care management activities.
Upon acceptance of a referral, the Navigator nurse submitted the appropriate information to the relevant program or clinical staff, who later contacted the patient to engage them in care. A follow-up Navigator phone call with the patient ensured that contact with these resources had been made and addressed any additional needs at that time.
Sample
The Navigator was first pilot tested with patients with diabetes. Thus, our sample consisted of Veteran patients with high-risk diabetes who received the majority of their primary care from the main VAAAHS campus or an affiliated community-based satellite site. The VAAAHS provides care to more than 60,000 Veterans and delivers more than 500,000 outpatient visits annually. Using a population-based registry, we identified patients with a recorded International Classification of Diseases, Ninth Revision (ICD-9) diagnosis of diabetes and at least two primary care visits to one of the VAAAHS sites within the previous year. High-risk diabetes criteria included at least one of the following: a history of amputation; last A1c >9 or last A1c >8 and age ⩽55 years; last recorded systolic blood pressure >160 and/or last recorded diastolic blood pressure >100; presence of diabetic ulcer; and/or insulin usage. Patients who met the defined high-risk criteria were considered eligible for the Navigator program and were entered into the Navigator tool for assessment by the RN.
Data collection and measures
We obtained patient information available from the Navigator as well as patient self-reported information collected by the RN during the initial Navigator assessment. These data included patient demographics (gender, age as of date of assessment, and living arrangement), the high-risk diabetes criteria mentioned above, and the number of primary care visits for each patient within the past year. Additionally, the Navigator assessment included several Likert items that asked patients to rate or score their interest and preferences for care delivery and perceptions of quality of life, health status, depression symptoms, confidence in self-care, and pain. The Navigator assessment tool was specifically developed for program purposes to identify important patient factors that are relevant to the VHA self-care programs that are offered. The assessment questions were previously tested, and a description of the development of the assessment tool is provided elsewhere. 12 In general, the assessment items were adopted from established survey instruments, including the Short Form-12 (SF-12®) Health Survey, 30 the Vulnerable Elders Survey (VES-13), 31 the Patient Health Questionnare-2 (PHQ-2), 32 the Brief Pain Inventory (BPI), 33 and the Chronic Disease Self-Efficacy scales developed by Lorig et al. 34
Our primary outcome was whether the patient accepted or declined referral at the time of the initial assessment. Information on the number and type of referrals made by the RN was collected and stratified into two groups according to whether the applicable program was one that focused specifically on developing and/or increasing patient self-management strategies versus one that provided clinical services to the patient. Referral information was only documented for patients who indicated they were interested in receiving the referral. Thus, information for referrals that were offered but declined by patients was missing for most patients. This prevented analysis of the likelihood of accepting referrals as potentially influenced by the type of referral (i.e. clinical service versus self-care program). Therefore, patients were classified as accepting a referral when one or more referrals were documented as accepted by the Navigator nurse, while patients who declined all referrals were classified as declining referrals. Many of these programs do not routinely collect enrollment data in a standardized format (i.e. not in the electronic medical record system), and thus, we were unable to determine participation rates for the various programs. As such, our intention here was to explore patients’ receptiveness to an offer of services as an initial step in the care management continuum.
Data analysis
Due to low frequencies for some response categories for several of the assessment questions, we collapsed their Likert-type scales into fewer categories for analysis in order to provide meaningful groups. For example, the five response levels for quality of life and general health were grouped into three values of excellent or very good, good, and fair or poor. The two highest response values of “more than half the days” and “nearly every day” were combined into one category for two questions related to feeling depressed and having little interest in doing things. On further examination of the data, we found that the three questions pertaining to patients’ self-efficacy in managing health were highly skewed, with the majority of patients reporting the highest confidence level (10 on a 1–10 scale) for each. Thus, binary categories indicating very high (9–10) and less than high (1–8) were created. The 0–10 response levels for the four questions relating to pain were grouped into none to very little pain (0–1), small amount (2–4), moderate amount (5–7), and very much (8–10). However, a large proportion of patients reported no pain for two of these questions (pain in the previous week and previous 4 weeks). Thus, we compared those with no pain to those reporting some pain for these two questions.
