
Abstract
Objectives:
This study aims at identifying profiles of mental health professionals based on individual, interactional, structural and professional role characteristics related to interprofessional collaboration.
Methods:
Mental health professionals (N = 315) working in primary health care and specialized mental health teams in four Quebec local service networks completed a self-administered questionnaire eliciting information on individual, interactional, structural and professional role characteristics.
Results:
Cluster analysis identified four profiles of mental health professionals. Those with the highest interprofessional collaboration scores comprised two profiles labeled “highly collaborative female professionals with fewer conflicts and more knowledge sharing and integration” and “highly collaborative male professionals with fewer conflicts, more participation in decision-making and mutual trust.” By contrast, the profile labeled “slightly collaborative professionals with high seniority, many conflicts and less knowledge integration and mutual trust” had the lowest interprofessional collaboration score. Another profile positioned between these groups was identified as “moderately collaborative female psychosocial professionals with less participation in decision-making.”
Discussion and conclusion:
Organizational support, participation in decision-making, knowledge sharing, knowledge integration, mutual trust, affective commitment toward the team, professional diversity and belief in the benefits of interdisciplinary collaboration were features associated with profiles where perceived interprofessional collaboration was higher. These team qualities should be strongly encouraged by mental health managers for improving interprofessional collaboration. Training is also needed to promote improvement in interprofessional collaboration competencies.
Keywords
Introduction
Interprofessional collaboration (IPC) has benefits for patients, mental health (MH) professionals, health care organizations and health systems alike.1,2 Good collaboration among mental health professionals (MHPs) has been found to reduce clinical errors, improve patient health status and enhance the quality of patient care, while leading to better patient treatment compliance and enhanced satisfaction.2–4 IPC also increases work satisfaction and motivation among professionals, while reducing tensions and promoting problem solving in health care teams.1,5,6 IPC is known to reduce duplication of services, fragmentation of care and staff turnover while favoring positive work environments.4,7 More globally, studies have confirmed that IPC reduces health care costs. 8
Despite the many benefits of IPC, research suggests that the uptake of IPC in health care teams is limited.1,2,9 Yet, failure to work collaboratively is associated with greater team conflict, medication errors, duplication of services, longer patient hospitalization and higher mortality rates.3,10 In order to develop and implement interventions that promote IPC, factors that may influence IPC need to be identified. Few studies along these lines have been undertaken,11–13 and what this research tends to overlook is the heterogeneity among MHPs, whose sociodemographic, professional, cultural and economic characteristics vary considerably.14–16 A better understanding of similarities and differences among MHPs based on IPC would permit the development of appropriate interventions to enhance IPC as well as approaches appropriate to identified subgroups.17,18 Professional profiles producing a variety of psychosocial and clinical outcomes have been generated in fields outside MH. 19 Nonetheless, studies differentiating MHPs according to IPC remain limited. Little is known about whether profiles of MHPs may be distinguished according to perceived IPC. Cluster analysis methods might be applied to this task. 19 Indeed, unlike other quantitative methods such as multiple regression, cluster analysis may reveal relationships between variables as well as previously unidentified group structures. 17
Based on the Bronstein 20 model and published works of San Martin Rodriguez et al. 21 and Mulvale et al., 13 independent variables related to IPC may be classified into four conceptual blocks: Individual characteristics (e.g. sociodemographic variables), Interactional variables (related to interpersonal relationships), Structural variables (related to the organization) and Professional role characteristics (related to professional practice). 20
Concerning Individual characteristics, a positive association was identified between seniority in the team and IPC22,23 as well as belief in the benefits of interdisciplinary collaboration and IPC.24,25 Sarma et al. 23 found that female physicians collaborated more with nurses, whereas male physicians collaborated more with specialists. Elsewhere, Jehn et al. 26 and Pelled 27 reported a positive relationship between gender diversity and relationship conflict, whereas Williams and O’Reilly 28 showed no effect of gender diversity on conflict among group members. Regarding Interactional variables, studies identified participation in decision-making as a key element of IPC in health teams.29,30 Participation in decision-making has been associated with lower rates of risk-adjusted mortality among patients and higher levels of job satisfaction among professionals. 