
Abstract
Objective:
Central obesity is an emerging public health problem globally and an independent risk factor for heart, blood vessels, and metabolic disorder. This study aimed to assess the central obesity and associated factors among adults working in government offices in Bedele town, Southwest Ethiopia, 2021.
Methods:
An institutional survey was conducted among randomly selected government offices. Anthropometric measurements were carried out. Face-to-face interview using standard questionnaires were also used to collect data. A total of 403 respondents were selected from the list of public office workers employed in Bedele Town. Data were entered into Epi data 3.1 then exported to SPSS version 20 for analysis. Each variable with a p value less than 0.25 in the bivariate analysis was entered into logistic regression and p value 0.05 was considered as statistically significant.
Results:
The response rate was 373 respondents (92.6%). The overall prevalence of central obesity among public office workers of Bedele town was 54.7%. Sitting for more than 5 h at workplace adjusted odds ratio = 2.911 (95% confidence interval = 1.644, 5.156), being a female adjusted odds ratio = 3.258 (95% confidence interval = 1.744, 6.047), age range of 40–49 (adjusted odds ratio = 4.520, 95% confidence interval = 1.798, 11.363), age ⩾ 50 years (adjusted odds ratio = 5.907, 95% confidence interval = 1.808, 19.297), being physically inactive (adjusted odds ratio = 4.594, 95% confidence interval = 2.313, 9.125), consumption of snack (adjusted odds ratio = 4.521, 95% confidence interval = 2.583, 7.913), and alcohol consumption (adjusted odds ratio = 2.324 95% confidence interval = 1.210, 4.463) were factors significantly associated with central obesity among office workers in Bedele town.
Conclusion:
The magnitude of central obesity was high among office workers in Bedele town and being female gender, older age, physical inactivity, consumption of snacks, and alcohol were associated with it. Physical exercise and a healthy lifestyle should be promoted to minimize the problem.
Introduction
Obesity can be defined as an abnormal medical condition when high fat is accumulated within the body. 1 Obesity affects an individual’s health. The type of obesity called central obesity is the most common nutritional abnormality. It is defined as high accumulation of visceral fat in the abdominal area. 2 The reason behind central obesity development is that energy consumption and expenditure is not balanced. 3
The reason behind central obesity development is that energy consumption and expenditure is not balanced. 3 It has been known that obesity is a world health problem. The causes of obesity can be nutritional transition of energy dense foods that are high in fat and/or sugars and low in dietary fiber, fruits, and vegetables. 4 Food transition and other factors like not engaging in physical exercise, mode of transportation, increasing urbanization, and generally lifestyle of an individual will aggravate the level of obesity. 1
Body mass index (BMI) is the most commonly used measure of obesity. 1 It can be used as a screening tool at an individual level because it estimates body fat but it neither gives diagnostic value of the body fatness nor the health of the individual. 5 But it does not directly measure body fat. 6 Although obesity confers a major threat to the health, the dissemination of body fat is of great importance in the determining of its health threat. So it would not be appropriate to use BMI alone as a health indicator since individuals with normal weight could sometimes have central obesity. 7
Instead, waist circumference (WC), waist-to-hip ratio (WHR), or waist-to-height ratio (WHtR) is reported to be better predictors of obesity. 8 Studies showed that the risk of metabolic complications is not totally attributable to excess body weight, but to the location of this excess weight, particularly central obesity unlike gynoid obesity. 9 Hence, abdominal obesity was established to be the most prevalent cause of cardio-metabolic risk, even among those with a normal BMI.10,11
Central obesity is defined by World Health Organization (WHO) as, WC measurement of >94 cm for men and >80 cm for women, WHR ⩾ 0.90 for men and ⩾0.85 for women, and WHtR cut-off points for the increased cardiovascular risk, 12 that differ among diverse ethnic groups due to differences in energy imbalance, physical activities, and body build level.13,14
Obesity is a significant public health problem affecting more than half a billion people globally. It is a major threat to health throughout the world and killing more people than those who are underweight. 1 If action is not taken globally an estimated 57.8% of adults will be expected to be classified as people with obesity by 2030.15,16
In the recent, obesity was considered as a problem in high-income countries; but nowadays the number of overweight people and having obesity has been rising in the low- and middle- income countries, especially in the urban settings. 17 Office workers are at a higher risk of obesity due to sedentary work accompanied by stress, drinking, smoking, lack of exercise, and irregular meals. 18 Recently, studies conducted in different parts of the African continent have been showing that central obesity is growing faster.8,19 –21