For our analysis, we grouped patients as having accepted or declined a program referral. Chi-square tests were used to assess whether the characteristics of patients differed between those who accepted and those who declined. Due to the non-normal distributions of age at assessment and the number of primary care visits in the previous year, we compared differences in these variables between the accepted and the declined groups via Wilcoxon rank-sum tests.
In multivariate analysis, we performed logistic regression which modeled referral acceptance as the outcome. Model development consisted of an iterative process to select variables, informed by results from the bivariate analyses, as well as conceptual clarity. For example, although the level of pain during the past week and the level of pain over the past 4 weeks were both significantly associated with referral acceptance, they were highly correlated (Spearman correlation = 0.83, p < 0.0001). Thus, only the level of pain over the past 4 weeks was included in the models. Variables with a 0–10 or 1–10 scale were treated as continuous variables. The odds ratios comparing those who accepted referrals versus those who declined are reported. All statistical tests were performed with a significance level of p < 0 0.05. All analyses were conducted using SAS version 9.3 (SAS Institute Inc., Cary, NC).
The Navigator program was developed for clinic operations and implemented as usual care. Program and administrative data were analyzed for quality improvement purposes. All VHA authors of this article attest that the activities that resulted in producing this article were not conducted as part of a research study, but as part of a non-research evaluation under the authority of VHA operations. Thus, institutional review board approval was not required.
Results
We identified all available high-risk patients who completed a Navigator assessment with an RN between December 2010 and January 2013 (n = 541). Documentation of an acceptance or declination of a referral was available for 425 patients (79%). Patients with a missing referral status were more likely to be affiliated with the satellite site than the medical center-based primary care site as compared to those with a referral status (46% versus 11%, p < 0.001). However, we suspected this difference was likely due to new nurses still being trained in using the Navigator. In further examination, there were no significant differences between those with a missing referral status (n = 116) and those with a documented referral status with respect to gender, age, living arrangement, number of primary care visits in previous year, and proportions identified with the high-risk conditions of diabetic ulcer, amputation, high blood pressure, and insulin usage. However, those with a missing referral status were more likely to have been identified with a high A1c than those with a referral status (44% versus 30%, p = 0.005). We further examined other variables of interest and found no further differences between the two groups. We excluded from analyses those with missing documentation of a referral acceptance or declination.
The majority of patients were male, older, lived with a spouse or other adult(s), and received most of their care at the main medical center-based primary care site (Table 1). These characteristics did not differ significantly between the two groups. However, a patient accepting a referral had more primary care visits in the previous year than those declining a referral (mean 5.1 versus 4.4, p = 0.02). Additionally, those who accepted a referral were less likely to have been identified with high blood pressure (27% versus 40%, p = 0.01) and more likely to have been identified as using insulin (70% versus 58%, p = 0.01) than those who declined.
Characteristics among patients who completed a Navigator assessment, December 2010–January 2013.