31 It serves also to develop a better analysis and evaluation of all possible solutions.32,33 Poor decision-making processes have been shown to contribute to the occurrence of critical incidents. 34 Other studies have shown that affective commitment toward the team promotes knowledge sharing, 35 increases mutual trust 36 and reduces team conflict, 37 all essential conditions for IPC.37,38 Team conflict increases the level of stress and anxiety, limits the cognitive abilities of team members and decreases team performance.27,39,40 Studies have also found positive associations between knowledge integration and IPC.21,41 The integration of expertise and skills from several disciplines is particularly important for the biopsychosocial management of complex cases such as mental disorders. 42 Organizational support, a prevalent Structural characteristic in IPC studies, was also found to be positively related to IPC,24,43 with direct impact on staff turnover, 44 job satisfaction and performance. 45 Finally, type of profession is a frequently studied role characteristic in relation to IPC. The values and cultures of some health professions strongly support IPC, 46 while others may become sources of team conflict, reducing IPC effectiveness.47,48
While a growing body of literature has identified variables that may influence IPC, only limited research has involved the profiling of professionals in terms of perceived IPC on their teams, particularly in the MH field. To the best of our knowledge, no study has created a typology of MHPs working in MH teams, operating in local service networks (LSNs), whether in primary health care (PHC) or specialized MH services. Cluster analysis has never been used to generate profiles of MHPs working within interdisciplinary teams based on perceived IPC. Yet, this method has the potential to provide a multidimensional portrait of health care professionals that might better inform health care management. This study intended to fill these gaps by identifying profiles of (MH) professionals in relation to their perceived IPC and taking into account multiple independent variables describing practices of MHPs as well as their hypothesized relationship with IPC based on the literature.13,20,21 By linking different variables that may influence IPC, findings may provide a better understanding of IPC, while also improving the detection of (MH) professionals at risk for lesser collaboration, with a view toward maximizing IPC.
Methods
Study design and sample
This study emanated from a larger evaluation of health services network implementation in the context of the 2005–2015 reform of the Quebec MH system. 49 This major reform aimed in part at consolidating frontline services, setting up MH interdisciplinary teams and promoting service delivery based on IPC.50,51 Interdisciplinary MH teams typically include psychiatrists, nurses, psychologists, social workers, psycho-educators and administrative support professionals. 51
The study was cross-sectional, including MHPs from four Quebec LSNs, which consist of organizations and professionals providing health and social services to territorial populations. 50 Four LSNs were identified in consultation with a research advisory committee composed of 20 Quebec MH decision makers (e.g. the Ministerial MH director, regional MH coordinators and a representative of the Quebec Psychiatric Association) who completed a survey. The networks were selected based on geographic diversity (urban or semi-urban areas), population (range from 135,000 to 300,000 inhabitants) and services offered (e.g. presence or absence of a public psychiatric hospital). Selected LSNs were divided into two broad groupings: LSNs located in densely populated urban areas, with specialized psychiatric services (N = 3), and an LSN located in a less populated, semi-urban area, without psychiatric services (N = 1).
To qualify for the study, MHPs had to be working in one of the four selected LSNs, as a member of a specialized MH team or PHC team with at least three professionals representing two or more disciplines. A list of all eligible MHPs was provided by the advisory committee. All potential study participants were invited by email or telephone to participate. Presentations by researchers were also organized in various organizations to inform, and recruit, potential participants.
Data collection and variables
Analysis of variance (ANOVA) was used to calculate the sample size; at α equal to 0.05 with 80% power, a minimum of 200 MHPs were needed to detect the different among groups of the dependent variable (IPC). A total of 315 MHPs working in 79 MH teams (31 PHC teams and 48 specialized MH teams) participated in the study, for a 68% response rate. They responded to a self-administered questionnaire mailed between May 2013 and November 2014. The questionnaire, which took 45 min to complete, included sociodemographic information and standardized scales on diverse aspects of teamwork.
Table 1 describes the instruments used in the study according to categories of variables. The main variable of interest (IPC) was measured with the Team Collaboration Questionnaire, which is a validated instrument with rating on a seven-point Likert-type scale (1 = completely disagree; 7 = completely agree), and including four sub-dimensions: team communication, synchronization, explicit coordination and implicit coordination. Cronbach’s alpha for the different dimensions varies from 0.77 to 0.91.
Variables and instruments used in the study.
