
Abstract
Objective:
In Ethiopia, only a few studies were conducted to determine factors contributing to antiretroviral treatment failure, in general, and there are no published data in the study area, in particular. Thus, the aim of the study was to assess the determinants of first-line treatment failure among adult HIV patients on antiretroviral treatment at Nekemte Specialized Hospital, western Ethiopia.
Methods:
The hospital-based 1:2 unmatched case–control study was conducted in Nekemte Specialized Hospital from 1 August to 30 September, 2019, on 252 HIV-positive patients receiving antiretroviral treatment (86 cases and 166 controls). Cases were selected from patients who were switched to second-line antiretroviral treatment regimen after first-line antiretroviral treatment failure. Controls were from those who are on the first-line antiretroviral regimens for at least 6 months. Data were collected by two trained clinical nurses. Record review and an interviewer-administered questionnaire were used to collect data. Data were entered into Epi-Data, version 7.2.2, and then exported to SPSS, version 25, for analysis. The association between treatment failure and each covariate was assessed by bivariate analysis to identify candidate variables at p value < 0.25. All candidate variables were entered into multivariate analysis done in stepwise backward likelihood ratio to declare statistical significance association at p value < 0.05, 95% confidence interval.
Results:
Data from a total of 252 (86 cases and 166 controls) patients were extracted at a response rate of 98.4%. Statistically higher odds of first-line treatment failure were observed among those who started treatment at an advanced stage (Baseline World Health Organization stage 3 o r4 (adjusted odds ratio = 3.12, 95% confidence interval: 1.55–6.26), lower Baseline CD4 count < 100 cells (adjusted odds ratio = 3.06, 95 % confidence interval: 1.45–6.50), lack of participation in a support group (adjusted odds ratio = 4.03, 95% confidence interval: 1.98–8.21), history of antiretroviral treatment discontinuation for greater than 1 month (adjusted odds ratio = 2.36, 95% confidence interval: 1.17–4.78) and poor adherence to antiretroviral treatment (adjusted odds ratio = 3.09, 95% confidence interval: 1.54–6.19).
Conclusion:
Antiretroviral treatment initiation at an advanced stage, lower CD4 count, no participation in a support group, and poor adherence were determinants of treatment first-line antiretroviral treatment failure. Therefore, health care providers and program developers should give special attention to; early diagnosis and start of treatment, encouraging patients to participate in a support group, trace patients early, and attentively follow patients to improve their adherence to antiretroviral treatment.
Introduction
Since the start of the epidemic, 75.7 million people have become infected with HIV and 32.7 million people have died from AIDS-related illnesses. 1 The Joint United Nations Program on HIV/AIDS (UNAIDS) has set new targets in 2014 toward the elimination of HIV including diagnosis of 90% of HIV-infected individuals, access to treatment for 90% of identified HIV-infected persons, and 90% viral suppression among those initiated on treatment. 2 Globally, only 47% of HIV patients on antiretroviral treatment (ART) reach the required viral load suppression status while in sub-Saharan Africa; only 29% of people living with HIV have achieved viral suppression.2,3
Although significant progress exists, there is a significant gap in reaching the third “90%” (viral suppression) of the UNAIDS in vulnerable populations of low- and middle-income countries. 4 Currently, there are nearly 11 million persons living with HIV who need to attain the third “90” (viral suppression) UNAIDS target by 2020. 5
A number of factors that may be associated with virologic failure have been highlighted by previous studies. Patients with higher baseline World Health Organization (WHO) clinical stages (3 or 4) or higher baseline CD4 count are at high risk for immunological treatment failure. 6 Poor adherence, body mass index (BMI), and low CD4 count have been associated with virologic treatment failure. 7 Virologic failure may also be caused by patient-related factors such as co-morbidities, intermittent access to ART, missed clinic appointments, and antiretroviral (ARV) regimen–related factors, such as drug adverse effects, suboptimal virologic potency, pharmacokinetics, food requirements, and among other factors.8,9
