
Abstract
Objectives:
This study was aimed to assess the food hygiene practice and associated factors among food handlers working in food establishments during the COVID-19 pandemic in East Gojjam and West Gojjam Zones, North West Ethiopia.
Methods:
A facility-based cross-sectional study was conducted among 845 food handlers working in 423 selected food establishments of East and West Gojjam Zones from 22 September to 2 November 2020. The food handlers were categorized as a cooker and a waiter based on their responsibility. A data collection tool was adapted from the literature and validated by conducting a pre-test prior to the study. Binary logistic regression was done to identify the factors associated with food hygiene practice among food handlers.
Results:
The prevalence of poor food hygiene practices among food handlers working in food establishments was 51.2% (95% confidence interval = 47.8, 54.6%). Being both a cooker and waiter (adjusted odds ratio = 2.98; 95% confidence interval = 1.02, 8.66), availability of personal protective equipment (adjusted odds ratio = 2.67; 95% confidence interval = 1.75, 4.08), presence of pipe water in the kitchen (adjusted odds ratio = 2.73; 95% confidence interval = 1.84, 4.06), presence of a supervisor (adjusted odds ratio = 2.26; 95% confidence interval = 1.41, 3.62), and separate dressing room (adjusted odds ratio = 2.69; 95% confidence interval = 1.84, 3.93) were significantly associated with food hygiene practice among food handlers.
Conclusion:
The prevalence of poor food hygiene practices among food handlers working in food establishments during the COVID-19 pandemic was high. Therefore, improving food hygiene practice focusing on availing personal protective equipment, pipe water in the kitchen, and ensuring the presence of a supervisor as well as a separate dressing room in the food establishment is recommended.
Introduction
Food hygiene is a measure important to make sure the safety and suitability of food in any respect levels of the food chain. 1 Food becomes infected at any level of production and distribution. In addition, a big percentage of foodborne ailment incidents are because of foods improperly prepared or mishandled at home, in food establishments, or at markets. Food handlers need to properly recognize the jobs they should play, including adhering to the fundamental hygienic practices while buying, selling, and getting ready meals in order to protect their health and that of the broader community. 2 In Ethiopia, the magnitude of good food hygiene/safety practices among food handlers was ranged from 29.9% in Dire Dawa City 3 to 67.8% in Asosa town. 4
Unsafe food contains dangerous viruses, parasites, bacteria, or chemical substances, causes more than 200 diseases.1,2,5 Poor food hygiene practices result in an outbreak of foodborne diseases and threaten public health security globally. Due to this, it has got an international concern. 6 Globally, an estimated 600 million (almost 1 in 10 people) in the world became ill following consuming contaminated food, and 420,000 humans die each year, which accounts for the loss of 33 million healthy life years. 2
Currently, in addition to unsafe food, the world is facing a threat from the COVID-19 (Coronavirus Disease 2019) pandemic, which is caused by the Severe Acute Respiratory Syndrome Corona Virus-2 (SARS-CoV-2) virus. In response to the COVID-19 pandemic, World Health Organization recommends respiratory hygiene, physical distancing, and handwashing with water and soap or hand rub with alcohol/sanitizer, wearing Personal Protective Equipment (PPE) as the primary preventive measures. 7 Although there is no existing evidence that viruses that cause respiratory illnesses being transmitted via food or food packaging, it is imperative for the food establishments to ensure the implementation of personal hygiene measures and provide training on food hygiene principles in order to eliminate or reduce the risk of food surfaces and food packaging materials from becoming contaminated with the virus from food workers. These measures will prevent foodborne illnesses in addition to preventing the spreading of COVID-19 among workers, and maintain a healthy workforce.7,8 Thus, the food hygiene practice among food handlers working in food establishments was expected to be increased during the COVID-19 pandemic. However, there is no study conducted on food hygiene practice and associated factors among food handlers working in food establishments during the COVID-19 pandemic. Therefore, this study assessed the food hygiene practice and identified factors associated with food hygiene practice among food handlers working in food establishments during the COVID-19 pandemic. The findings of the study will be used as input for programmers and health professionals to arrange training on food hygiene practices for food handlers working in food establishments.