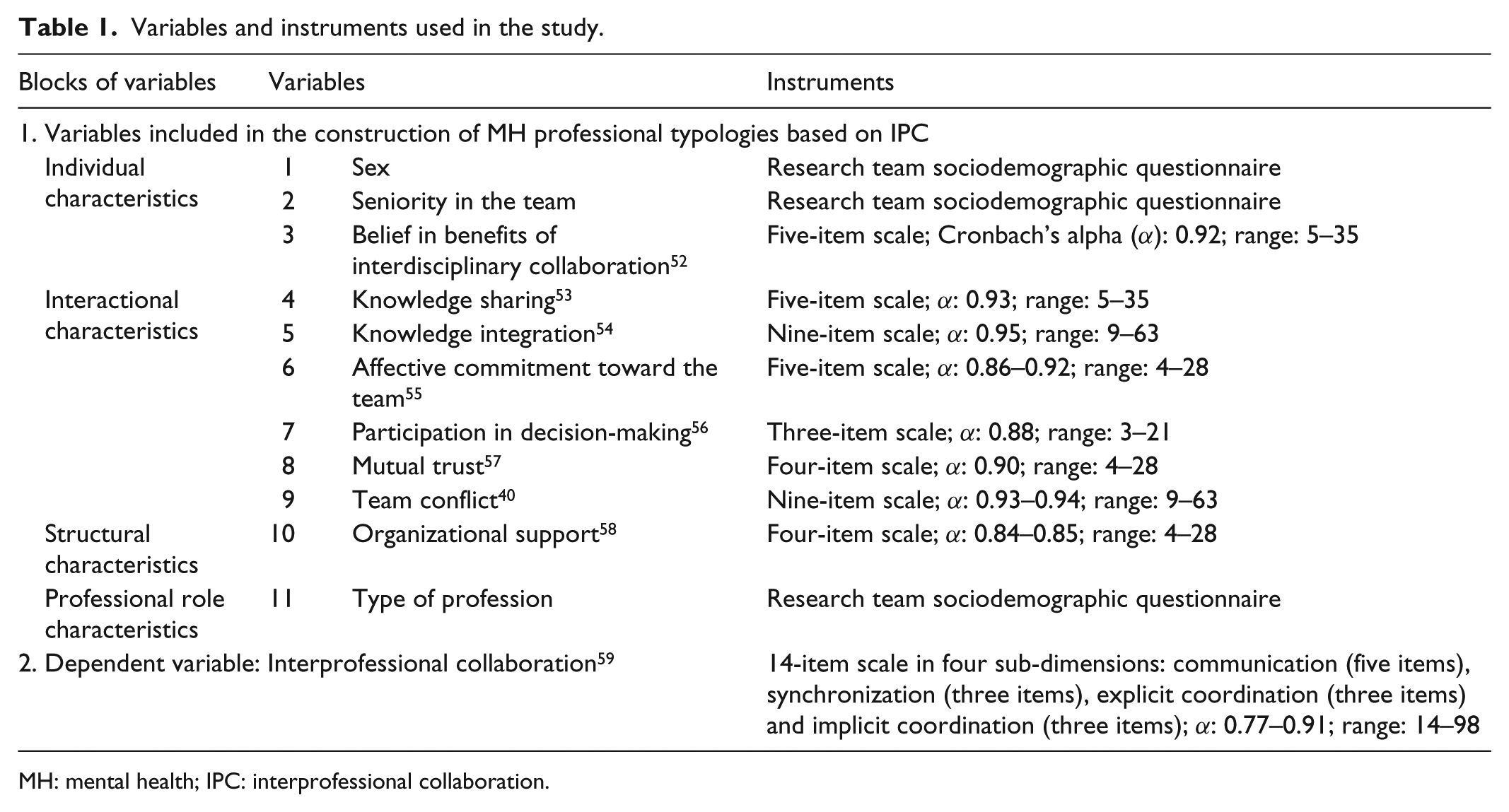
MH: mental health; IPC: interprofessional collaboration.
Based on the interdisciplinary collaboration framework cited above, the pertinent variables were organized under four key dimensions: (1) Individual characteristics (three variables), (2) Interactional characteristics (six variables), (3) Structural characteristics (one variable) and (4) Professional role characteristics (one variable). All variables related to Interactional characteristics, one variable related to Individual characteristics (belief in the benefits of interdisciplinary collaboration) and the variable on Structural characteristics (organizational support) were measured with validated scales (see Table 1) using seven-point Likert-type scales (1 = completely disagree; 7 = completely agree). The variable measuring Professional role characteristics (type of profession) was categorized as medical (e.g. specialist, general practitioner, nurse, pharmacist), psychosocial (e.g. social worker, psychologist) and administrative support professional (e.g. technician, clerk).