The magnitude of first-line ART treatment failure differs across the countries and regions depending on clinical, immunological, or virologic diagnostic criteria used. 10 Because of non-specificity, diagnosing treatment failure by immunologic or clinical criteria may increase or decrease the numbers of patients switched to a second-line treatment options.11,12 Patients are receiving medications with some adverse effects when they are switched to second-line treatment options. As a result of this, adherence to the medications becomes less, and the progression of HIV/AIDS will be more rapid, which make patient monitoring more difficult and expensive. 13 The availability of second-line ART regimens is too limited in developing countries. 14 At the individual patient level, a failed ART regimen or HIV drug resistance limits treatment options complicates succession of therapy, and puts the patient at increased risk for drug toxicity. 15 According to some literature, if the level of pretreatment non-nucleoside reverse transcriptase inhibitors (NNRTIs) drug resistance exceed 10%, then drug resistance is predictable with attack frequency of 105,000 and 135,000 incidences and deaths related to HIV/AIDS, respectively, in sub-Saharan Africa between 2016 and 2020. 16 Therefore, early and accurate diagnosis for first-line ART failure decreases the number of patients who develop drug-resistant HIV strain. 17
In Ethiopia, among patients on highly active antiretroviral therapy (HAART), only 51% of them had viral suppression where significant number of patients’ viral load were non-suppressed, 5 which could lead to treatment failure. Currently, only viral load measurement determines HIV treatment failure and is confirmed by two viral load tests (viral load ⩾ 1000 copies/ml), performed 3 months apart as per national guideline, before a change of ART regimen. 18
In general, limited studies7,14,19 have been done on determinants of virologic treatment failure among patients receiving first-line ARV therapy using routine viral load testing as a measure of treatment failure, and no similar study was done particularly in the study area. To achieve a high treatment success rate, identifying and intervening factors responsible for virologic treatment failure is very important. Therefore, this study was aimed to investigate determinant factors for first-line ARV therapy failure at Nekemte Referral Hospital using the virologic using plasma viral load.
Methods
Study design and setting
The unmatched (1:2) case–control study was conducted at Nekemte town, East Wollega Zone of Oromia region, western Ethiopia which is located 331 km away from the capital city, Addis Ababa to the west direction. The total population of the town was about 128,380 based on the data from the town’s health bureau of 2019. There are four public health facilities in the town; two hospitals (Nekemte specialized and Wollega University referral hospital) and two health centers (Chalalaki and Nekemte health center).
These health institutions currently provide HIV care and treatment services for 3131 people. Large numbers of patients (2276) follow their care at Nekemte Specialized Hospital and relatively small numbers (55) follow their care at Wollega University Referral Hospital. In health centers, 798 patients were on ART, whereas only 70 HIV patients were on care at Chalalaki Health center and the others, 728 were on ART at Nekemte Health Center. Although all of these public institutions were providing HIV care and treatment services, the study was conducted only in Nekemte Specialized Hospital since it is the only hospital where first-line ART regimen failure is treated in the Nekemte town.
There are total of 197 patients who switched to a second-line regimen at Nekemte Specialized Hospital Since 2012. Routine viral load measurement was started in 2017 in Nekemte public health research and referral laboratory. Currently, the WHO standard machine (Abbott m2000sp) 20 is available for viral load measurement and report from referral laboratory is used to diagnose treatment failure.
Source and study population
All HIV-infected patients aged 15 years and above who had taken first-line ART for at least 6 months were the source population. Cases were HIV patients aged 15 years or older who were switched to second-line ART after first-line ART failure diagnosed by plasma viral load ⩾1000 copies/mL in two consecutive viral load measurements in a 3-month interval. Controls were HIV-infected patients aged 15 years and older on first-line ART whose plasma viral load was <1000 copies/mL in two consecutive viral load measurements after at least 6 months of treatment.
Inclusion and exclusion criteria
Inclusion criteria for case: HIV-infected patients aged 15 years and older who had documented treatment failure by viral load measurement after at least 6 months on first-line ART and switched to second-line regimen.
Inclusion criteria for controls: HIV-infected patients aged 15 years and above on the first-line ARV whose plasma viral load was <1000 copies/mL in two consecutive viral load measurements after at least 6 months of treatment on the first-line ART regimen.
Exclusion criteria
As study participants, patients who transferred in from other facilities, and who had incomplete recorded data were excluded from the study.