Materials and methods
Study area and period
The study was conducted in East and West Gojjam Zones of Amahara Regional State. East Gojjam and West Gojjam zones are found in North West of Ethiopia. There were a total of 39 Woredas in East Gojjam (21 Woredas) and West Gojjam Zones (18 Woredas). In addition, there were an estimated 1616 and 1676 food and drink establishments in East Gojjam and West Gojjam Zones, respectively. The study was conducted from 22 September to 2 November 2020.
Study design and population
A facility-based cross-sectional study was employed among food handlers. The source population was all food handlers working in food establishments of East and West Gojjam Zones in 2020. Food handlers working in the food establishments were included in the study. None of the food handlers were excluded from the study.
Sample size determination and sampling procedure
The sample size was determined using both single and double population proportion formulas. The highest sample size was obtained from the single population proportion formula as determined using the formula
A multistage sampling technique was applied to select study participants. The primary and secondary sampling units were Woreda and food establishments, respectively. Motta, Dejen, Sinan, Debre Markos town, and Machakel were selected randomly among the Woredas found in East Gojjam Zone. Finote Selam, South Achefer, Sekela, Shendi, and Dembecha were randomly selected among the Woredas found in West Gojjam Zone. Then, food establishments were selected by systematic random sampling technique using a sampling interval of 3. Finally, one cooker and one waiter were selected from each food establishment by lottery method.
Study variables
The food hygiene practice of food handlers was the outcome variable. The independent variables were socio-demographic factors (age, sex, educational level, income, year of experience, and job type), institutional factors (type of the food establishment, availability of handwashing facility, PPE, and presence of supervisor), training on food safety, knowledge on food safety, attitude toward food hygiene practice, knowledge of food handlers on COVID-19 (good/poor), and inspection from health professionals.
Operational definitions
Level of food hygiene practice: there were a total of 23 questions that were used to assess the practice of food handlers on food hygiene coded as 0 for no and 1 for yes. The score on food hygiene practice ranges from 0 to 23. If the food handler scored less than the 60% of food hygiene practice-related questions (answered below 14 questions out of 23 questions), he or she considered as having a “poor level of food hygiene practice.” If he or she scored the 60% and above of the food hygiene practice-related questions (answered 14 and above questions out of 23 questions), he or she was considered as having a “good level of food hygiene practice.”
Level of knowledge on food hygiene: there were a total of 24 questions that were used to assess knowledge on food safety coded as 0 for no and 1 for yes. The knowledge on food hygiene score ranges from 0 to 24. If the food handler scored less than 60% of their responses to food hygiene knowledge-related questions (answered below 15 questions out of the 24 questions), he or she considered as having a “poor level of knowledge regarding food hygiene.” Those who scored 60% and above of the food hygiene knowledge-related questions (answered 15 and above questions out of the 24 questions), he or she was considered as having a “good level of knowledge on food hygiene.”
Attitude toward food hygiene: there were a total of 22 five Likert-type scale questions (coded as 1 for strongly disagree, 2 for disagree, 3 for neutral, 4 for agree, and 5 for strongly agree) that were used to assess the attitude of food handlers toward food hygiene. The attitude score ranges from 22 to 110. The respondents who scored less than 60% of the attitude score (scored below 66) were considered as having an “unfavorable attitude towards food hygiene.” Those who scored 60% and above of the attitude score (scored 66 and above) were considered as having a “favorable attitude towards food hygiene.”
Knowledge level on COVID-19 pandemic: there were a total of 21 questions that were used to assess knowledge on food safety coded as 0 for no and 1 for yes. The score ranges from 0 to 21. If the food handler scored 60% and above of knowledge-related questions on the COVID-19 pandemic (answered 13 and above questions out of the 24 questions), he or she is considered as having a “good level of knowledge regarding COVID-19 pandemic.”