Analyses
After scrutinizing the database for outliers and missing values, univariate analyses were performed. Missing data were less than 5% per variable and were replaced using a multiple imputation technique. Univariate analyses were analyzed using frequency distributions (number and percentage) for categorical variables and central tendency distributions (mean values and standard deviations (SDs)) for continuous variables. MHP profiles were calculated using two-step cluster analysis with SPSS 21®. IPC was the variable of interest, as defined above. Individual characteristics were organized as continuous and categorical variables before introduction into the model. Categorical variables were entered first, followed by continuous variables. The log-likelihood method was used to determine intersubject distance. Participant classifications were performed using Schwartz Bayesian criteria and the final number of profiles was set at 4, according to their overall contribution to interclass homogeneity. An ANOVA was then performed to test whether differences among profiles on IPC scores were statistically significant, followed by post hoc tests using the Bonferroni correction.
Results
Sample
No differences were found between participants (N = 315) and non-participants (N = 151) with respect to distributions for team type (χ2(1, N = 466) = 0.79; p = 0.68) and gender (χ2(1, N = 466) = 0.03; p = 0.87). Mean age of participants was 43 years (SD = 10.5). Mean seniority on teams was 3 years (SD = 4.62). Most participants were psychosocial professionals (54.6%), and the rest were medical professionals (34.6%) or administrative support professionals (10.8%). Women were more prevalent than men (70% vs 30%). Most professionals worked in outpatient specialized health care (56%), a third in PHC (32%) and fewer in specialized inpatient health care (12%). Participant characteristics are presented in Table 2.
Characteristics of participating mental health professionals (N = 315).

SD: standard deviation.
Mean score (1–7 for each variable); min: 1, max: 7; higher = positive.
Mean score (1–7 for 19 variables); min: 1, max: 7; lower = positive.
MHP profiles based on IPC
Four profiles were identified (Table 3), with subsample sizes ranging from 112 (36%) in Profile 4 to 63 (20%) in Profile 2. Profile 1 included 63 participants (21%), while Profile 3 included 75 participants (24%). An ANOVA comparing IPC scores among the four profiles revealed significant differences: F(4, 310) = 24.47, p < 0.001. Post hoc tests using the Bonferroni correction revealed that perceived IPC among MHPs in Profile 1 (M = 16.09, SD = 3.27) was significantly lower than those in other profiles (p < 0.001). There were no significant differences between Profiles 3 (M = 20.69, SD = 3.16) and 4 (M = 21.56, SD = 2.83); both had significantly higher scores than Profile 2 (M = 17.04, SD = 3.17; p < 0.05) and Profile 1 (p < 0.001). The perceived IPC score for Profile 2 (M = 17.04, SD = 3.17) was significantly higher than that for Profile 1 (p < 0.001).
Cluster analysis of mental health (MH) professionals based on interprofessional collaboration (IPC).

SD: standard deviation.
Profile 4 had the highest IPC score and consisted entirely of women. While all types of professions were represented, this group had the most medical professionals (41%), compared with other profiles. Profile 4 also had the highest scores for belief in the benefits of interdisciplinary collaboration, affective commitment toward the team, knowledge sharing, knowledge integration and organizational support and the lowest score on team conflict. We labeled this cluster “highly collaborative female professionals with fewer conflicts and more knowledge sharing and integration.”
Profile 3 also had a high IPC score not significantly different than Profile 4 and consisted exclusively of men from predominantly medical and psychosocial professions. Profile 3 individuals had the highest scores on participation in decision-making and on mutual trust, as well as the second highest scores on belief in the benefits of interdisciplinary collaboration, affective commitment toward the team, organizational support and knowledge integration. Profile 3 was labeled “highly collaborative male professionals with fewer conflicts and more participation in decision-making and mutual trust.”