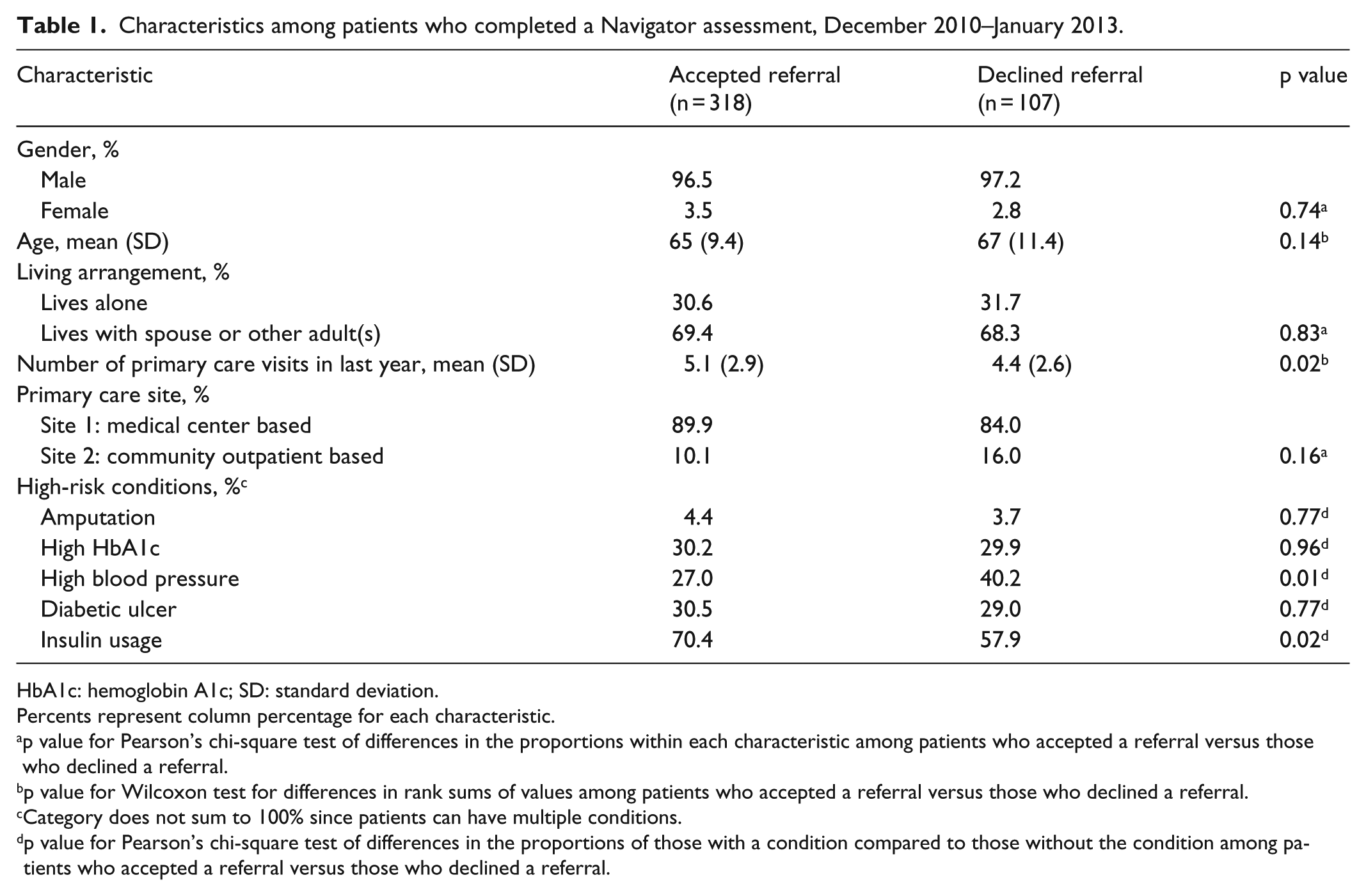
HbA1c: hemoglobin A1c; SD: standard deviation.
Percents represent column percentage for each characteristic.
p value for Pearson’s chi-square test of differences in the proportions within each characteristic among patients who accepted a referral versus those who declined a referral.
p value for Wilcoxon test for differences in rank sums of values among patients who accepted a referral versus those who declined a referral.
Category does not sum to 100% since patients can have multiple conditions.
p value for Pearson’s chi-square test of differences in the proportions of those with a condition compared to those without the condition among patients who accepted a referral versus those who declined a referral.
In total, the 318 patients (75%) who accepted a Navigator referral received 583 referrals to programs offered by the VAAAHS. Fifty-two percent of the referrals were to self-care programs, including MyHealtheVet (an online personal health record, n = 82), home telehealth (n = 71), MOVE and TeleMOVE (VHA weight loss programs, n = 50 and n = 41, respectively), CarePartners (a VAAAHS program involving informal caregivers, n = 34), diabetes education (n = 23), and tobacco cessation classes (n = 4). The clinical service referrals (47%) included a variety of services such as RN case management (n = 104), social work (n = 87), PCP (n = 31, made when there was a new or exacerbated medical issue), clinical pharmacist (n = 13), geriatrics (n = 12), home-based primary care (n = 9), and others (n = 20). Among 318 patients who accepted a Navigator referral, 33% received referral(s) only to self-care programs, 29% received referral(s) only for clinical services, and 38% received referrals to both self-care programs and clinical services. Because the type of referral offered is typically not documented for patients who decline referral, we were unable to determine whether the type of referral was associated with patients’ willingness to accept referral(s).
