
Abstract
Background:
Antiretroviral treatment failure occurred when the antiretroviral regimen is unable to control HIV infection. There is no information on antiretroviral therapy failure in this study area.
Objective:
The aim of this study was to assess the magnitude and associated factors of antiretroviral therapy failure among HIV-positive adult patients in Harar public hospitals from January to February 2018.
Methods:
An institution-based cross-sectional study was conducted using chart review data from February 2005 to July 2017. Systematic sampling technique was used to include a sample of 1094 patient charts. Data were analyzed by Statistical Package for Social Sciences version 20.0. Statistical significance was considered at p < 0.05.
Results:
The prevalence of first-line antiretroviral treatment failure was 21% (95% confidence interval = 18.3–23.5). Being male in sex, age of 45–54 years, patients with World Health Organization stages 3 and 4 during antiretroviral therapy initiation, a baseline CD4 count <100 cells/mm3, poor drug adherence, and on antiretroviral therapy follow-up for ⩾25 months were predictors of antiretroviral treatment failure.
Conclusion:
In this study, the rate of antiretroviral treatment failure is relatively high. Therefore, the concerned body should pay attention to the predictors to reduce the risk of treatment failure among this study group.
Background
Acquired immunodeficiency syndrome (AIDS) is a global epidemic disease which is caused by a virus called human immunodeficiency virus (HIV). About 70% of all people living with HIV (PLWHIV) are in sub-Saharan Africa. In Ethiopia, antiretroviral (ARV) treatment began in 2003, and free antiretroviral therapy (ART) was launched in 2005. ART has reduced HIV-related morbidity and mortality at all stages of HIV infection, reduced HIV transmission and improved the patient’s quality of life.1–3
All HIV-infected adults and adolescents started ART when their CD4 count was ⩽500 cells/mm3 irrespective of the World Health Organization (WHO) clinical stage, WHO clinical stages 3 and 4 irrespective of CD4 cell count, active tuberculosis disease irrespective of CD4 cell count, all HIV-positive pregnant and breastfeeding women irrespective of CD4 count and all HIV-infected partners of sero-discordant couple regardless of CD4 cell count (to reduce the risk of HIV transmission to the negative partner). First-line ART regimen is recommended, which is simplified and less toxic, and more convenient regimens as fixed-dose combinations are available. Once-daily regimens comprising nucleoside reverse transcriptase inhibitor (NRTI) backbone (TDF + 3TC) and one non-nucleoside reverse transcriptase inhibitor (NNRTI) (EFV) are maintained as the preferred choices in adults, adolescents and children older than 10 years. Based on the national ART treatment guideline, CD4 count is performed every 6 months, and most of the time viral load test is performed, treatment failure is suspected. But in the absence of viral load test treatment, failure has been assessed using clinical and immunological criteria.1,2,4
The identification and management of first-line ART failure is a key challenge for HIV programs in resource-limited setting. Staying on a failing first-line therapy is associated with an increased risk of mortality. 4 The patients who have failed first-line drug therapy are 46% more likely to fail second-line drug therapy and have greater likelihood of experiencing drug resistance. 5
To increase the success rate of ARV combination therapy substantially, there is an urgent need to know the prevalence and understand better the factors associated with treatment failure. This kind of study has been conducted in other different areas; however, there are very limited studies in our country—in particular, there is no study conducted in this study area. Therefore, this study was used to generate evidence on the magnitude and associated factors of ART failure among adult HIV-positive patients on ART.
Materials and methods
Study area and period
This study was conducted in Harar region. Harar is one of the nine regional states found in the eastern part of Ethiopia at a distance of 525 km from Addis Ababa. In the region, there are 2 public hospitals, 1 federal police hospital, 2 private hospitals, 4 urban and 3 rural health centers, and 33 private clinics. 6 Based on the National HIV AIDS Multi-Sectoral Response of the 2016 Annual Joint Review report conducted in Adama, the 2016 adult HIV prevalence in Harar region was 2.95%. 7 This study was conduct from January to February 2018.