Profile 1 had the lowest IPC score. This subgroup included disproportionately more individuals with high seniority in their teams. All professions were represented, but mostly medical professionals. The percentages of psychosocial professionals (9%) were low relative to other groups, whereas the percentages of support professionals (63%) were higher. Profile 1 individuals had the lowest scores on affective commitment toward the team, mutual trust, knowledge integration and organizational support and the highest score on team conflict. Profile 1 was labeled “slightly collaborative professionals with high seniority, many conflicts and less knowledge integration and mutual trust.”
Profile 2 presented a moderate IPC score and included female psychosocial MHPs exclusively with the least seniority compared with those in other profiles. Scores on belief in benefits of interdisciplinary collaboration and participation in decision-making were lowest. Otherwise, this profile came third on almost all variables in the Interactional and Structural characteristics dimensions. Profile 2 was labeled “moderately collaborative female psychosocial professionals with less participation in decision-making.”
Discussion
This study developed a typology of MHPs, taking multiple independent variables into account. Variables describing the practices of MHPs were selected, as well as those with hypothesized relationships to IPC based on the literature.13,20,21 Four profiles of MHPs emerged using cluster analysis, two groups of highly collaborative professionals and two groups of moderately or slightly collaborative professionals. A better understanding of MHP profiles that facilitate or impede IPC may contribute to enhancements in service planning. Health team members who collaborate effectively and perceive themselves as high performing also take more initiatives to improve patient care.60,61
Results of the study demonstrate that “highly collaborative female professionals” (Profile 4) and “highly collaborative male professionals” (Profile 3) had the best overall scores on variables in the Individual, Interactional and Structural characteristic dimensions and the lowest score on team conflict. These findings are consistent with previous studies showing that high-functioning health care teams enjoyed elevated scores on belief in benefits of interdisciplinary collaboration, participation in decision-making, affective commitment toward the team, mutual trust, knowledge sharing, knowledge integration, organizational support and low levels of team conflict.12,62 These two profiles included a mix of professionals, about one third each of medical, psychosocial and support professionals. The difference between these two profiles was the sharp division along gender lines: Profile 4 consisted entirely of women, while Profile 3 consisted exclusively of men. Conversely, the profile with lower IPC and higher conflict (Profile 1) was the only one composed of both men and women. This finding is consistent with previous studies showing that gender diversity decreased communication 63 and cooperation among team members 64 while increasing relationship conflict26,27,65 and lack of cohesion. 66 However, the typical stereotypes about how men and women perform in groups and relate to each other were not reflected in these results.67,68
As opposed to Profiles 3 and 4, consisting of IPC “champions,” the group with the poorest IPC score (Profile 1) had the worst scores on five of the six Individual characteristics, namely, affective commitment toward the team, mutual trust, knowledge sharing, knowledge integration and the highest score on team conflict, as well as the lowest score on organizational support (Structural characteristics). Profile 1 also had the second worst score on participation in decision-making (Interactional characteristics) and on belief in benefits of interdisciplinary collaboration (Individual characteristics). The main difference between Profiles 1, 3 and 4 was in the proportion of support professionals, which was higher in Profile 1. It may be that support professionals felt less integrated in their teams than members of medical or psychosocial professions. Furthermore, Profile 1 included individuals with higher seniority. Here, the low results were not consistent with other research identifying seniority on the team as positively related to IPC.2,3,22 A possible explanation for this may be that older members of medical professions, the majority in Profile 1, tended to work more in silo. By contrast, newer professionals in the other teams would have had less work experience, leading them to perhaps collaborate more readily with others. Better collaboration and understanding may also reduce the risk of error among less experienced professionals. 69
Profile 2 (moderately collaborative female psychosocial professionals) had the lowest scores on belief in benefits of interdisciplinary collaboration and on participation in decision-making, which suggests a particular challenge in the context of the recent MH reform in Quebec.70,71 Indeed, effective interventions in MH care need to take into account increasingly the biopsychosocial needs of patients. 39 This implies close collaboration among professionals working in MH teams. Furthermore, the increasing incidence and prevalence of comorbidity between mental disorders and chronic physical illnesses (e.g. cancer, stroke, diabetes and acute coronary syndrome) as well as MH/addiction comorbidity require greater IPC among psychiatrists, general practitioners, nurses, psychologists, social workers and other MHPs. 72 Research demonstrates the value of psychology and psychosocial services in lowering risk factors for many diseases. 73 As opposed to Profiles 4 and 3, Profile 2 consisted entirely of psychosocial professionals. Psychiatrists and other MH medical professionals have been working for a long time in a biopsychosocial mode and on teams, 49 whereas psychologists social workers and others most often worked in silo prior to the creation of multidisciplinary MH teams under the Quebec MH reform. 74 Moreover, the role of social workers in MH teams is not always well defined, which puts them at a disadvantage 75 and exposes them to additional stress. 76