Patients who accepted a referral were more likely to be currently enrolled in another program as compared to those who declined a referral (18% versus 6%, p < 0.01; Table 2). In fact, among the 63 patients who were enrolled in other programs, 90% accepted a referral. Additionally, patients who accepted a referral were significantly more likely to report being interested in traveling to the VHA site for programs (44% versus 29%), comfortable using the phone (88% versus 76%), interested in phone-based programs (48% versus 18%), interested in programs using family or friend support (26% versus 4%), and having a computer that he or she uses regularly (59% versus 41%) compared to those who declined.
Percentage of patients with select characteristics among those who completed a Navigator assessment, by referral status.
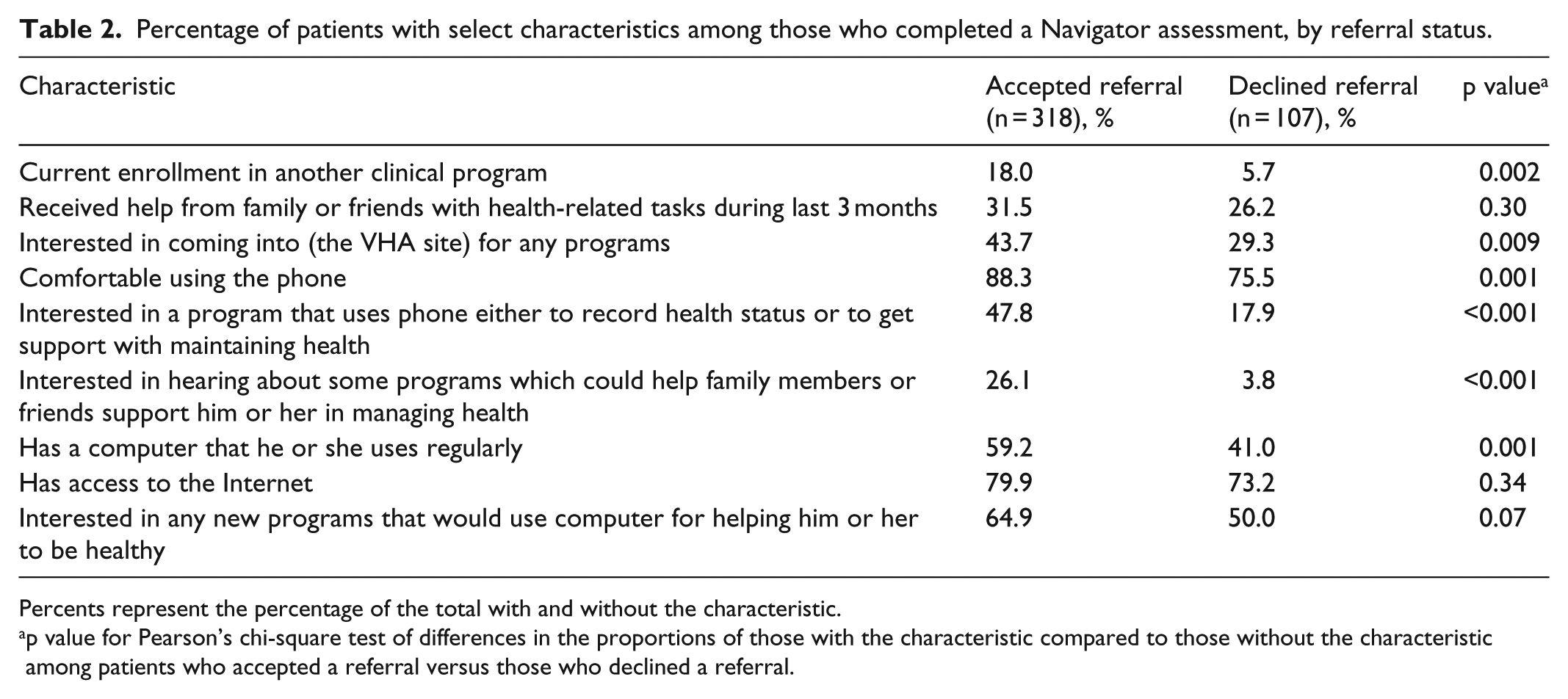
Percents represent the percentage of the total with and without the characteristic.