Studies conducted in different regions indicate the significant prevalence of central obesity to be 21.29%, 19.6%, and 26% in Mizan Aman town, Addis Ababa, and Jimma University teaching hospital, respectively.22 –24 Non-communicable diseases are estimated to account for 39.3% of the total deaths in 2016 in Ethiopia. 25 About 31% of deaths reported from hospitals in Addis Ababa were attributed to diabetes mellitus and cardiovascular diseases (CVDs). 26 The prevalence of metabolic syndrome was 20.1% among working adults in Eastern Ethiopia.27,28
According to the Ethiopian law of labor proclamation, Ethiopian public office workers are expected to spend the 8 working hours of a day in their office during the working days of the week. 29 Sitting time at office, coupled with time spent on leisure time, was also associated with cardio-metabolic risk biomarkers, with sitting time being an independent risk of central adiposity. A review of studies on sedentary behavior and health found that adults spend 46%–59% of the day being sedentary and indicated that this could be a new focus of research area. 30
For public health intervention programs to be more effective in the reduction of obesity and related risk of non-communicable diseases, special attention should be paid to a common risk factor such as sedentary lifestyles among groups of people, office workers in particular, who are at more risk of exposure to sedentary lifestyles. 31
Although office workers do not have well-established and legally bound breaks to support physical activity, studies on central obesity and associated factors, in particular, have not been conducted in the study area yet. Therefore, this study was conducted to assess the magnitude of central obesity and its associated factors among public office workers in Bedele town in southwest Ethiopia, 2021.
Methods and materials
Study area, design, and period
An institution-based cross-sectional study was conducted from April to May 2021 in public offices in Bedele town, 480 km away from the capital city of the country, Addis Ababa, to the southwest and has a total population of 32,325. According to the 2021 report of public service and Human resource management, there are 32 public offices and 1498 public office workers in the town.
Eligibility criteria
All employees working in public offices of Bedele town were included, whereas pregnant women were excluded from the study.
Sample size determination and sampling technique
Determined using a single population proportion formula by considering 49.4% prevalence of central obesity from the study conducted in Addis Ababa Public Office workers 30 and our total sample size after adding 5% nonresponse rate was 403. A simple random sampling technique was utilized. The researcher obtained a complete list of all employees from the public service and human resource management office and then all the employees were allocated a number. To select those who were to be included in the sample numbers were randomly drawn from a small box; those whose numbers were chosen were required to voluntarily participate in the study. In the case of selected employees who were transferred or fired during the study period, they were replaced by other randomly selected employees complying with the sample criteria.
Data collection tool and procedure
Interviewer-administered structured questionnaires that were adapted from WHO-STEP wise for non-communicable diseases surveillance, Ethiopian Demographic Health Survey, WHO Global Physical Activity Questionnaires (GPAQs), and Food and Agricultural Organization (FAO) were used to collect the data.32 –35 The questionnaires consist of socioeconomic, behavioral, diet-related, physical activity questions, knowledge toward obesity, and anthropometric measurements of WC. Data were collected by three BSc nurses and three health officers assigned as supervisors.
Assessment of dietary factors and physical activity
Dietary pattern was assessed by using food frequency questionnaires (FFQs) adopted from WHO stepwise, which is used to assess frequency of consumption of different types of food groups and to assess dietary pattern, participants were asked to report the number of times they consumed weekly from the past months. 32
The GPAQ developed by WHO for physical activity surveillance was used to assess the physical activity pattern among selected participants. 36 This is based on intensity, duration, and frequency of physical activity at work, in recreational settings and involving transportation (journeys) using a set of 16 questions.
Knowledge toward obesity
To assess knowledge of the participants toward obesity, 12 standard questions adopted from FAO was used. 35 Based on this question, the mean of their score was taken to classify them as having poor knowledge or good knowledge toward obesity. Those who responded less than mean were classified as poor knowledge toward obesity, while those who responded greater than or equal to mean were classified as good knowledge toward obesity.