Profiles 1 and 2 had the highest scores on team conflict, viewed as a major obstacle to IPC even while some conflict is inevitable.13,77 Identifying and addressing sources of conflict is crucial in MH, where demands and expectations are very high for managing cases of complex mental disorders. Indeed, while effective MH care depends on the contributions of several disciplines, conflict can hinder team functioning, decrease effectiveness and impact patient care. 78 Furthermore, constraints on the clinical decision-making process pose a particular threat to positive team performance, as does lack of knowledge sharing and knowledge integration among disciplines.21,41 Such Interactional characteristics are especially important in MH teams staffed by multidisciplinary professionals. 79
Caricati et al. 80 and Bookey-Bassett et al. 24 have shown that, without a high sense of affective commitment toward the team and mutual trust, both higher in Profiles 4 and 3, but lower in Profiles 1 and 2, collaboration among team members rarely succeeds. Affective commitment toward the team is also associated with professional well-being and job satisfaction,81,82 whereas mutual trust is associated with high job performance, organizational citizenship behaviors, organizational commitment, job satisfaction and lower staff turnover. 83 Affective commitment toward the team and mutual trust are particularly important in MH due to the high incidence of crisis situations.
Regarding Structural characteristics, organizational support, higher in Profiles 4 and 3 than in Profiles 1 and 2, remains a key determinant of effective IPC in health teams.24,84 Organizational support includes multi-level leadership and resource provision in terms of time, funding, equipment and space to care effectively for patients. 84 Support at the organizational level is also critical to the adequate functioning of MH teams dealing with serious MDs, 85 while also empowering professionals psychologically 86 and enhancing productivity. 87 Finally, belief in benefits of interdisciplinary collaboration (Individual characteristics) is identified as the basic requirement for IPC. 25
Limitations
While this study has many strengths, certain limitations must also be acknowledged. First, the results of the study are based on self-report and are subject to common-method variance issues. The study used a cross-sectional design which precludes causal interpretations. Finally, the results may not be generalizable to jurisdictions with health care systems different from the Quebec system, or to professionals in fields outside MH.
Conclusion
This study empirically identified four profiles of MHPs based on their IPC scores. It is the first known study to present profiles for MHPs working in interdisciplinary teams using cluster analysis. The study included MHPs working in diverse LSNs and types of health care organizations, which is rare for studies of IPC in MH care. Two profiles (“highly collaborative female professionals with fewer conflicts and more knowledge sharing and integration” and “highly collaborative male professionals with fewer conflicts and more participation in decision-making and mutual trust”) had higher perceived IPC scores, whereas the two other profiles had lower scores. Overall, profiles with elevated IPC scored high on all variables related to Interactional, Structural and Individual characteristics. In this regard, the study highlights the relevance of focusing on participation in decision-making, knowledge sharing, mutual trust, team conflict, belief in benefits of interdisciplinary collaboration and knowledge integration for improving IPC in MH teams and for future service planning. Findings also confirm the value of team commitment, organizational support and professional diversity for strengthening IPC in the MH sector, while arguing for a biopsychosocial approach to mental health care. Here, MH managers have a significant role to play in implementing activities focused on strengthening IPC in MH teams. Managers should also remain alert to behavioral changes and signs of tension that may threaten effective IPC. Finally, more outreach and training are needed to improve and transfer interprofessional knowledge, IPC competencies and interdisciplinary values and skills among MHPs.
Footnotes
Acknowledgements
We are grateful for the support provided by Fonds de recherche du Quebec Santé and thank the individuals who participated in the research, including the advisory committee and network respondents, and the research team. We are especially grateful to Guy Grenier for his valuable advice and Judith Sabetti for the linguistic revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval for this study was obtained from the Research Ethics Board of the Douglas Mental Health University Institute (MP-IUSMD-11-037).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this research was provided by the Fonds de recherche du Quebec Santé (FRQS).
Informed consent
Informed consent was obtained from all participants, each of whom signed a consent form.