p value for Pearson’s chi-square test of differences in the proportions of those with the characteristic compared to those without the characteristic among patients who accepted a referral versus those who declined a referral.
There were no significant differences between the two groups in self-reported quality of life, general health, and feelings of depression (Table 3). However, those who accepted a referral tended to report having little interest or pleasure doing things in the previous 2 weeks more often than those who declined a referral (p = 0.05). Although patients in both groups reported very high levels of self-efficacy in managing their health, a significantly larger proportion of those who declined a referral rated their confidence higher than those who accepted a referral in two out of the three confidence questions.
Patient perceptions of quality of life, health, and self-efficacy among those who completed a Navigator assessment, by referral status.

Percents represent column percentage for each characteristic.
p value for Pearson’s chi-square test of differences in the proportions within each characteristic among patients who accepted a referral versus those who declined a referral.
Significantly more patients who accepted a referral reported the presence of pain during the past week (83% versus 63%, p < 0.001) and over the past 4 weeks (85% versus 66%, p < 0.001) as compared to those who declined (Table 4). There were no differences between the groups with respect to pain interfering with enjoyment of life or general activity.
Patient perceptions of pain among those who completed a Navigator assessment, by referral status.

Percents represent column percentage for each characteristic.
p value for Pearson’s chi-square test of differences in the proportions within each characteristic among patients who accepted a referral versus those who declined a referral.
In multivariate analyses, the level of pain over the past 4 weeks, current enrollment in another clinical program, interest in programs utilizing phone and family, and quality of life during the past week were all significantly associated with referral acceptance (Table 5). For example, for each one-unit increase in pain level, the odds of accepting a referral increase by 7.8%. Patients who were currently enrolled in a clinical program and patients who reported interest in programs using phone or family for support were three to four times more likely to accept a referral than those without these characteristics. Conversely, reporting an excellent or very good quality of life was associated with decreased odds of accepting a referral.
Estimates from logistic regression modeling the probability of referral acceptance among Navigator patients (n = 406).

Logistic regression likelihood ratio chi-square = 74.61 (13 degrees of freedom), p < 0.0001. Estimates that are significant with p < 0.05 are in bold.
Discussion
The Navigator tool was developed to help match patients’ preferences for care to available self-management programs as a part of PACT implementation. This project sought to better understand what patient characteristics may predict acceptance of a program referral using the Navigator tool. This is the first step in understanding the types of patients who are more willing to be engaged in their health care. We identified several key patient characteristics associated with acceptance of referrals in this population. In general, patients accepting referrals had more primary care visits in the previous year, were more likely to be enrolled in another program, expressed more interest in various types of care programs, were slightly less confident in managing health, and were more likely to report pain as compared to those who declined a referral. In consideration of all these factors, previous program enrollment and interest in programs were most strongly associated with referral acceptance. This suggests that patients’ preferences and previous participation in care are just as important as measures of their health status in determining their willingness to seek self-care assistance.
We found that just over half of the referrals (52%) were to self-management programs. In fact, many of the patients contacted were in need of something other than self-management support, for example, a referral to social work, RN case management, their PCP, or to the clinical pharmacist for a prescription refill or medication reconciliation. Anecdotally, the Navigator RNs reported that regardless of the referral destination, the Navigator calls seemed to help patients get on track with their health management and enabled participation in self-management programs. It also helped RNs to recognize their important role in care coordination within the PACT model of care.