Anthropometric measurements
WC was measured at the midpoint between the lower margin of the least palpable rib and the top of the anterior superior iliac crest in the mid-axillary line using non-stretchable fixed tension tape which was wrapped around at this point, parallel to the floor, ensuring it was adjusted without compressing the skin. While taking the measurement, the participant had to wear light clothes, stand relaxed with feet close together, arms at the side, and body weight evenly distributed. The measurement was taken at the end of a normal expiration. Each measurement was repeated twice; when the measurements are within 1 cm of one another, the average was calculated. When the difference between the two measurements exceeded 1 cm, the two measurements were repeated. 12
Operational definition and definition of terms
Adult: a person whose age group is between 20 and 64 years. 37
Central obesity population: for Ethiopian adults measure of WC for male is ⩾83.7 cm and female ⩾78 cm. 14
Meal frequency: number of meals consumed per day. 24
Snacking: eating between breakfast and lunch and between lunch and dinner. 38
Fast food consumption: consumption of fast foods like burger, pizza, chips, biscuit, “sanbusa,” and the like. 39
Eating outside: the purchase and consumption of meals and snacks prepared outside of the home, at least once in the reporting period. 33
Physically active: this is if the participants’ total physical activity MET-minutes/week is at least 600.
Physically inactive: this is if the participants’ total physical activity MET—minutes/week is <600. 34
Smoking status: in this study it was categorized as follows:
A daily smoker: defined as one who smoked at least one cigarette per day (at least seven cigarettes per week). Those who smoked less than one cigarette per day or seven cigarettes per week
Occasional smokers: those who smoked less than one cigarette per day or seven cigarettes per week.
Current smokers:—included daily and occasional smokers.
Ex-smokers: those who had smoked at least one cigarette per day for at least 6 months but had quitted.
Never smokers: those who had never smoked at all. 40
Alcohol drinking: consumption of alcohol within the past 30 days, irrespective of its quantity during the data collection periods. 41
Sleep duration: the average of the difference between bedtime and wakeup time in a typical day. 30
Ensuring data quality
To ensure data quality, a pretested standard questionnaire and fixed tension measuring tape was prepared. Data collection instrument was pretested on 5% of the sample size outside of the study area from Chora district randomly and a necessary modification was made on the instrument. Training on the topic and purpose of the research on how to approach the study subjects and how to use the questionnaire was given for 3 days for the data collectors and the supervisor. The collected data were checked out for completeness, accuracy, and clarity by the Principal investigator and Supervisors. This quality checking was done daily after data collection and correction was made before the next data collection measure. Data clean-up and cross-checking was done before analysis.
Statistical analysis
Data were checked for completeness and consistencies, coded and entered into Epi data 3.1, then exported to SPSS version 20 for cleaning and analysis. Descriptive analysis was conducted to show frequency distribution and to summarize the data. Binary logistic regression was done to investigate the association between each explanatory variable and central obesity.
To control the effect of confounding factors or to get independently associated variables, each variable with p value less than 0.25 in bivariate analysis were entered into multiple logistic regression models as the independent variable and p value < 0.05 was considered as statistically significant for all the independent variables in the final model. Goodness of fit of the model was checked using Hosmer Lemeshow’s goodness-of-fit test considering good fit at p value ⩾ 0.05 (0.486). The results were organized and displayed using tables, graphs, and statements.
Ethical considerations
Ethical approval for this study was obtained from the ethical Review Committee of Mettu University, College of Health Science and department of Public Health. Letter of ethical approval was obtained from the Institutional Review Board (IRB) of College of Health Science, Mettu University. Permission letter was taken from Bedele town administrative office and a Support letter was written for each selected public office. Privacy and confidentiality of the interviews and information gathered were assured.
Results
Sociodemographic and economic characteristics of the study participants
Out of 403 sampled participants, 373 participated in the study making a 92.6% response rate. Of the total respondents, 222 (59.5%) were males, 192(51.5%) were Protestant, 310 (83.1%) were married, and 220 (59%) had a bachelor’s degree. The mean (SD) of age of the respondents was 37.3 ± 8.5 years, out of which 45.8% were between 30 and 39 years (Table 1).
Sociodemographic characteristics of public office workers in Bedele town, 2021 (n = 373).

