
Abstract
Background:
Existing evidence indicates an increasing burden of puerperal sepsis in sub-Saharan Africa. Across the world, due to a lack of self-care practice and less attention to puerperal sepsis, postpartum women are exposed to major disorders and life-threatening conditions, leading to a lower quality of life. Therefore, this study aimed to assess the knowledge of puerperal sepsis and self-care practices related to the prevention of puerperal sepsis.
Methods:
A facility-based cross-sectional study was conducted among 422 postpartum women in Gurage zone public hospitals from July to August 2024. A systematic sampling technique was employed to get the representative sample. Bivariate and multivariable logistic regression were done to identify factors associated with outcome variables; a p-value <0.05 was considered statistically significant.
Result:
In this study, the response rate was 98.8%. The overall good knowledge and self-care practice were found to be 40.8% (95% confidence interval (CI): 36, 46) and 29.3% (95% CI: 25, 34), respectively. Educational status (Adjusted odds ratio (AOR) = 1.13; 95% CI: 1.10, 2.85 and AOR = 2.1; 95% CI: 1.64, 5.43), occupation (AOR = 2.01; 95% CI: 1.2, 3.4), and antenatal care (ANC) contact (AOR = 1.3; 95% CI: 1.23, 2.97) were associated with knowledge of puerperal sepsis. Multiparous (AOR = 1.2; 95% CI: 1.04, 3.14), ANC contact (AOR = 1.27; 95% CI: 1.15, 2.81), and knowledge (AOR = 4.3; 95% CI: 2.14, 9.31) were factors associated with the self-care practice of puerperal sepsis prevention.
Conclusions:
This finding showed that 70.7% of postpartum women lacked good self-care practices of puerperal sepsis prevention. Hence, counseling and enhancing their knowledge of self-care practices should be provided to women to increase their awareness regarding puerperal sepsis prevention and self-care.
Introduction
The World Health Organization defined puerperal sepsis as a life-threatening condition due to organ dysfunction resulting from infection during pregnancy, childbirth, post-abortion, or the postpartum period.1,2
Puerperal sepsis is manifested by pelvic pain or abdominal tenderness, fever, offensive vaginal discharge, and delayed uterine involution. 1 History of pelvic infection, intra-amniotic fluid procedures, prolonged rupture of membranes, wound hematoma, retained products of conception and their removal, multiple vaginal examinations, length of labor, and mode of delivery are contributors to the occurrence of puerperal sepsis.3,4
It is among the leading causes of maternal mortality worldwide and is a preventable cause of maternal morbidity and mortality in both developing and developed countries.4 –6
In addition to morbidity and mortality, puerperal sepsis causes long-term health problems such as pelvic infection and infertility if not recognized and treated early.1,7,8 It not only endangers the mother’s well-being but also leads to financial burdens due to management costs, including hospital stays and medications. Moreover, when mothers suffer from puerperal sepsis, they are unable to care for their infants, which increases the occurrence of early neonatal loss.9,10
Globally, an estimated 287,000 maternal deaths occur annually, with 70% in sub-Saharan Africa; around 11.5% of these deaths are due to puerperal sepsis. 11 In developing nations, puerperal sepsis remains a leading cause of maternal morbidity and mortality, accounting for 15% of maternal deaths.12 –14
Across the African countries, the prevalence of puerperal sepsis ranges from 2% to 24%,15 –19 often leading to surgical intervention, multi-organ failure, and death. 4 Evidence shows that sepsis requires urgent medical attention, early treatment, and resuscitation. Health providers should give careful attention to the diagnosis of sepsis to prevent unexplained end organ damage in the presence of infection, regardless of fever, and treatment should begin within an hour for life-saving outcomes. 6
Previous findings indicate that the majority of postnatal mothers had poor knowledge of the prevention of puerperal sepsis.20 –23 Beyond healthcare provider interventions, women’s self-care plays a crucial role in promoting well-being during the postnatal period. Maternal self-care is the mother’s capability to care for herself, including proper nutrition, exercise, rest, hygiene, and physical appearance.24,25 However, current evidence shows that postnatal women generally have poor self-care practices for the prevention of puerperal sepsis. Around three-quarters of postnatal women demonstrated poor self-care practices.20 –23,26