Study design and population
An institution-based retrospective cross-sectional study design was used. All records of adult HIV-positive patient whose age was >15 years at the time of ART initiation and who have ever started ART in the study area and have been taking ART for >6 months in the facilities from February 2005 to July 2017 were included. Transfer of patients from other health facility and incomplete charts or records were excluded.
Sample size determination and sampling procedure
The sample size was estimated using single population proportion formula by considering the prevalence of ART failure (37%) from the previous study conducted in Asella Referral Hospital, 8 with 95% confidence interval and 0.03 degree of precision. The final sample size including 10% non-response rate was 1094. The total study populations were allocated proportionally to each hospital. Based on this, 761 participants were recruited from Hiwot Fana Specialized University Hospital and 333 from Jugal Hospital. A lottery method was applied for first sample selection and then every fifth was selected until the sample size was reached. There are only two government hospitals in the region, and both of them were included to make it representative.
Data collection instruments and procedure
Data were collected using structured questionnaires adopted from previous literature.2,4,9 The data extraction tool is prepared in English and there was no need for translation. Medical record and registers of patients on ART in Hiwot Fana Specialized University Hospital and Jugal Hospital were used as a source of data. When the patient enrolled to the care, all the details were entered on patients’ charts and electronic database before ART and during ART.
Data quality control
Although the data collectors were familiar with all the information in the data collection instrument, training was given for 2 days before the data collection started. Before the actual data collection process, the data collection instrument was pretested in Haramaya Hospital with 5% (55) of the total sample size. The necessary modifications and corrections were made on the checklist before it was finally administered into the study area. The pretested questionnaires were not used in the main data and rather used to test the feasibility of the instrument and enabled in modifying few of the information in the original instrument. Double data entry was done by two separate data entry workers.
Data processing and analysis