Sample size and sampling procedure
The sample size was calculated by using Epi info version 7.2.2.6 Stat Calc. The known independent factors from a study conducted in Northern Ethiopia, Woldia and Dessie hospitals, Gondar referral Hospital, and Asella hospital were considered to get the maximum sample size for this study. Thus, recurrent diarrhea, current CD4 count less than 200, BMI less than 16, and poor adherence to ART were considered to obtain the maximum sample size. 7 By considering the following parameters; 80% power and at 95% confidence interval (CI), the expected frequency of recurrent diarrhea among those who did not fail first-line treatment 4%, and using a two-population proportion formula the final sample size was 236. By adding 10% as non-respondent, the total sample size was 258 (86 cases and 172 controls) (Table 1). Only Nekemte Specialized Hospital was included in the study among facilities in the town because it is the only facility providing treatment after failure of the first-line regimen, and it is a referral site for the remaining ART clinics. Finally, all cases were included until the required sample was filled but the systematic random sampling (SRS) technique was used to draw controls from the allocated sample from the ART clinic.
Socio-demographic and baseline characteristics of adult HIV patients who were on follow-up at Nekemte Specialized Hospital, western Ethiopia, 1 August–30 September 2019 (n = 252).

HIV: human immunodeficiency virus; ART: antiretroviral treatment; BMI: body mass index; ARV: antiretroviral; d4T: Stavudine; TDF: Tenofovir DF; ETB: Ethiopian Birr; CD: cluster of differentiation; WHO: World Health Organization; Others: amhara, gurage, tigere; AZT: azidothymidine.
SRS for controls were done by K = N/n where; N is the total of adult patients on first-line ARV at facility; n is sample size at the facility. Thus: K = 2002/172 which was 12. Then from list of 1–12, the fourth patient was selected by lottery method. Then data were collected from every 12th patient started from the fourth patients until the required sample size was fulfilled. All cases were included until required sample was fulfilled.
Data collection procedure
Record Review (Medical Record files) of HIV patients was used to identify cases and controls by predetermined criteria of case and control. After cases and controls were differentiated, data were collected from a review of the patient follow-up card and interview of the patient. The data were collected first from cases and then from controls. Two trained health professionals (non-staff of the facility) were recruited for data collection. The questionnaire was developed from different literatures15,18,19,21 and then tested using pilot study for possible modifications. A structured questionnaire and checklist were used for data collection. The questionnaire was prepared in English, translated to Afan Oromo language then back-translated to English by two health workers independently and at different times.
The questionnaire consists of socio-demographic factors (age, sex, residence, ethnicity, marital status, religion, occupational status, educational status, and monthly income); medical factors (CD4 count, WHO stage, BMI, presence of active TB, and CPT); and patient-related factors, such as adherence, alcohol consumption, being in a support group, and disclosure status.
Study variables
The dependent variable was first-line ART failure while independent variables were socio-demographic variables, such as age, sex, educational status, occupational status, income, and marital status; clinical variables such as, CD4 count, WHO stage, BMI, and duration of treatment; behavioral variables, such as alcohol consumption, substance abuse, unsafe sex, and fear of stigma; drug-related variables, such as baseline ARV regimen, regimen discontinuation, regimen substitution, and prior ART exposure; service provision like drug supply, duration of stay in the clinic, availability of clinicians; and other factors like treatment adherence, being in a support group, point of entry to care, disclosure status, and couples treatment status.
Operational definitions
Treatment failure: Two viral load tests shows viral load ⩾1000 copies/mL, performed 3 months apart as per national guideline, before a change of ART regimen. 22
Adherence to ART (good): equal to or greater than 95% adherence, that is, missing only 1 out of 30 doses or missing 2 from the 60 doses. 18
Adherence to ART (poor): less than 85% adherence, that is, missing ⩾5 doses out of 30 doses or >10 doses from 60 doses. 18
Body mass index: BMI was used to describe underweight (BMI < 18.5) and normal (18.5 < BMI < 25.0) in adults.
Disclosure: HIV patients who tell their HIV status to someone who is expected to help them.
Being in a support group: being a member in an association of HIV patients within the facility.
Alcohol consumption: defined as a having history drink alcohol since the start of ART.