A study conducted in Egypt found that fewer than 66.7% of participants had poor knowledge of puerperal sepsis, and more than half reported poor self-care practices. 21 Similarly, in Bangladesh, both knowledge and self-care practices regarding puerperal sepsis were poor. 22 In addition, in Tanzania, 37.9% of women had poor knowledge, and 88.6% had poor self-care practices. 23 Likewise, in Ethiopia, a study in Arba Minch revealed that 54.4% of postnatal mothers had poor self-care regarding puerperal sepsis prevention. 26
In Ethiopia, the maternal mortality ratio reduced from 401 in 2017 to 267 in 2020; however, accelerated progress is still needed to reach the 2030 target of 70 per 100,000 live births, as about 12,000 mothers are lost every year. Moreover, 13% of these deaths are attributed to puerperal sepsis.12 –14,27,28
Ethiopia aims to reduce maternal mortality to 199 per 100,000 by 2026 and to achieve the Sustainable Development Goal of 70 per 100,000 by 2030, by reducing 82% of direct causes, including puerperal sepsis. 29 Hence, to achieve this plan and speed up the reduction of maternal mortality, it is essential to address the contributors to maternal morbidity and mortality. This study is based on the indicated gaps and limited evidence in the country in identifying women’s knowledge of puerperal sepsis and the lack of self-care practice of puerperal sepsis prevention, which contribute to maternal morbidity and mortality.
The outcome of our findings will provide circumstantial evidence to guide maternal health education, strengthen infection prevention strategies, and inform policymakers in designing interventions to reduce maternal morbidity and mortality in resource-constrained countries like Ethiopia. Therefore, this study aimed to assess knowledge of puerperal sepsis, self-care practices for puerperal sepsis prevention, and associated factors among postpartum women in Gurage zone, Central Ethiopia.
Objective of the study
To assess the knowledge of puerperal sepsis, self-care practices for puerperal sepsis prevention, and associated factors among postpartum women in Gurage zone public hospitals, Central Ethiopia, 2024.
Research questions
What is the knowledge level of puerperal sepsis among postpartum women in Gurage zone public hospitals, Central Ethiopia?
What are the factors associated with knowledge of puerperal sepsis among postpartum women in Gurage zone public hospitals, Central Ethiopia?
What are the self-care practices for puerperal sepsis prevention among postpartum women in Gurage zone public hospitals, Central Ethiopia?
What are the factors associated with self-care practices for puerperal sepsis prevention among postpartum women in Gurage zone public hospitals, Central Ethiopia?
Methods and materials
Study setting and period
A facility-based analytical cross-sectional study was conducted in Gurage zone public hospitals, Central Ethiopia Region, from July 1 to August 30, 2024. Gurage zone is bordered on the southeast by Hadiya zone, on the west by Yem special Woredas, on the northeast by Oromia Region, and on the southeast by Silte’s Zone. According to the 2018/2019 annual report of the Gurage Zone Health Office, there are 7 hospitals and 72 health centers serving the total population of the zone. Among these hospitals, five are primary hospitals, one general hospital, and one comprehensive specialized hospital. All hospitals deliver comprehensive obstetrical and gynecological care. 30 The study was conducted from July to August in all randomly selected public hospitals found in the Gurage zone, Central Ethiopia, 2024.
Population
Source population
All postpartum women who visited Gurage zone public hospitals for postnatal care services.
Study population
All postpartum women who visited Gurage zone public hospitals for postnatal care services during the study period.
Inclusion and exclusion criteria
All postpartum women who visited Gurage zone public hospitals for postnatal care services in the maternity care unit and were willing to participate in the study were included.
All postpartum women who were seriously ill and unable to respond during the data collection period were excluded from the study.
Sample size determination and sampling techniques
The sample size was determined using a single population proportion formula by considering a population proportion of 50% with a 95% confidence interval (CI) and a 0.05 margin of error.