The collected data were sorted, coded and double entered into EpiData version 3.1 software and exported to SPSS version 20.0 for cleaning and data analysis. Variables with p ⩽0.25 in bivariate analysis were considered as candidates for multivariable logistic regression. A value of p < 0.05 was declared as statistical significance. ARV treatment failure is defined as progression of disease and high risk of mortality after beginning highly active antiretroviral therapy (HAART). This can be diagnosed by clinical, immunological, or virological failures 6 months after ART initiation as per the recommendation in the national and WHO guidelines. 2
Results
Socio-demographic characteristics and social condition
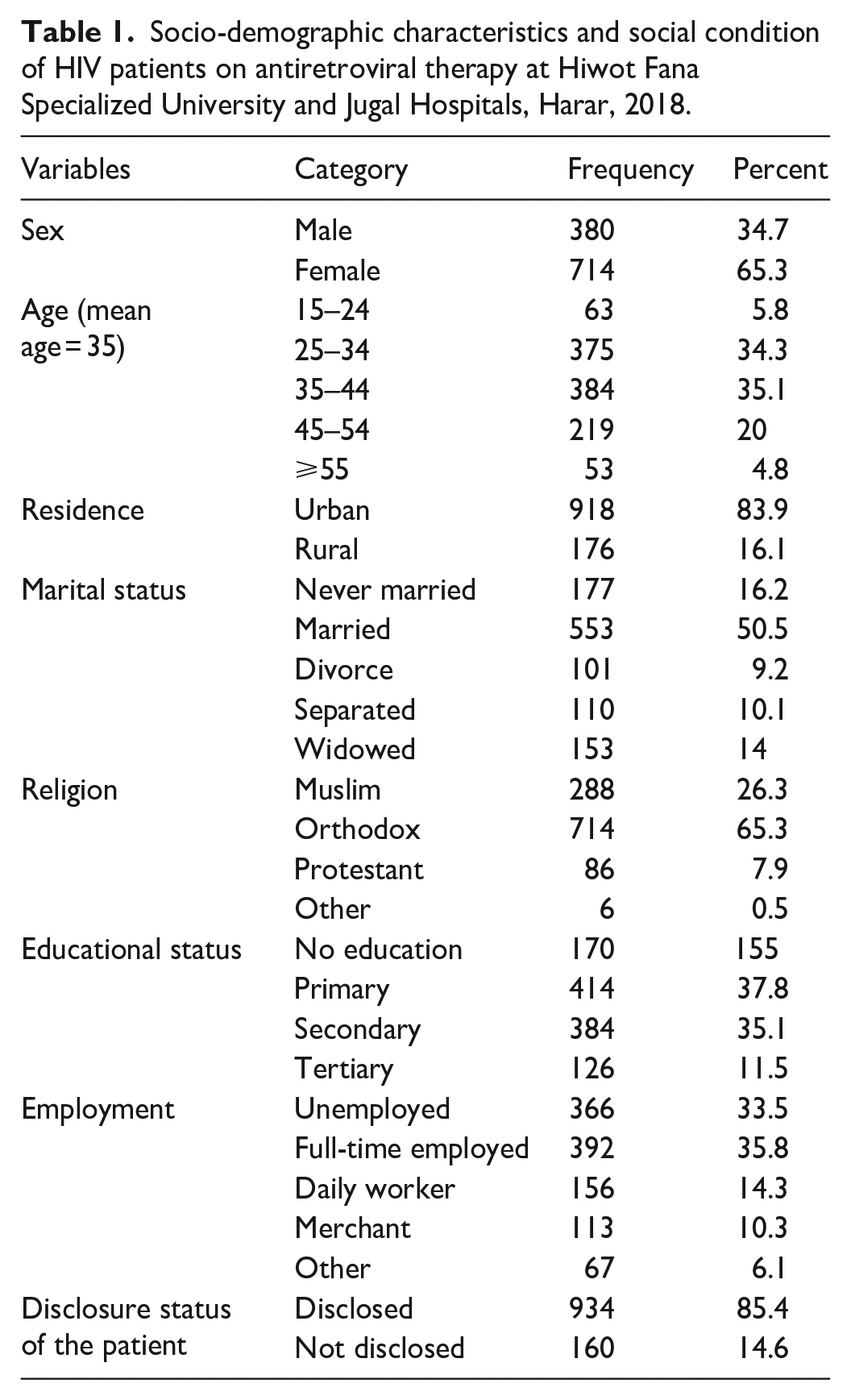
A total of 1094 adult patients on HAART chart registration and electronic database were reviewed from February 2005 to July 2017. The mean age of the patients at the start of ART was 35 ± 4 years. Of the total patients, 714 (65.3%) were females and 918 (83.9%) were from urban residence (Table 1).
Socio-demographic characteristics and social condition of HIV patients on antiretroviral therapy at Hiwot Fana Specialized University and Jugal Hospitals, Harar, 2018.
Clinical conditions of the study participants
Seven hundred three (64%) study participants started ART based on CD4 eligibility criteria and 670 (61%) were initiated with efavirenz-based first-line ART. Restarting first-line ART after interruption was observed in 205 (19%) patients. Excluding regimen change due to treatment failure, 445 (41%) patients had history of regimen change due to toxicity, pregnancy, new tuberculosis and new drug availability (Table 2).
Clinical conditions of the study subjects at initiation of ART and during the follow-up period in Hiwot Fana Specialized and Jugal Hospitals, Harar, January–February 2018.

ART: antiretroviral therapy; NNRTI: non-nucleoside reverse transcriptase inhibitor; NRTI: nucleoside reverse transcriptase inhibitor; INH: isoniazid.
On ART initiation, the weight of 664 patients (60.7%) were >50 kg, with a mean weight of 54 kg. Relative to the weight at initiation of ART, the change in weight after 6 months of ART follow-up was positive with a mean weight change of 3 kg. Based on the baseline CD4 count, 832 (76.1%) had a CD4 count >100 cells/mm3, with a mean count of 176 cells/mm3 (Table 3).
Clinical condition of the study subject from the time of ARV enrollment to chronic HIV care until the last ART visit in Hiwot Fana Specialized University and Jugal Hospitals, Harar, 2018.