Chronic disease: noninfectious diseases like hypertension, diabetes mellitus, congestive heart failure, and renal failure.
First-line ART: the initial regimen prescribed for patients fulfilling national clinical and laboratory criteria for starting ART. Current WHO treatment guidelines recommend two NRTIs and one NNRTI for initial treatment. 23
Second-line ART: is the regimen used immediately after first-line therapy has failed (clinically, immunologically, or virologic). Current WHO treatment guidelines recommend that the PI class be reserved for second-line ART, preferring ritonavir-boosted protease inhibitors supported by two agents from the NRTI class. 23
Data quality management
To ensure the quality of data, a range of mechanisms were employed to address major areas of bias. First, data collectors were trained on how to gather the appropriate information, procedures of data collection techniques, and the whole contents and subject matter of the questionnaire. A week before the actual data collection, the questionnaire was pre-tested on 5% of the sample in Nekemte health center among HIV patients on ART. The purpose of the pre-test was to ensure that the data collectors were familiar with the tools and the respondents were able to understand the questions. Amendments were done accordingly after the pre-test. Data were collected by two trained clinical nurses who had basic training on HIV chronic care and supervised by the principal investigator. Daily, on-site supervision was carried out during the whole period of data collection. At the end of each data collection day, the questionnaire was reviewed and cross-checked for completeness, accuracy, and consistency by the investigator, and corrective discussion was undertaken with the data collectors. Data cleaning was done after it was entered into the software.
Data processing and analysis
Collected data were entered into Epi-Data, version 7.2.2, and then exported to SPSS 25 for analysis. Data cleaning was done before analysis. Cross-tabulations and frequencies were used to summarize descriptive statistics. Binary logistic regression analysis was computed to identify the association between first-line treatment failure and each independent variable. Candidate variables of p value < 0.25 were taken to the final model. All these candidate variables were entered into multivariate analysis with 95% CI to show the strength of association, and p value < 0.05 was used to declare statistical significance. The goodness of fit of the final model was checked using the Hosmer–Lemeshow test of goodness of fit considering good fit at p value ⩾ 0.05, an omnibus likelihood test < 0.05. Multi-collinearity was assessed by a variance inflation factor (VIF) of 1.2.
Ethical consideration
The ethical approval was obtained from Institutional Review Board of Wollega University with the approval number of Ref. No /CHRT/95/2011. Written informed consent was obtained from all the subjects including the legally authorized representatives of minor participants to be enrolled in the study. A permission letter was also secured from facility directors to access the necessary data from patients’ records. Confidentiality of the respondents was ensured as their name was excluded from the data responses.
Results
Socio-demographic and baseline characteristics
Among 258 of the study participants, 252 (86 cases and 166 controls) adult HIV-positive patients on treatment at Nekemte Specialized Hospital were involved in the study, giving a response rate of 98.4% (Table 1).
At baseline, the mean age (standard deviation) for cases and control were 31.41(standard deviation (SD): ±9.24) and 29.77 (SD: ±9.30), respectively. Regarding sex of respondents, 39 (54.7%) of cases and 103 (62%) of controls were males and females, respectively. More than half (54.7%) of cases and the majority 125 (75.3%) of controls were married. Twenty-eight (32.6%) of cases and 23 (13.9%) of controls had no formal education, while 22 (25.6%) and 36 (41.9%) of cases, and 35 (21.1%) and 108 (65.1%) of controls attended primary and secondary schools, respectively (Table 1).
Initially, 37 (43.1%) of cases and 88 (53.1%) of controls started their treatment by Tenofovir-based regimen. Among study participants, 40 (46.5%) of cases started treatment at WHO stage-III, while 86 (51.8%) of controls have initiated treatment regimen at WHO stage-II. Regarding their functional status, the majority (150 (90.4%)) of controls and 60 (69.8%) of cases were working status at baseline. Sixty-two (72.1%) of cases and 150 (90.4%) of controls had normal BMI (⩾18.5 kg/m2) at the time of ART initiation. At baseline, 45 (52.3%) of cases and 138 (83.1%) of controls had CD4 count greater than 100 cells, respectively. After started HIV treatment, 35 (40.7%) of cases and 33 (19.1%) of controls developed and treated for tuberculosis (Table 1).