Data collection tool and procedure
A semi-structured questionnaire was adapted from different pieces of the literature.4,9–13 The tool was addressed questions on socio-demographic characteristics, institutional factors, training on food safety, knowledge on COVID-19, knowledge on food hygiene, attitude toward food hygiene practice, and food hygiene practice (Supplementary File 1). The data collection tool was validated by conducting a pre-test prior to the study. Data were collected by interviewer-administered face-to-face interview with the presence of at least 2 m physical distancing between the interviewer and the interviewee. The data were collected by six trained BSc health professionals (nurse/public health/environmental health) and supervised by three Master of Public Health (MPH) professionals.
Data quality assurance
To assure the quality of the data, the questionnaire was prepared in English and translated to Amharic, and then back to English. Then, a 2-day training was given for data collectors and supervisors. A pre-test was done on 5% of the sample sizes out of the selected districts to improve the data collection tool and the skill of data collectors as well as supervisors. In addition, the data collection tool was validated by conducting a pre-test prior to the study. The Cronbach’s Alpha values were acceptable for the questions designed to assess the knowledge of the respondents on COVID-19 (Cronbach’s Alpha = 0.753), knowledge of the food handlers on food hygiene (Cronbach’s Alpha = 0.693), the attitude of food handlers toward food hygiene (Cronbach’s Alpha = 0.880), and practice of food handlers on food hygiene (Cronbach’s Alpha = 0.745). Moreover, day-to-day supervision took place during data collection by supervisors and investigators. The data completeness and consistency were checked by the data collectors and supervisors in the field.
Statistical analysis
The collected data were compiled, checked for any inconsistency and missed value, coded, and entered using Epi-data version 3.1 Software and exported into Stata 16.0 for data management and analysis. The reliability of the questionnaire was assessed using Cronbach’s Alpha. The data were cleaned for missing values by running frequencies and crosstabs. Descriptive analysis was performed to describe the study variables. Prevalence with a 95% CI was estimated for food hygiene practice among food handlers. Bi-variable and multivariable binary logistic regression was done to identify the factors associated with food hygiene practice among food handlers working in food establishments. Those variables with a p-value of less than 0.25 in bi-variable binary logistic regression were entered into the multivariable binary logistic regression model. 14 A statistically significant association was declared at a p-value of less than 0.05. The model fitness of the adjusted model was checked using the Hosmer and Lemeshow goodness-of-fit test which was 0.675. The findings were described in the text, percent, and odds ratio (OR) and presented using text, tables, and charts.
Results
Socio-demographic characteristics of the respondents
A total of 845 food handlers working in food establishments were approached for the study with a response rate of 98.9% (836 food handlers). Table 1 shows the socio-demographic and economic characteristics of the respondents. The majority of the respondents were from West Gojjam Zone (53.0%) and one-third of the respondents (33.6%) were from Debre Markos Town Administration. Regarding the sex of the respondents, the majority of them (85.6%) were female. Most of the respondents (77.5%) were within the age group of 18–29 years. Above one-third of the respondents (37.2%) were attended primary level education. In addition, the majority of the respondents (67.6%) were single. Half of the respondents (49.0%) were cooker regarding their job responsibility. The majority of the respondents (57.8%) had a work experience of 2 years and above. The majority of the respondents (56.9%) had a monthly income of less than 1100.00 Ethiopian Birr (ETB), which is the lowest salary scale in Ethiopia (Table 1).
Socio-demographic and economic characteristics of food handlers working in food establishments in East and West Gojjam Zones, North West Ethiopia, 2020 (N = 836).

ETB: Ethiopian Birr.
Food establishment related characteristics
Among a total of 836 food handlers, 220 (26.6%) were working in hotels. Regarding training, only 12.7% of the food handlers have ever attended training related to food hygiene. Most of the food handlers were working in food establishments having handwashing facilities (93.1%) and soap with the handwashing facility (84.1%). Similarly, the majority of the food handlers were working in food establishments having at least one PPE (67.3%) and a supervisor (74.8%). Two-thirds of the food handlers (66.1%) were working in food establishments that did not have pipe water in the kitchen (Table 2).
Characteristics of food establishments in East and West Gojjam Zones, North West Ethiopia, 2020 (N = 836).