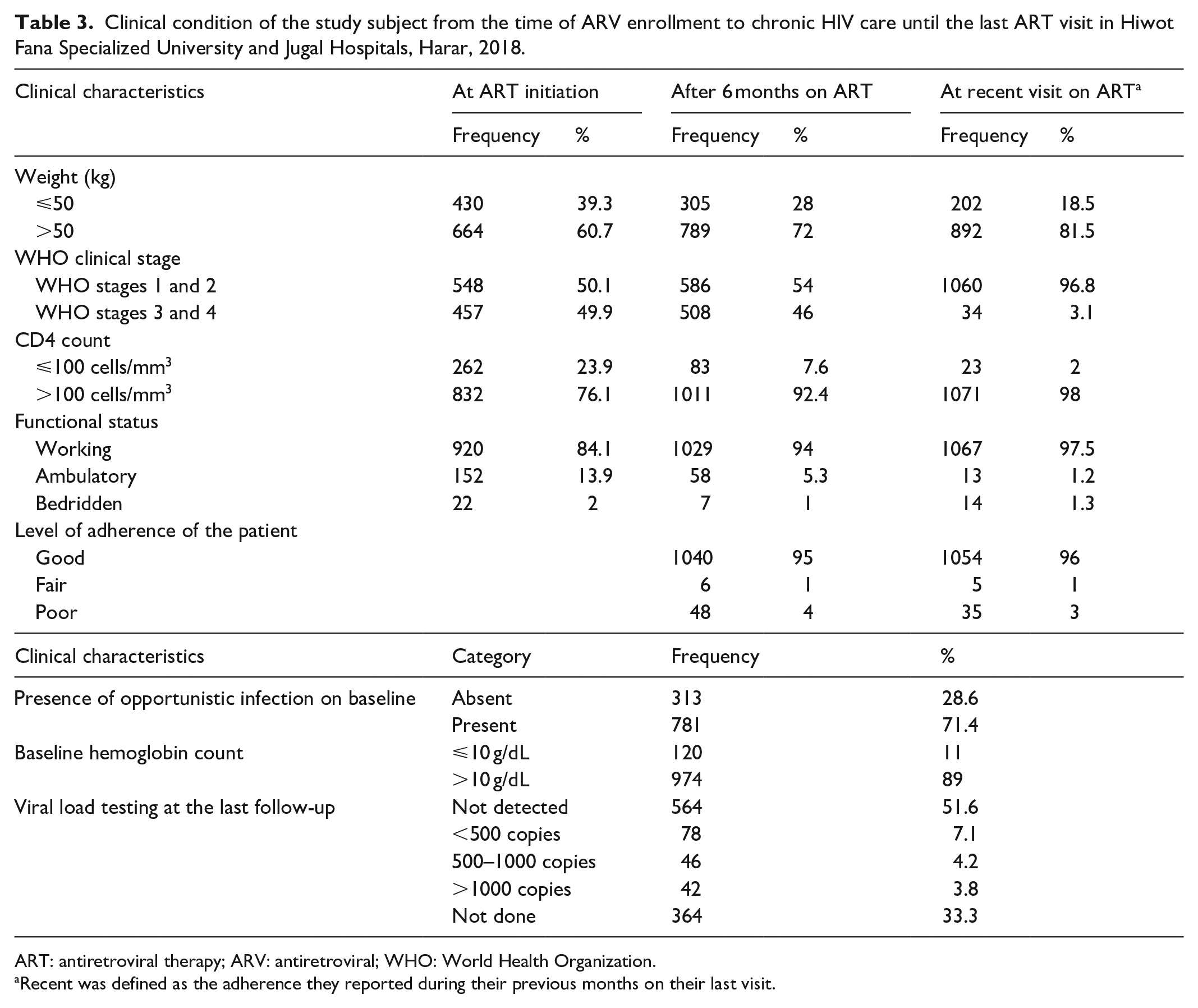
ART: antiretroviral therapy; ARV: antiretroviral; WHO: World Health Organization.
Recent was defined as the adherence they reported during their previous months on their last visit.