Treatment-related characteristics of respondents
First-line regimen substitution was happened among 38 (44.2%) of cases and 91 (55.8%) of controls. Among these, 16 (18.6%) of cases and 34 (20.5%) of controls, regimen was changed twice or more by similar line regimen. Moreover, 80 (93%) of cases and 150 (90.4%) of controls had history of Cotrimoxazole prophylaxis therapy and 76 (88.4%) of cases and 156 (94.0%) of controls had history of isoniazid prophylaxis treatment. In this study, 50 (58.1%) of cases and 50 (30.1%) of controls started ART after coming for HIV testing, and after initiation of ARV drug, 46 (53.5%) of cases and 36 (21.7%) of controls interrupted taking their ARV drug. Among those who interrupted their treatment 42 (91.2%) of cases and 18 (85.7%) controls returned to their treatment after discontinuing for about 1 month or more. About 17 (19.8%) of cases and 21 (12.7%) of controls missed their appointment while taking their medications and about three-fourth (75.5%) of cases and the majority of controls (94%) had good adherence status to their ARV medication (Table 2).
Treatment-related characteristics of HIV-infected patients on treatment at Nekemte Specialized Hospital, western Ethiopia, 1 August–30 September 2019 (n = 252).

ART: antiretroviral treatment; INH: isoniazid; TB: tuberculosis; BMI: body mass index; HIV: human immunodeficiency virus; VCT: voluntary counseling and testing for HIV; PITC: provider-initiated testing and counseling; ARV: antiretroviral; CD: cluster of differentiation.
Behavioral, attitude, and other characteristics of respondents
During the start of treatment, 59 (68.6%) of cases had partner and 54 (91.5%) of them disclosed their HIV status to their partner. Similarly, 144 (86.7%) of controls have partner and 141 (97.9%) of them disclosed their HIV status to their partner. Concerning HIV treatment disclosure, 58 (67.4%) of cases and 154 (92.8%) of controls disclosed as they are on HIV treatment to their family or relatives. Among couples who were HIV positive, 26 (59.1%) of cases and 68 (67.3%) of controls have initiated ARV with their partner. Thirty-eight (44.2%) of cases and 107 (64.5%) of controls had participated in support group association of HIV patients. During early treatment initiation, 30 (34.9%) of cases, and 24 (14.5%) of controls were worried about peoples’ feeling toward them. Regarding substance abuse, 14 (16.3%) of cases and 19 (11.4%) controls were abused to one of the substances (alcohol, khat chewing, or smoking). Condom was used by 39 (45.3%) of cases and 101 (60.8%) of controls during sexual intercourse (Table 3).