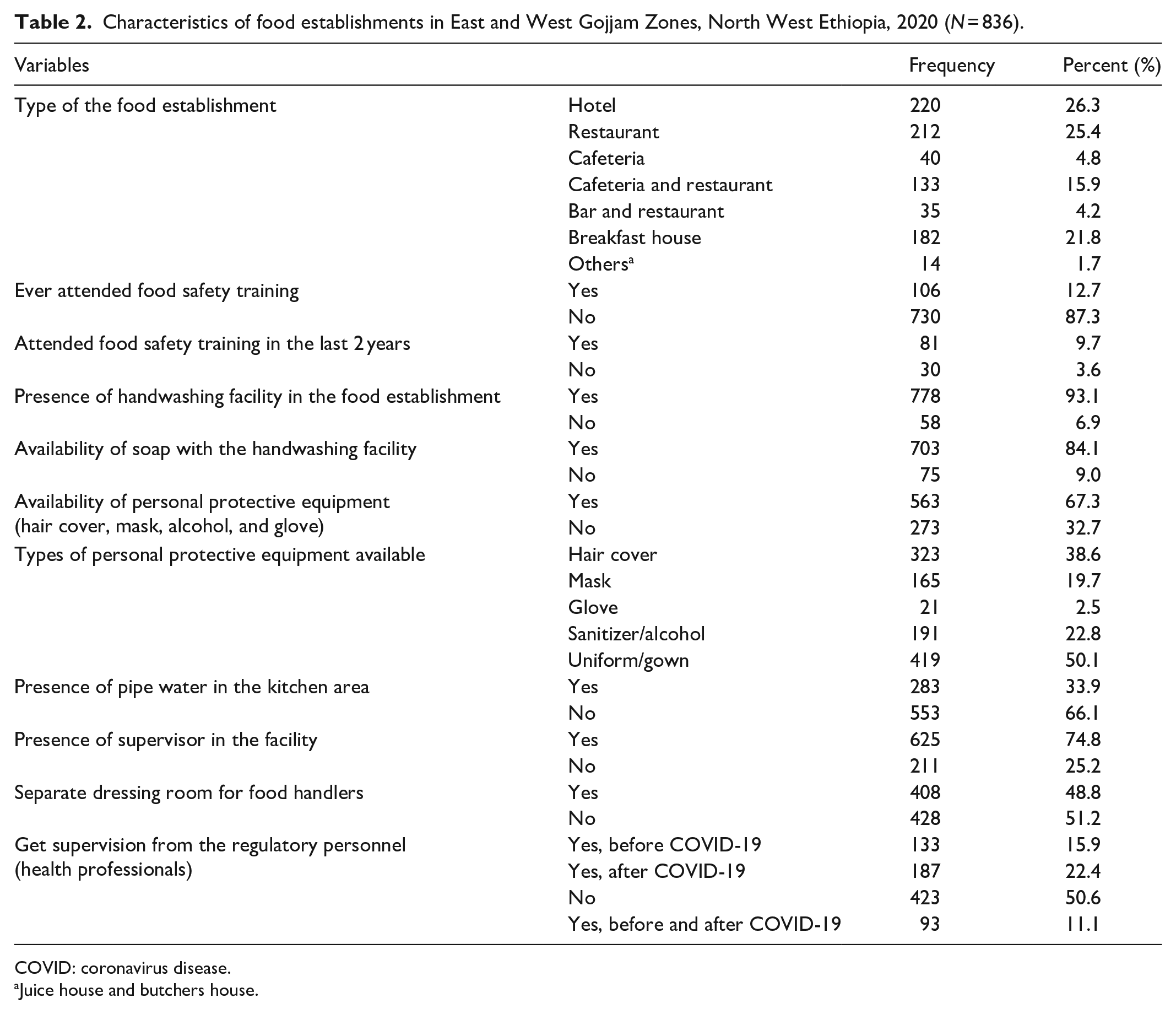
COVID: coronavirus disease.
Juice house and butchers house.
Knowledge of food handlers toward the COVID-19 pandemic
Almost all of the food handlers (96.5%) heard about the COVID-19 pandemic. The majority of the respondents (79.8%) mentioned cough as the main symptom of COVID-19. Only less than one-third of the food handlers mentioned chest pain, headache, chills, fatigue, loss of appetite, and throat pain as the main sign and symptoms of COVID-19 (Table 3).