Prevalence of ARV treatment failure
The overall prevalence of ART failure was 231 (21.1%) (Figure 1). Among participants with failure, 154 (18.6%), 32 (3.2%) and 40 (3.7%) had immunological, virological and clinical failure, respectively. One hundred fifty-eight (74%) failures had occurred among clients who were on ART for >48 months. The mean time for the occurrence of failure was 71 months (Figure 2).

Diagrammatic presentation of the occurrence of first-line ART failure among the study subjects in Harar Hiwot Fana Specialized University Hospital and Jugal Hospital, 2018.

Duration of the occurrence of first-line ART failure among study subjects in Hiwot Fana and Jugal Hospitals.
Factors associated with ARV treatment failure
In bivariate analysis, ART failure was more prevalent in male patients; patients aged 46–55 years; patients infected with opportunistic infection at baseline; weight on ART initiation <50 kg; WHO clinical stages 3 and 4 on ART initiation; patients who were ambulatory and bedridden by their functional status; baseline CD4 count <100 cells/mm3; length of follow-up of 49–60 months, >60 months and 49–60 months; level of adherence after 6 months of ART initiation being fair and poor; and treatment interruption and restart during the follow-up period (Table 4).
Factor associated with ART failure in multivariate logistic regression analysis among ART clients in Hiwot Fana Specialized University and Jugal Hospitals, Harar, 2018.

ART: antiretroviral therapy; WHO: World Health Organization; CI: confidence interval; AOR: adjusted odds ratio.
Significant at p < 0.25 for bivariate analysis.
Statistically significant p < 0.05 for multivariate analysis.
All independent variables that have an association with the outcome in bivariate analysis models were included in the multivariate regression model. Finally, being male in sex (adjusted odds ratio (AOR) = 1.6, 95% confidence interval (CI) = 1.09–2.34), age range 45–54 years (AOR = 2.4, 95% CI = 1–5.4), baseline WHO clinical stages 3 and 4 (AOR = 2.04, 95% CI = 1.36–3.07), baseline CD4 count <100 cells/mm3 (AOR = 2.7, 95% CI = 1.77–3.98), drug interruption (AOR = 6.9, 95% CI = 4.1–11.9), and being on ART for a long period of 25–48 months (AOR = 3, 95% CI = 1.4–6.9), 49–60 months (AOR = 3.9, 95% CI = 1.5–10) and >60 months (AOR = 5.5, 95% CI = 2.5–12) were more likely to develop treatment failure compared to their counterparts (Table 4).
Discussion
In this study, the prevalence of first-line ART failure was 21%, which is similar to the prevalence of ART failure reported in Debre Markos Hospital, Northwest Ethiopia. 9 This is higher than the prevalence reported in the study conducted in India at government general teaching hospital, where the prevalence of first-line ART failure was 0.47%; 10 in Gondar Teaching University Hospital, 4.1%; 4 and Bale Zone Dolomena Hospital, 6.47%, 11 but lower than the prevalence reported in Asella Referral Hospital, that is, 37%. 8 The difference in prevalence may be due to the difference in study setting where the systematic review was conducted. 9 Prevalence of treatment failure need not be uniform all over the country; it may be heterogeneous and may vary from region to region or states, so it is desirable to estimate the prevalence of treatment failure at frequent intervals. 10 The difference in prevalence might be due to difference in the study area or location and methodology.