Behavioral, attitude, and patient-related characteristics of HIV patients on HAART at Nekemte Specialized Hospital, western Ethiopia, 1 August–30 September 2019 (n = 252).
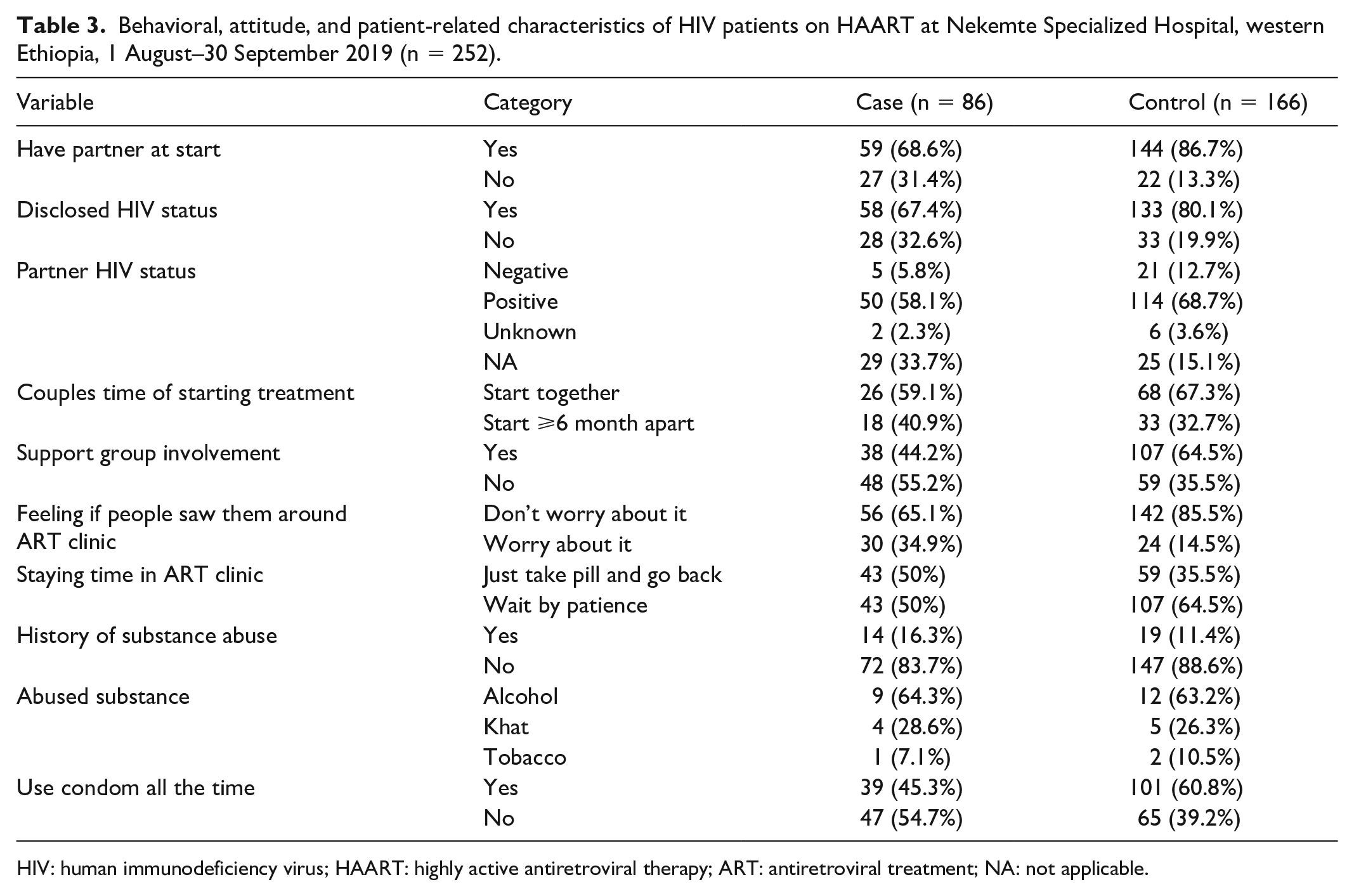
HIV: human immunodeficiency virus; HAART: highly active antiretroviral therapy; ART: antiretroviral treatment; NA: not applicable.
Determinants of first-line treatment failure among adults on ART
After all variables in the study were entered into a binary logistic regression to identify candidate variables for multivariate analysis, some variables were selected being potential candidates at p value < 0.25. These were residence, baseline WHO, baseline BMI, current BMI, baseline CD4 count, baseline functional status, initial ARV regimen, tuberculosis infection after ART started, HIV status disclosure, history of ART discontinuation, duration of ART discontinuation, adherence status to ART, participate in a support group of HIV patients, feeling about stigma and discrimination, and willingness to stay in ART clinic were potential candidates for multiple logistic regression analysis.
To control possible confounders, all candidate variables were included in multivariate logistic regression analysis using backward likelihood ratio model (LR); it was found that baseline WHO stage, baseline CD4 count, history of HIV treatment discontinuation, participation in a support group association, and adherence level to ART treatment had a statistically significant association with first-line treatment failure (p value < 0.05; Table 4).
Factors associated with first-line treatment failure in Nekemte Specialized Hospital, western Ethiopia, 1 August–30 September 2019 (n = 252).

ART: antiretroviral treatment; HIV: human immunodeficiency virus; WHO: World Health Organization; CD: cluster of differentiation; ARV: antiretroviral treatment; BMI: body mass index; TDF: Tenofovir DF; AOR: adjusted odd ratio; AZT: azidothymidine; COR: crude odd ratio; CI: confidence interval.
1 = reference category ** = statistical significant association.