Knowledge regarding the mode of transmission, signs and symptoms, mode of prevention and its fatality among food handlers working in food establishments in East and West Gojjam Zones, North West Ethiopia, 2020 (N = 836).
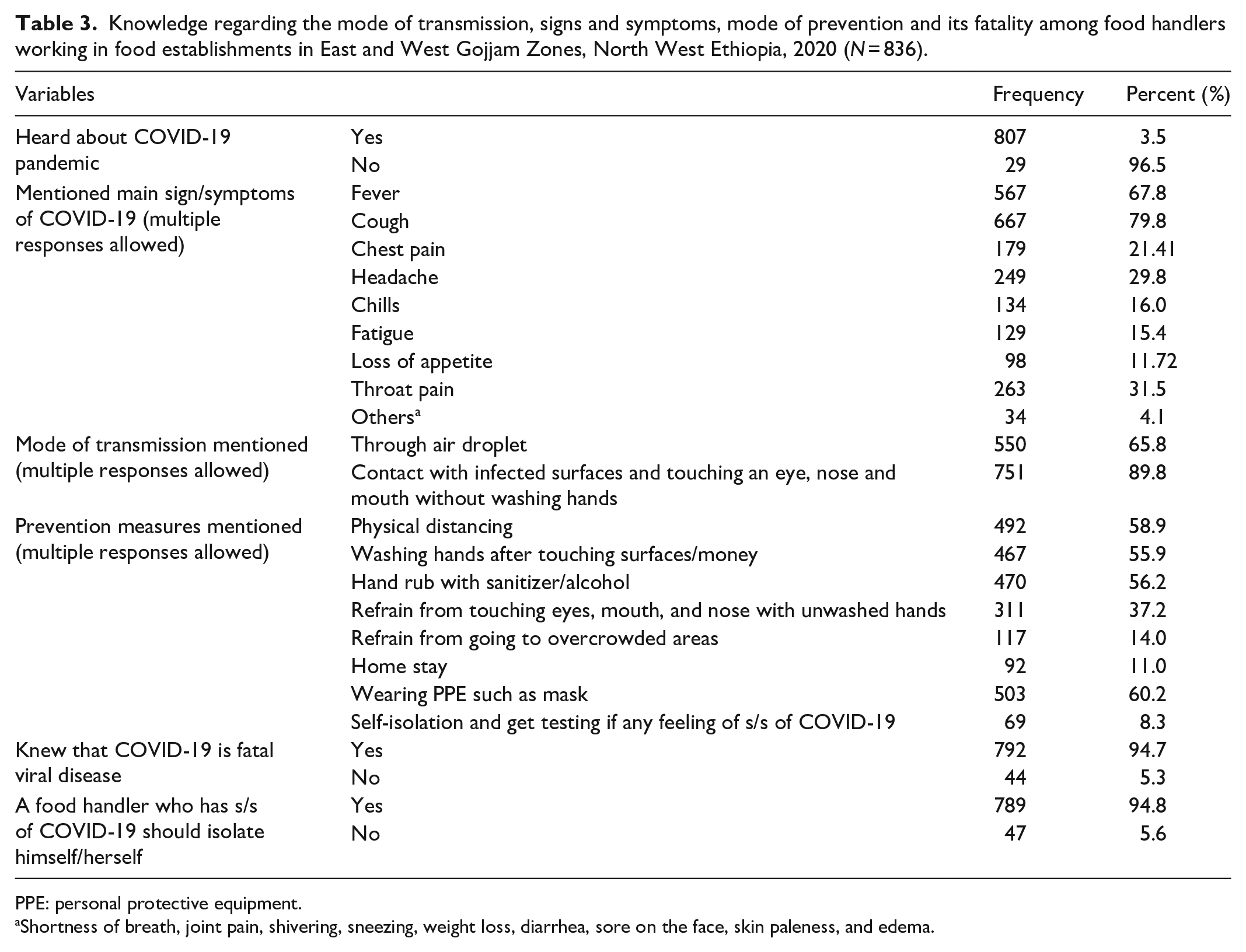
PPE: personal protective equipment.