Although the proportion of females on ART is higher than males in this study, the prevalence of ART failure was highest in males. This finding is similar to the study conducted in India. 10 And in the study conducted in Ethiopia Bale Zone of South Eastern Ethiopia, it was found that males were 4.49 times more likely to experience treatment failure compared to females; the possible reason could be the difference in mean CD4 count between males and females during ART initiation and also unhealthy behaviors in males such as using alcohol, cigarette and khat than females, leading to poor adherence and reduction in treatment success. 11
The mean age in this study (35 years) is almost equivalent to the median age of 35 years as reported in the study conducted in Ethiopia. 9 The reason for finding relatively young and middle-aged patients in this study might be due to the fact that 84% of the study subjects lived within the urban region where access to information and health service is relatively good. There is a relationship observed between age of the patient and ART failure. Patients whose age ranged 45 from 54 years had higher ART failure. This is relatively similar the previous report of the study performed in Burkina Faso; this could be explained by the deficit in immune reconstitution functions, which gradually increases with age. 12 This was also supported by the study conducted in Bale Zone, which showed that the risk of treatment failure increased 2.91 times in older ART clients. 11 The reason for failure among those could be associated with diminished immunity due to age and long stay on treatment. Also, those who received ART drug for long duration (⩾25 months of ART duration) were significantly associated with treatment failure. Those who took drug for long duration of time may develop drug side effects and resistance easily. Previous study also supports this finding. 13
Patients who were on WHO stages 3 and 4 during initiations of ART have higher odds of treatment failure. This result is similar to the study reported from Southern Ethiopia. 14 This might be due to the higher rate of morbidity associated with the inability to identify failures early and switch to second-line regimen.
This research identifies that patients with baseline CD4 count of <100 cells/mm3 have higher odds of first-line ART failure, which is in line with studies conducted in Ethiopia at Debre Markos Hospital, 9 Addis Ababa public hospitals, 15 Bale Zone hospitals 11 and Gondar Teaching University Hospital. 4 This is also supported by the study conducted on African patients that showed low baseline CD4 cell count <50 cells/mL leads to hazardous failure 16 and the study conducted in Burkina Faso that identifies that CD4 level <200/mm3 at treatment initiation develops treatment failure. 12 This might be due to the fact that patients with baseline CD4 count ⩽100 cells/mm3 are at lesser immunity. 9
In this research, among patients identified as failure, 87% of them switched to second-line ART; the remaining 13% of patients who developed failure to first-line regimen were not switched to second-line ART. This shows that patients who fail first-line regimen are not timely switched to second-line regimen. A research showed that those individuals who remained on first-line therapy after failure had a higher probability of dying than those who had switched. 17 Delaying in switching to second-line treatment is not only associated with death but is also associated with deteriorating immunological status of the patients, which exposes them to opportunistic infections, risk of developing resistance and potential transmission to partners. 18 The reason for not being timely switched to second-line treatment might be due to the less attention given to diagnose treatment failure and lack of trained manpower to pick and manage treatment failures early.
The strength of this study was the use of large sample size that helped to assess factors which are not found in the reviewed literature. But the limitation of the study is that prevalence of failure could be underestimated because the study uses data collected retrospectively in patient charts.
Conclusion
In this study, there was a high prevalence of first-line ART failure, that is, 21%. A baseline CD4 count <100 cells/mm3, interrupting first-line ART for some time and restarting the first-line ART, age of the patient 45–54 years, being male in sex and individuals with WHO stage 3 and 4 conditions at the initiation of ART were the main predictors of ART failure. Special focus should be given on building the capacity of health care providers working on ART clinics for early recognition and management of treatment failure.
Footnotes
Acknowledgements
First, we thank College of Health and Medical Sciences, Haramaya University for giving us the chance to conduct this study. We would also express our deepest gratitude to ART clinics of the two hospitals and all individuals and organizations that supported us in conducting this study.
Author contributions
R.F., K.T.R, B.G. and F.W. designed the study, participated in data collection, analysis, interpretation, and write-up, drafted the manuscript, and critically revised the manuscript.
Availability of data and materials
All the necessary data supporting our findings are contained within the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted after approval of ethical clearance from the Institutional Research Ethics Review Committee of Haramaya University with reference number C/AC/R/D/01884/18. An official support letter was given to Hiwot Fana Specialized University Hospital and Jugal Hospital. Institutional consent was obtained by communicating to Regional Health Bureau and respective hospitals before conducting the study. Finally informed consent from the client was waived by Haramaya University Institutional Review Ethics Committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Haramaya University post-graduate directorate.
Informed consent
Institutional consent was obtained by communicating to Regional Health Bureau before conducting the study. Informed consent of the health facility medical directors was also obtained.