The odd of treatment failure among patients who started treatment at WHO stage 3 or 4 at baseline was 3 times (adjusted odds ratio (AOR) = 2.96, 95% CI: 1.50, 5.86) more likely to occur when compared with those who started treatment at WHO stage I/II. The study also revealed that the odds of first-line treatment failure was 3 times more (AOR = 3.21, 95% CI: 1.55, 6.62) in those whose baseline CD4 count was <100 cells/mm3 compared with those whose CD4 count ⩾100 cells/mm3 at baseline. The risk of developing first-line treatment failure was 2.54 times (AOR = 2.54, 95% CI: 1.27, 5.09) more among those who returned to ART treatment after discontinuation compared to those who had no history of ART discontinuation (Table 4).
Besides, the odd of first-line treatment failure was 3.35 times (AOR = 3.35, 95% CI: 1.68, 6.64) more among those who are poorly adherent to their ART treatment when compared to those who had good adherent to their ART treatment. The study also revealed that those who did not participate in the HIV association were 4.53 times (AOR = 4.53, 95% CI: 2.27, 9.04) more likely to develop treatment failure than those who participated in the HIV association (Table 4).
Discussion
Early identification and management of HIV treatment failure is the backbone for prevention of newly emerging drug-resistant HIV and unnecessary shift of more toxic second-line ARV regimen. This study was aimed to assess determinants of treatment failure among patients on first-line ARV treatment and showed that Baseline WHO stage (stage III or IV), Baseline CD4 count (<100 cells/mm3), lack of participation in a support group, interruption of ART and poor Adherence to ART was found to have higher odds of first-line ARV treatment failure.
In this study, the odds of first-line treatment failure were 2.96 higher among advanced WHO stage (stage 3 or 4) than WHO stage I/II (AOR = 2.96, 95% CI: 1.50, 5.86). Studies from other countries of similar setting like Zimbabwe, 24 Mozambique, 25 and Swaziland 26 also revealed that odds of first treatment failure was higher among patients whose baseline WHO clinical stage was III or IV. Other studies in the same country (Arba Minch public health facilities, and Northern Oromia) similarly reported that treatment failure was more among those who started treatment at WHO stage 3 or 4 than those initiated at stage 1 or 2.27,28 This could be due to a delay in ART initiation which leads to high viral load and declined CD4 cells thus; increased risk of concomitant opportunistic infection which causes pill burden with ARV drug. However, the current Ethiopian ART guideline expanded to treat all HIV-positive patients. This will minimize delay in HAART initiation but a delay in diagnosis is a remaining problem. 29
Lower CD4 count (<100 cells/mm3) at the time of ART initiation had a significant association with first-line treatment failure. The odds of first-line treatment failure were 3.12 times higher among patients who started ART at lower CD4 count than their counterparts (AOR = 3.12, 95% CI: 1.55, 6.62). This finding is in agreement with the study from Kenya, 30 and several other studies in Ethiopia including studies in Northeast Ethiopia, 7 Bale zone, 31 Arsi University, 32 and Bahir-Dar referral Hospital, 33 in which low baseline CD4 cells was a predictor of HAART failure among adults on first-line ARV regimen.
This study also revealed that patients who discontinued ART and returned to treatment were 2.5 times likely to develop first-line treatment failure (AOR = 2.54, 95% CI: 1.27, 5.09) than those who did not interrupt their treatment. Similar findings were being reported in some African countries like Zimbabwe, 24 Tanzania, 34 Southeast Ethiopia, 32 and Kuyu hospital of Northern Ethiopia. 28 At the time of drug interruption, the viral rebound is at a high level and production of the mutant viral gene will occur which in turn develop resistance to ARV drugs.
In this study, the odds of treatment failure were four times higher among patients who did not participate in a support group (AOR = 4.53, 95% CI: 2.27, 9.04). This finding was supported by a study conducted in Tanzania, 34 and Zimbabwe, 35 in which belonging in a support group minimize the risk of getting ART failure, whereas, the HIV patients in Nepal, 36 have the chances of attending clinics regularly because of having support group which increase their knowledge about ART regimens. This could be due to the support group association is the place where HIV patients got adherence support, discuss their psychosocial problems as well as drug- and HIV-related myth with their fellow which is led by expert patients. 34 When patients did not involve in support groups, these all problems will remain unsolved.