Shortness of breath, joint pain, shivering, sneezing, weight loss, diarrhea, sore on the face, skin paleness, and edema.
Regarding the mode of transmission of COVID-19, the majority (65.8%) and most of (89.9%) of the respondents mentioned that COVID-19 is transmitted through air droplets and contact with infected surfaces and touching eyes, nose, and mouth without washing hands (Table 3). The majority of the respondents mentioned physical distancing (58.9%), washing hands after touching surfaces/money (55.9%), hand rub with sanitizer/alcohol (56.2%), wearing PPE such as mask (60.4%) as the methods of COVID-19 prevention. Most of the respondents did not mention homestay, self-isolation, and get testing if there is any feeling of sign/symptoms of COVID-19, refrain from touching eyes, mouth, and nose with unwashed hands, and refrain from going to overcrowded areas as the main prevention measures of COVID-19 (Table 3). Among a total of 836 food handlers working in food establishments in East and West Gojjam Zones, 689 (82.4% (95% CI = 79.7, 84.9%)) had poor knowledge about the COVID-19 pandemic.
Knowledge of food handlers toward food hygiene and safety
The magnitude of good knowledge on food hygiene among food handlers working in food establishments in East and West Gojjam zones was 99.6% (95% CI = 98.9, 99.9%).
Attitude of food handlers toward food hygiene practice
Among a total of 836 food handlers working in food establishments in East and West Gojjam Zones, all of them (100.0%) had a favorable attitude toward food hygiene practice.
Food hygiene practice and its associated factors
Food hygiene practice
Among a total of 836 food handlers working in food establishments in East and West Gojjam Zones, 51.2% (95% CI = 47.8, 54.6%) had poor food hygiene practices.
Factors associated with food hygiene practice
Table 4 shows the result of a multivariate logistic regression analysis fitted to identify factors associated with food hygiene practice. After adjustment for possible confounders such as sex, educational status, marital status, monthly income, job type, type of food establishment, ever attended training on food hygiene/safety, availability of handwashing facility, availability of PPE, presence of pipe water in the kitchen, presence of a supervisor, availability of separate dressing room, knowledge on food hygiene, we found that job type, availability of PPE, presence of pipe water in the kitchen, presence of a supervisor in the food establishment, and availability of separate dressing room were significantly associated with food hygiene practice among food handlers working in food establishments (Table 4).
The bivariate and multivariable logistic regression analysis to identify factors associated with food hygiene practice among food handlers working in food establishments in East and West Gojjam Zones, North West Ethiopia, 2020 (N = 836).

CI: confidence interval; COR: crude odds ratio; AOR: adjusted odds ratio; ETB: Ethiopia Birr; PPE: personal protective equipment.
Adjusted for sex, educational status, marital status, average monthly income, job type, ever attending food hygiene/safety training, type of food establishment, availability of handwashing facility, availability of PPE (hair cover, mask, alcohol, glove, and gown), presence of pipe water in the kitchen area, presence of supervisor in the facility, separate dressing room for food handlers, and knowledgeable toward COVID-19.
Juice house and butchers house.
The Hosmer and Lemeshow goodness-of-fit test of the adjusted model was 0.675.
p-value < 0.05; **p-value < 0.01; ***p-value < 0.001.
The odd of good hygiene practice was approximately three times higher among food handlers who were working as both a cooker and a waiter as compared to the odds among the food handlers who were working as a cooker (adjusted odds ratio (AOR) = 2.98; 95% CI = 1.02, 8.66) (Table 4). The odds of good hygiene practice were 2.67 times higher among food handlers who were working in food establishments having PPEs as compared to the odds among the food handlers who are working in the food establishment that does not have PPEs (AOR = 2.67; 95% CI = 1.75, 4.08) (Table 4).