With the assumptions of 95% CI, 5% margin of error, and an estimated knowledge of puerperal sepsis and self-care practices for puerperal sepsis prevention among postpartum women at 50% (p = 0.5), the formula yields 384. The estimated p-value was selected to obtain the ideal sample size and gave 422 with a 10% nonresponse rate.
There are seven hospitals in the Gurage zone. Using simple random sampling procedures, five public hospitals were selected. The estimated total number of postnatal women who visited each hospital for postnatal care services over the 2-month period was 925. Based on their case flow, the sample was proportionally allocated to each hospital.
A systematic random sampling technique was used to select study participants. The sampling interval (K) was calculated by K = N/n, where N = the total average number of postpartum women, and n = the actual sample size, which yields two. Then, every second mother was interviewed with a similar K value of two. The first study participant was selected by using a random sampling procedure (the lottery method) between the first two women who visited the maternity care unit for postnatal care services on the first day of data collection. Then, every second mother was enrolled in the study.
Study variables
Independent variables: Sociodemographic characteristics
Age, ethnicity, residence, religion, marital status, educational level, occupation, and family wealth index. Obstetrics-related Factors: Parity, number of antenatal care (ANC) contacts, place of ANC contact, gestational age at first ANC contact, and place of birth.
Components of counseling received after birth
Postpartum danger signs, nutrition, exclusive breastfeeding, immunization schedule, hygiene, exercise, and family planning. Counseling received on symptoms of puerperal sepsis: Fever, foul-smelling vaginal discharge, and abdominal tenderness.
Operational definition
Puerperal sepsis is a genital tract infection that can occur anytime from the onset of membrane rupture or labor up to the 42nd day postpartum, characterized by pelvic pain, fever, abnormal vaginal discharge, foul odor, or delayed uterine involution.1,7
Knowledge of puerperal sepsis score
Postpartum mothers who scored an average score on correct knowledge questions were considered to have good knowledge of puerperal sepsis. Those who scored lower than the mean were considered to have poor knowledge regarding puerperal sepsis.22,23,26
Self-care practices of puerperal sepsis prevention
Postpartum mothers who scored a mean or above on the self-care practice 10 questions (yes–no) related to puerperal sepsis were considered to have a good self-care practice. However, those who scored less than the mean score were considered to have poor self-care practices for puerperal sepsis prevention.23,26
Family wealth status
Households were given scores based on the assets they own, like a television, radio, and others, in addition to housing characteristics such as a source of drinking water, toilet facilities, and flooring materials. Each item was coded 0 for “No” and 1 for “Yes,” and then the Principal Component Analysis (PCA) was computed. The individual scores were added together, and the distribution among study participants was divided into 5 quintiles, each comprising 20% of the total participants. 31 Scores were then ranked into three quintiles so that each household received its quintile category. Accordingly, poor clients are in the first and second quintiles, medium clients are in the third quintile, and rich clients are in the fourth and fifth quintiles.32,33
Data collection tool and procedures
The data collection tool was adapted from similar research on the outcome of interest and used for collecting data.22,23,26 The questionnaire was prepared in English. Then, it was translated into the Amharic version, and then to the Guragigna language. After, it was translated back to the English version to check its consistency. The tool included postpartum mothers’ sociodemographic information, obstetrics-related factors, knowledge of puerperal sepsis, and reported self-care practices for puerperal sepsis prevention questions.
The overall knowledge score for each participant was calculated by summing the results from 12 questions, with a possible range of 0–12. The question items needed categorical responses (yes or no), with 1 point awarded for each correct answer and 0 for each incorrect answer. The self-care practices were assessed based on practice-related questions, and the overall mean was computed and dichotomized. Postpartum mothers who scored above the mean value were considered to have good self-care practices, which was coded as “1,” and those mothers who scored less than the mean value were considered to have poor self-care practices, which was coded as “0.”
This research utilized a standardized questionnaire previously used by different scholars, which underwent a pretest to ensure clarity, appropriateness, and reliability. The tool’s content validity was checked by a panel of experts for relevance and essentiality, and its content reliability was assessed using Cronbach’s alpha, resulting in a 0.86 Cronbach’s alpha value for postpartum women’s knowledge-related questionnaires and a 0.93 Cronbach’s alpha value for self-care practice-related questionnaires.