Behavioral characteristics of the study subjects
Most of the study populations (96.5%) never smoked cigarettes, while 3.5% of them were currently smoking; 31.9% of the participant’s had drunk alcohol within the past 30 days (Table 2).
Behavioral-related factors of adults working in Bedele town, 2021 (n = 373).

Dietary pattern characteristics of participants
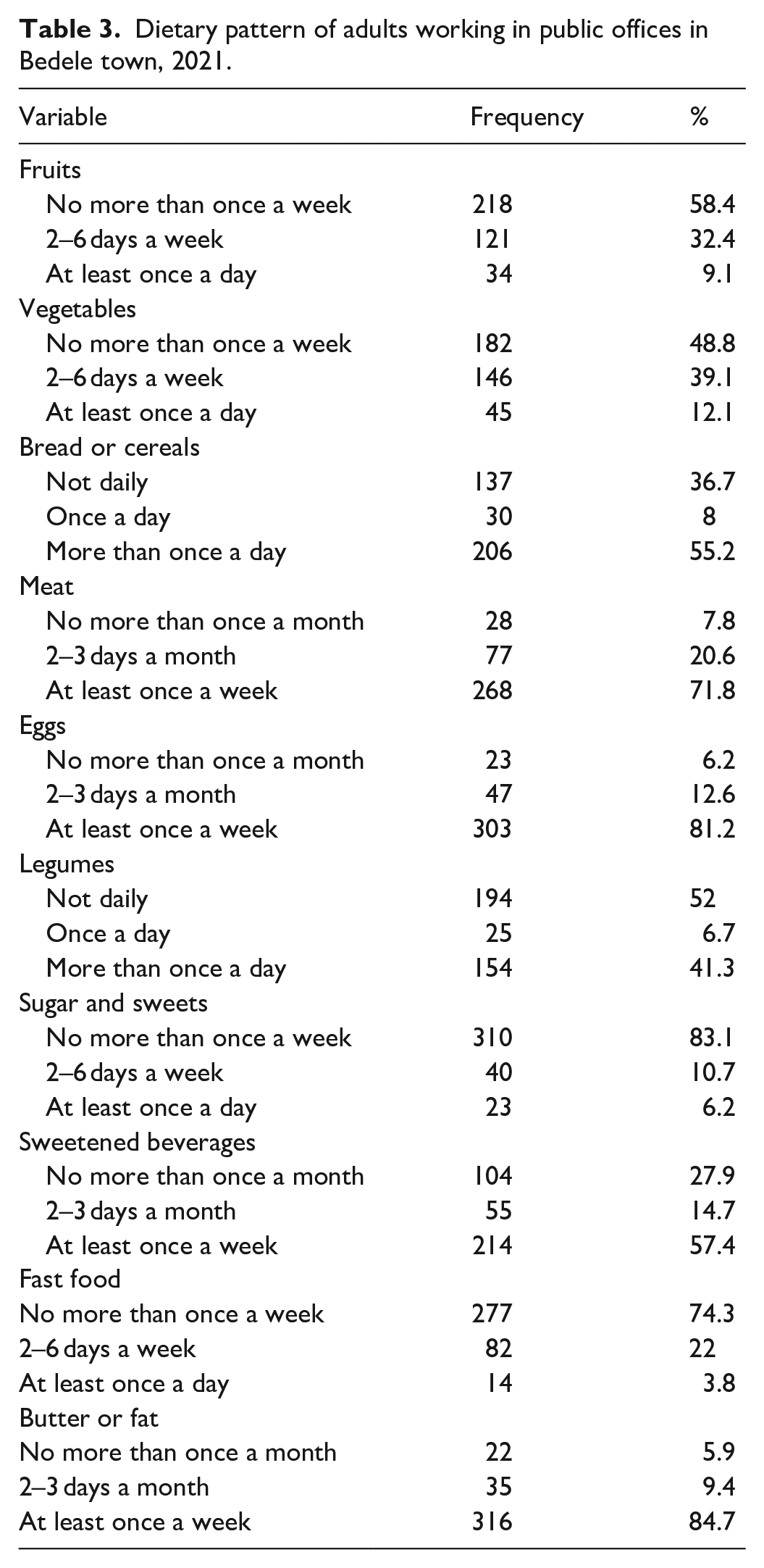
Based on the data from food consumption frequency, 206 (55.2%) of the participants consumed bread and 45 (12.1%) respondents consumed vegetables at least once a day, while 268 (71.8%) of them consumed meats at least once a week (Table 3).