Our results also demonstrated that the presence of pain was associated with higher likelihood of accepting a referral. In a previous study, researchers identified pain as a barrier to participation in self-management activities for patients with chronic disease. 26 The juxtaposition of pain as a potential activator for seeking care while simultaneously impeding self-care efforts has important implications not only for engaging these patients in self-care activities but also in keeping them engaged for the long term. It also stresses the importance of addressing health issues, such as pain, that may not be directly related to chronic disease management, yet may influence patients’ interest in and the ability to participate in chronic disease self-care programs.
Three-quarters of patients for whom we had a referral status accepted a referral, possibly indicating a high interest and willingness of patients to seek and obtain care outside of the usual medical care they receive from providers. Moreover, the high acceptance rate may also indicate the success of the Navigator in linking patients to programs via referrals that may not have otherwise been received by patients. Past research has shown providers’ referral practices to self-management programs to be low 27 and that some health care providers act as the gatekeeper to supplemental programs, such as telehealth.35,36 Providers’ willingness to refer patients to programs is affected by multiple factors, including fear of fragmenting care or increasing workload, concerns about the amount of time necessary to motivate patients, and uncertainty as to which patients would benefit most. 28 Utilizing a primary care RN, an algorithm identifying high-risk patients, strong reliance on RN’s clinical judgment, and an assessment that matches patient preferences to available programs, the Navigator may help address barriers to provider referrals. Further strategies may be needed, however, for patients who appear to be less connected to health resources and may, to some degree, be more in need of care provided by these types of programs.
We recognize limitations to our project findings. First, our results are from a large, academically affiliated VA health care system, therefore may not be generalizable to smaller, non-academically affiliated VAs or non-VA medical facilities or practices. Also, the population only included those patients with diabetes who were considered high risk using criteria developed by the PACT Demonstration Laboratory, thus the findings may vary for patients with other chronic conditions. This work should be expanded to explore patient characteristics and preferences of those with other chronic conditions, such as heart disease. Additionally, we had missing referral acceptance/declination information for 21% of our sample, which potentially may have affected our results. Suggested referrals are typically not recorded for patients who declined referrals; thus, we were unable to determine whether the likelihood of referral acceptance was different for those receiving referrals for clinical services versus those receiving referrals for self-care programs.
Finally, we were unable to determine patients’ participation in programs, as this information was not readily available for some programs. Although program participation is a key outcome for care management interventions, understanding factors that may increase the likelihood of patient participation is also important. Without an initial receptiveness or willingness to consider available services, participation may not occur. Thus, further exploration of patients’ initial contact with care management resources may provide valuable information that can help guide outreach efforts and ultimately increase program participation.
Conclusion
The Navigator system was designed to promote key provisions of the medical home model of care in VAAAHS. PACT principles include patient-centeredness, which is included in the Navigator system by matching patients’ goals and preferences to a variety of resources. Use of the Navigator increases patients’ and providers’ knowledge of available programs and promotes patient ownership and decision making in their care. Importantly, the Navigator promotes nurse-driven care management and care coordination, expanding the roles of primary care nurses, which is a key objective of PACT. A better understanding of the characteristics associated with acceptance of a program referral allows providers and/or RNs to strategically and proactively contact patients who may need and be open to additional care, as well as develop new programs to match patients’ needs. These efforts may lead to a more knowledgeable and engaged patient population with chronic disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Evaluation of the Navigator program was deemed non-research operations (i.e. not research) by the Veterans Health Affairs Office of Research Oversight. Formal attestations of only non-research activities regarding this project and article were obtained and documented in official records from all VHA-employed co-authors and their supervisors and the VHA Director of Primary Care Services.
Funding
This work and the VAAAHS PACT Demonstration Laboratory were supported by the Office of Primary Care, Veterans Health Administration, Department of Veterans Affairs. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Informed consent
The Navigator program was deemed non-research operational activity (see above) and thus did not require informed consent from participants.