The odds of good hygiene practice were 2.73 times higher among food handlers who were working in food and drink establishments having pipe water in the kitchen as compared to the odds among the food handlers who are working in the food establishment that does not have pipe water in the kitchen (AOR = 2.73; 95% CI = 1.84, 4.06) (Table 4). Likewise, the odd of good hygiene practice was 2.26 times higher among food handlers who were working in food and drink establishments having a supervisor as compared to the odds among the food handlers who are working in the food establishment that does not have a supervisor (AOR = 2.26; 95% CI = 1.41, 3.62) (Table 4). Moreover, the odds of good hygiene practice were approximately 2.69 times higher among food handlers who were working in food and drink establishments having a separate dressing room for food handlers as compared to the odds of food hygiene practice among the food handlers who are working in the food establishment that does not have a separate dressing room (AOR = 2.69; 95% CI = 1.84, 3.93) (Table 4).
Discussion
We conducted a facility-based cross-sectional study to determine the magnitude of food hygiene practice and identify factors associated with food hygiene practice among food handlers working in food establishments during the COVID-19 pandemic. The study found that 51.2% of food handlers had poor food hygiene practices. In addition, after adjustment for possible confounders, job type, availability of PPE, presence of pipe water in the kitchen, presence of a supervisor in the food establishment, and availability of separate dressing room were significantly associated with food hygiene practices among food handlers working in food and drink establishments during the COVID-19 pandemic.
This study showed that the prevalence of poor food hygiene practices among food handlers working in food and drink establishments during the COVID-19 pandemic was 51.2%. This figure is comparable to the study finding conducted at Dangila (47.5%) 15 and Woldia town (53.5%), 16 Ethiopia. However, it is not in line with findings from different parts of Ethiopia. It is higher compared to a study finding conducted in different parts of Ethiopia, specifically in Asosa town (32.2%), 4 Bahir Dar city (32.5%), 17 Gondar town (33.4%), 18 and Debre Markos town (46.3%). 19 Lack of training regarding food hygiene, not having a supervisor in the food establishments, and not having pipe water in the kitchen were the possible reasons for this high magnitude of poor food hygiene practice among food handlers in this study as evidenced by the findings of this study. The presence of high poor food hygiene practices among food handlers working in food establishments implies that the customers served in the food establishments were at risk of contracting foodborne diseases. This will create a double burden on the healthcare system during the COVID-19 pandemic. In addition, poor food hygiene practices during the COVID-19 pandemic results in food insecurity 20 and decreased dietary diversity practice which results in undernutrition. 21 This hinders the tackling of childhood stunting. 22 Thus, it needs an immediate intervention program that aims to improve the food handling practice of food handlers working in food establishments.
In addition, it is lower as compared to study findings conducted in Dire Dawa City Administration (70.1%), 3 Arba Minch town (67.4%), 10 and Debark town (59.9%). 23 The possible reasons for this lower magnitude of poor food hygiene practice among food handlers in this study were the better proportion of food handlers who got training regarding food hygiene and good food hygiene knowledge as evidenced by the findings of this study.
The odd of good food hygiene practice was approximately three times higher among food handlers who were working as both a cooker and a waiter as compared to the odd among the food handlers who were working as a cooker. Although there is no pre-existing evidence, the possible reason might be that most of the food handlers working as both a cooker and waiter were the owners of the food establishment and have a sense of better responsibility in order to attract customers.
Similarly, the odds of good food hygiene practice were 2.67 times higher among food handlers who were working in food establishments having PPEs as compared to the odds among the food handlers who are working in the food establishment that does not have PPE. This is in line with the previous evidence. 15
Likewise, this study showed that the odds of good hygiene practice was approximately 2.73 times higher among food handlers who were working in the food establishments having pipe water in the kitchen as compared to the odds among the food handlers who are working in the food establishment that does not have pipe water in the kitchen. This is in agreement with previous evidence. 17 This might be due to the existence of a kitchen that is conducive to food hygiene practice. This finding implies that all food establishments should have pipe water in a kitchen in order to improve the food hygiene practice of food handlers working inside the food establishment.