Dietary pattern of adults working in public offices in Bedele town, 2021.
Dietary habits of participants
Regarding dietary habit, 177 (47.5%) of the respondents had meal frequency of three and above, while 153 (41%) of them did not consume breakfast daily, and 209 (56%) of the respondents consumed snacks at least once a day. Of the total respondents, 51 (13.7%) of them consumed a meal (Table 4).
Dietary habit of adults working in public offices in Bedele town, 2021 (n = 373).

Sedentary behaviors of participants
Regarding sedentary behaviors, 197 (52.8%) of respondents spent more than or equal to 5 h sitting at work daily, while 213 (57.1%) of the respondents spent at least 2 h sedentary watching TV, and 195 (52.3%) of them spent more than 1 h sedentary while using computers at home. Regarding knowledge toward obesity, 126 (33.8%) of respondents had poor knowledge of obesity (Table 5).
Sedentary behaviors of adults working in public offices in Bedele town, 2021.

Prevalence of central obesity
The overall magnitude of central obesity among the study office workers was 54.7% (95% confidence interval (CI) = 50.1%, 59.8%) as measured by WC. It was 49.1% and 62.9%, in men and women, respectively (Figure 1).

The overall magnitude of magnitude of central obesity among adults working in government offices in Bedele town, Buno Bedele zone, southwest Ethiopia.
Factors associated with central obesity
In multivariate analysis, sitting for more than 5 h at workplace adjusted odds ratio (AOR) = 2.911 (95% CI = 1.644, 5.156), being a female AOR = 3.258 (95% CI = 1.744, 6.047), age range of 40–49 (AOR = 4.520, 95% CI = 1.798, 11.363), age ⩾ 50 years (AOR = 5.907, 