This study identified that the odds of treatment failure were three times (AOR = 3.35, 95% CI: 1.68, 6.64) higher among patients who were poor adherent to their treatment than those patients who had good adherence. The finding was consistent with a report from an African virology study; in western Kenya among African patients reported that poor adherence is an independent risk factor for treatment failure. 37 A similar result was also gained from a study from Zimbabwe that showed the odds of treatment failure is about three times higher among those poorly adherents to their ARV medications. Accordingly, the study done in Northeastern Ethiopia Woldia and Dessie referral hospital reported the odd of treatment failure was higher among those who were poorly adhered to their ART, 7 and cohort study from Adama General Hospital Medical college of Central Ethiopia also found that poor adherence is one of the independent factors for first-line treatment failures among HIV patients. 38 This is pharmacologically possible as poor adherence results in drug dosage below the level necessary to produce a therapeutic effect; thereby enabling the development of drug-resistant genes. It is evident that patient who misses three doses per month is associated with drug resistance and declined immunity and then it makes a loss of opportunity for ART to suppress viral replication which leads to treatment failure. 39
Conclusion
First-line treatment remains the worsening problem among ART users because of the development of new drug-resistant HIV cells. Therefore, early identification and taking effective action against the associated factor is very crucial. This study showed that low CD4 cells, late ART initiation (stage 3 or 4), lack of participation in a support group, ART interruption, and poor adherence to ART were significantly associated with first-line treatment failure. Thus, the test and treat program should be strengthened as it minimizes starting treatment at the advanced WHO stage. Specific patient counseling on the problem with ARV discontinuation and early tracing of patients who discontinued ART should be strengthened. Efforts should also be done to improve adherence of patients to HAART to boost immunity and for enhancement of positive life support. Baseline viral load determination should also be done for new patients. It would be beneficial if genotyping of newly diagnosed treatment failure and new patients are started.
Limitation of the study
This study did not include a baseline viral load because of the unavailability of the test in the facility. There may be also a potential for recall bias as questions related to HIV and treatment history were obtained from the patient interview. We also did not know time period of switch from first-line to second-line ART regimens since our study design is not cohort.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211030182 – Supplemental material for Determinants of first-line antiretroviral treatment failure among adult HIV patients at Nekemte Specialized Hospital, Western Ethiopia: Unmatched case-control study
Supplemental material, sj-pdf-1-smo-10.1177_20503121211030182 for Determinants of first-line antiretroviral treatment failure among adult HIV patients at Nekemte Specialized Hospital, Western Ethiopia: Unmatched case-control study by Mengistu Desalegn, Dejene Seyoum, Edosa Kifle Tola and Reta Tsegaye Gayesa in SAGE Open Medicine
Footnotes
Acknowledgements
The authors are very grateful to Wollega University for providing them the necessary support to undertake this study. They also thank the Nekemte town health bureau and ART clinic staffs at Nekemte Specialzed Hospital for their unreserved cooperation by providing them all the necessary information during the data collection period. Finally, they thank all study participants for their willingness to be enrolled in this study.
Authors’ contributions
M.D. and D.S. had substantial contribution for the design and concept of the preliminary study; E.K. and L.T. supported in the data collection, analysis, and interpretation; E.K. and L.T. has prepared the drafts of the manuscript; D.S. and M.D. helped the study in revising the drafts of the article for the important intellectual content. Finally, all authors have read and approved the final version of the article to be published, and all of the authors are equally accountable for all aspects of the work, as well.
Authors’ declaration
The ethical approval was obtained from institutional review board of Wollega University with Ref. No /CHRT/95/2011 prior to study initiation. Written informed consent was obtained from all the subjects including the legally authorized representatives of minor participants to be enrolled in the study. This research is our original work and that all sources of materials used for this paper have been duly acknowledged. Also this work has not been submitted to any other university for achieving any academic degree or diploma awards.
Availability of data and materials
The data analyzed during the study are available from the corresponding author up on formal request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval with Ref. No /CHRT/95/2011 for this study was obtained from the Institutional Review Board of Wollega University.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all the subjects including the legally authorized representatives of minor participants prior to study initiation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.