Furthermore, the odd of good hygiene practice was 2.26 times higher among food handlers who were working in the food establishments having a supervisor as compared to the odds among the food handlers who are working in the food and drink establishment that does not have a supervisor. This finding is supported by a study conducted at Arba Minch town, Southern Ethiopia. 10
Moreover, the availability of a separate dressing room was significantly associated with good food hygiene practices among food handlers working in food establishments. The odds of good hygiene practice were approximately 2.69 times higher among food handlers who were working in the food establishments having a separate dressing room for food handlers as compared to the odds of food hygiene practice among the food handlers who are working in the food establishment that does not have a separate dressing room. This finding is supported by previous evidence in Ethiopia. 15
The findings of the study should be interpreted considering the following strength and limitations. Since the study employed a multistage sampling method using a large sample size, the findings could be generalizable to all food handlers working in food and drink establishments during the COVID-19 pandemic in the study area. However, the practice of food hygiene was collected by observation using a structured checklist. As a result, some respondents might practice hygienic food practice perceiving that they are under observation. This might overestimate the prevalence of good food hygiene practices among food handlers working in food establishments during the COVID-19 pandemic. In addition, due to the cross-sectional nature of the study, it does not show a causal relationship between the dependent and independent variables.
Conclusion
In conclusion, the prevalence of poor food hygiene practices among food handlers working in food establishments during the COVID-19 pandemic was high compared to the literature. The type of job responsibility, availability of PPE, presence of pipe water in the kitchen, presence of a supervisor in the food establishment, and availability of separate dressing room were significantly associated with food hygiene practices among food handlers working in food establishments during the COVID-19 pandemic. Therefore, an interventional program that aims to improve food hygiene practice focusing on availing PPEs, pipe water in the kitchen, and ensuring the presence of a supervisor as well as a separate dressing room in the food establishment is recommended.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221081070 – Supplemental material for Food hygiene practice and its associated factors among food handlers working in food establishments during the COVID-19 pandemic in East Gojjam and West Gojjam Zones, North West Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221081070 for Food hygiene practice and its associated factors among food handlers working in food establishments during the COVID-19 pandemic in East Gojjam and West Gojjam Zones, North West Ethiopia by Alehegn Aderaw Alamneh, Daniel Bekele Ketema, Muluye Molla Simieneh, Moges Wubie, Yonas Lamore, Mekuanint Taddele Tessema, Abtie Abebaw, Biachew Asmare, Tsehay Alemu, Abraham Teym and Menichil Amsalu in SAGE Open Medicine
Footnotes
Acknowledgements
First, the authors acknowledge the College of Health Sciences of Debre Markos University for giving us an ethical clearance letter and writing a support letter to the study area. Second, our gratitude goes to the East Gojjam and West Gojjam Zone Health Bureaus which provided us with all the necessary information needed for this study. At last but not least, the authors thank all the respondents for their voluntariness and participation.
Author contributions
A.A.A. contributed to the conception and design of the work. A.A.A., D.B.K., M.M.S., M.W., Y.L., M.T.T., A.A., B.A., T.A., and M.A. contributed to the training data collectors and supervising the overall data collection process. A.A.A., D.B.K., M.M.S., M.W., Y.L., M.T.T., A.A., B.A., T.A., A.T., and M.A. contributed to the data entry, analysis, and interpretation of the data. A.A.A., D.B.K., M.M.S., M.W., Y.L., M.T.T., A.A., B.A., T.A., A.T., and M.A. wrote the manuscript. A.A.A., D.B.K., M.M.S., M.W., Y.L., M.T.T., A.A., B.A., T.A., A.T., and M.A. reviewed the manuscript. A.A.A., D.B.K., M.M.S., M.W., Y.L., M.T.T., A.A., B.A., T.A., A.T., and M.A. contributed to the final approval of the version to be published.
Availability of data and material
The data underlying the results presented in the study are available from the corresponding author upon a reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Research Ethics Committee of the College of Health Science of Debre Markos University, Ethiopia. The ethical approval number of the study was HSC/R/C/Ser/Co/471/13/12.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study got financial support from Debre Markos University, Ethiopia.
Informed consent
We obtained informed verbal consent from the study subjects whose age is 18 years and above. While we obtained assent from the study subjects whose age is less than 18 years, and also we obtained informed verbal consent through a phone call from their parents. The reason we took only verbal consent/assent is that the study did not involve advanced data collection procedures such as specimen collection and so on. Just the data were collected simply by interviewing and observation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.