95% CI = 1.808,19.297), being physically inactive (AOR = 4.594, 95% CI = 2.313, 9.125), consumption of snacks (AOR = 4.521, 95% CI = 2.583, 7.913), and alcohol consumption (AOR = 2.324, 95% CI = 1.210, 4.463) were factors significantly associated with central obesity among office workers in Bedele town (Table 6).
Factors associated with central obesity among public offices workers in Bedele town, 2021 (n = 373).
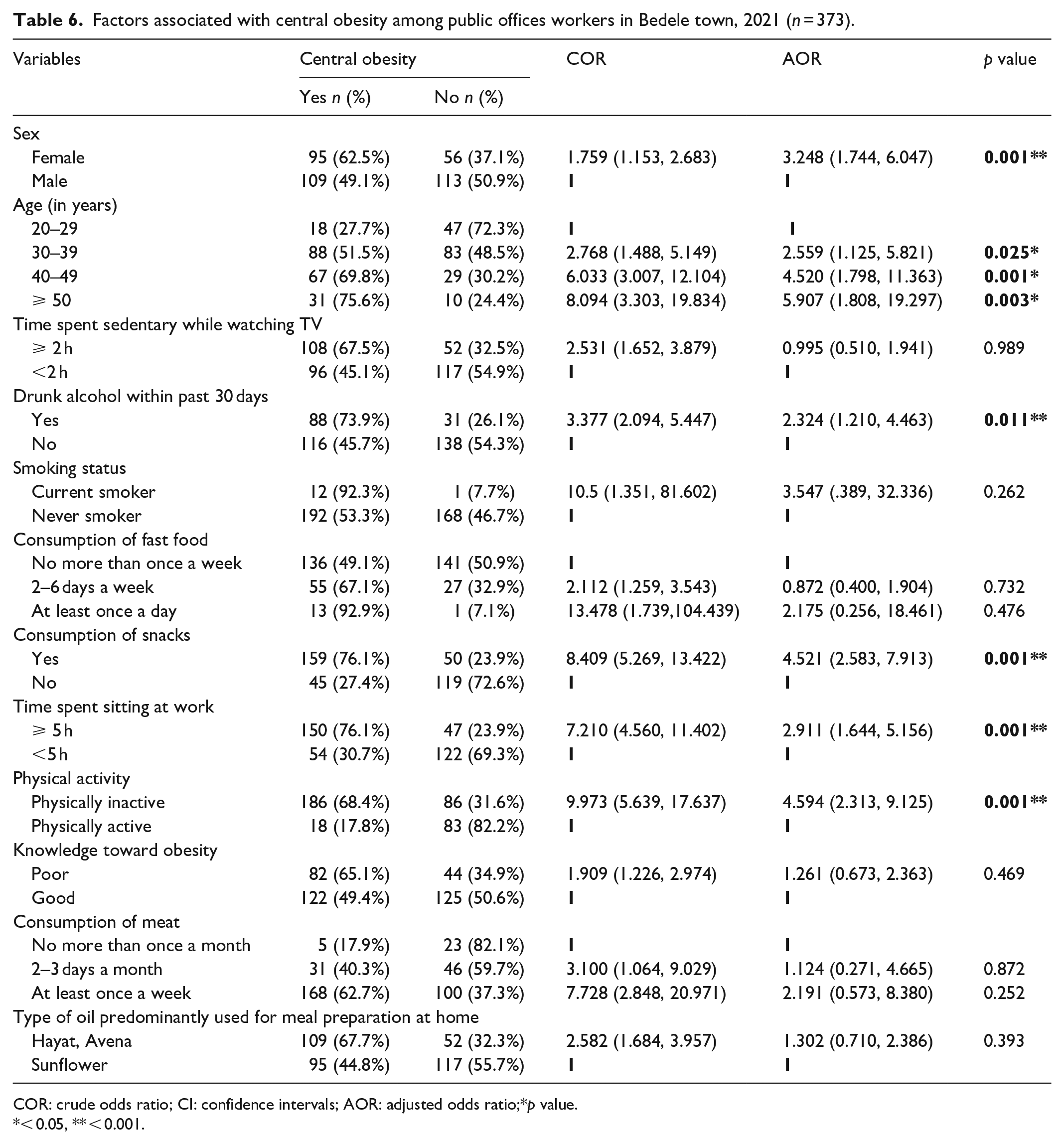
COR: crude odds ratio; CI: confidence intervals; AOR: adjusted odds ratio;*p value.
< 0.05, ** < 0.001.
Discussion
The purpose of this study was to assess the magnitude of central obesity and the associated factors among public office workers in Bedele town, Buno Bedele Zone, Southwest Ethiopia. The overall magnitude of central obesity among the study office workers was 54.7% (5% CI = 50.1%, 59.8%). The prevalence of central obesity in this study was in line with the finding from the studies conducted in Wolaita Sodo 52.7%, 42 Gondar 58.5%, 43 and southwestern Nigeria 56.8%. 44
However, our finding was higher than the studies conducted in Dodoma region of Tanzania 24.88%, 20 Jimma University Teaching hospital 26%, 24 and the study in Addis Ababa 49.4%. 30 This might be due to the fact that there is a considerable difference in the study periods, place, and operational definition they use for central obesity. However, it was lower compared with the study done in India 71.2% 45 and in eastern Sudan 67.8%. 46 This might be due to the sociocultural background, methodological difference which is primarily explained by the difference in sample size, and also the setup in which the study was conducted.
This study showed that females were more likely to be the centrally obesity population compared with males. This is consistent with the findings of the study done in Ethiopia (Nekemte town), South Africa, Uganda, and Tanzania.20,21,47,48 This is due to the hormonal changes at the time of menopause, and fat that is regained after the postpartum period relatively, which is stored more in the central part of the body; additionally, the cultural way of comforting women after giving birth, especially in Ethiopia, are the reasons that will cause women to be the centrally obesity population. The other possible reason for this variation in prevalence could be that females have more steroid hormones which expose them to obesity; 42 the use of hormonal contraceptives are other possible factors. 49
In this study, the risk of abdominal obesity increased with age, which was again supported by previous studies done in China and Nigeria.28,50 The possible explanation for this might be physiological change in reduction of basal metabolism and reduction in physical activities causing decreased energy expenditure as age increased, leading to positive energy balance; hormonal changes during aging can be another factor, as aging is associated with a decrease in growth hormone secretions, reduced responsiveness to thyroid hormone, and decline in the amount of muscle mass, which leads to a decrease in metabolism.24,42
The result of this study shows that individuals who consume alcohol were 2 times more likely to have central obesity than their counterparts. A similar finding was observed in a study conducted among adults in northeast Ethiopia, 51 Tamale, Ghana, 52 and in Spain. 53 The reason for this is that alcohol is an extra energy which adds to the total daily energy intake by itself and inhibition of fat oxidation occurs as a consequence of the anti-lipolytic properties of metabolites from alcohol degradation, thereby favoring lipid storage and hence promoting an increased risk of developing obesity. 24
Snack users also had 4.5 times more increase in the likelihood of central obesity. In this study, snacking is positively associated with central obesity. Similarly, a study in the United States showed that as the eating frequency increases, regardless of the amount of energy central obesity also increases. 54
Beyond the additional eating frequency from the regular food which adds energy, the type of food that is eaten during snacking are mostly energy-dense foods such as caloric beverages and fried foods and low in fiber; 38 complementary with alcohol use and physical inactivity it will lead to weight gain and obesity. The role of eating frequency in obesity development is debated; it is also argued that snacking may increase diet quality by increasing intakes of fruit, whole grains, and fibers, which could promote satiety and reduce risks for obesity. 55 However, the reason for the inconsistent association between central obesity and snacking status could be due to the variation in the definition of snacking, difference in the frequency and kind of foods eaten for snacking, which was not measured in this study, and the type of study design used.
This study also found that workers who spent sitting at least 5 h at work had 3 times higher odds of central obesity than those who sat for less than 5 h. This was supported with the result of a study conducted in Addis Ababa which found sedentary working individuals had more body fat. 30 The reason might be participants spend much time sitting and involved less physical labor leading them to a sedentary lifestyle. This might determine the number of calories stored in the body in the form of fat. 56
The findings showed that physically inactive individuals were 5 times more likely to be the centrally obesity population than physically active ones. The finding is consistent with the study conducted in rural northeast China 28 and West Africa. 19 The reasons could be physical inactivity can lead to positive energy balance and accumulation of fat around the waist (visceral area) and once obesity was established, habitual physical activity remained extremely low, denoting low energy expenditure.
Limitations of the study
Since the study was institution based, it could possibly affect generalization. Other factors that can affect excess body weight like genetic factor and underlying health conditions were not addressed in this study. The study was also unable to do biochemical and other advanced methods of measuring central adiposity. Since this is a cross-sectional study, the issue of temporality is questionable. Finally, some variables were identified from self-reported data, which might be affected by recall bias.
Conclusion
The findings of this study showed that the magnitude of central obesity was substantially high and being female, older age, physical inactivity, consumption of snacks, and alcohol were associated with central obesity. Physical activity and a healthy lifestyle should be promoted to minimize the problem.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221105993 – Supplemental material for Magnitude of central obesity and associated factors among adults working in government offices in Bedele town, Buno Bedele zone, Southwest Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221105993 for Magnitude of central obesity and associated factors among adults working in government offices in Bedele town, Buno Bedele zone, Southwest Ethiopia by Workineh Tefera, Muluneh Shuremu, Amanuel Tadelle, Daba Abdissa and Zelalem Banjaw in SAGE Open Medicine
Footnotes
Acknowledgements
The authors acknowledge Bedele Town public service office and the human resource management for providing with the total number of manpower and the number of public offices. They also acknowledge the data collectors, supervisors, Banche Maru and participants in the study.
Data availability
The original data of this study is available for the third-party only upon author’s request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the ethical Review Committee of Mettu University (reference number RPG/12/2013), College of Health Science and department of Public Health. Letter of ethical approval was obtained from the Institutional Review Board (IRB) of College of Health Science, Mettu University. Permission letter was taken from Bedele town administrative office and also Support letter was written for each selected public office.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Permission was obtained from each office head. After getting permission from the offices, eligible and volunteer office workers were included in the study. Written informed consent was sought from each office worker. Each participant in the selected offices was given a written consent form which included the aim, procedure, and benefit of the study. Selected office workers who were willing to participate in the study were included in the study. Privacy and confidentiality of the interviews and information gathered was assured.
Trial registration
Trial registration was not applicable for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.