Data were collected through face-to-face interviews at 6 weeks of the postnatal period at the maternity care unit. For data collection, two BSc midwives, two Nurses as data collectors, and one MSc nurse supervisor were recruited, who were able to speak Amharic and Guragigna local languages.
Data quality management
The tool was pretested on 21 postpartum mothers at Wolkite Health Center prior to the actual data collection to ensure consistency, clarity, and completeness of the tool. Data collectors and the supervisor received 2 days of training on the study’s objectives, questionnaire clarification, sampling strategy, and data collection process and supervision.
The principal investigator and supervisor guided, facilitated, and checked data completeness, ensuring the overall activities were effectively managed throughout the data collection process. Data were coded, entered, and rechecked during data entry into the computer software before analysis. Simple frequencies and a box plot were used to look for missing values and outliers, respectively.
Statistical analysis
After the data were thoroughly coded and carefully entered into the Epidata version 4.6 computer program, it was exported to SPSS version 26 for analysis. PCA was computed to see the wealth status of households. From a total of 15 items included in the analysis, 3 factors with ten items were created, which together explained 73.6% of the total variance. A descriptive statistical analysis was conducted to summarize and describe the characteristics of the study participants, and the information was presented using text, frequency tables, and figures.
The dependent variables were dichotomized as good or poor based on the analyzed mean values. A logistic regression model was fitted to assess the relationship between the outcome and independent variables. All predictor variables with a p-value of 0.25 or less in binary logistic regression were considered candidates for multivariable logistic regression analysis. In this study, the adjusted odds ratio (AOR) with 95% CIs, and a p-value less than 0.05 was used to declare a statistically significant association between the outcome and predictor variables. Multivariable logistic regression analysis was performed to identify variables in the final model.
Model fitness was confirmed using the Hosmer and Lemeshow Goodness of Fit test, with p-values of 0.461 and 0.523 for knowledge and reported self-care practices of puerperal sepsis prevention, respectively. The omnibus tests of model coefficients were less than 0.0001 for both outcomes, confirming the overall significance of models. Multicollinearity among independent variables was assessed using Variance inflation factor (VIF) and tolerance tests. The maximum VIF values were 2.67 and 2.53, and the minimum tolerance values were 35.4% and 36.2%, for knowledge and self-care practice, respectively, indicating no multicollinearity issues. Finally, the results were presented in tables, graphs, and figures.
Ethical approval and consent to participants
Ethical clearance was obtained from the Wolkite University, College of Medicine and Health Sciences Ethics Committee (Ref no. WKU-CMHS REC 025/2024). A formal letter of permission was obtained from Wolkite University and submitted to the Zonal Health Office and the hospitals to authorize the conduct of the research. The study was conducted in accordance with the ethical standards outlined in the Declaration of Helsinki. An ethical letter was written to the Gurage zone public hospitals to obtain permission for data collection. The purpose of the study and participants’ right to refuse were explained to the study participants, and informed written consent was obtained. Moreover, consent from participants with no formal education was obtained after the information sheet was read aloud in the local language and documented by thumb impression with a witness. Additionally, written informed consent was obtained from the legally authorized representatives of all minor (under 18 years) participants before enrollment. Coding was implemented to remove respondents’ names and other personal identifiers throughout the study to ensure participant confidentiality.
Results
Among a total sample of 422 study participants, 417 were interviewed, yielding a response rate of 98.8%, and the results are presented below under subheadings.
Sociodemographic characteristics of the study participants
Nearly two-fifths of respondents were in the age group of 25–29 years, with a mean age of 27 years (27 ± 2.1 SD). More than three-fourths of women were of Gurage ethnicity 320 (76.7%), over half lived in urban areas 216 (51.8%), nearly half were orthodox in religion 194 (46.5%), about one-third had completed primary school concerning their educational level 124 (29.7%), and nearly two-fifths of respondents had a high family wealth index of 161 (38.6%) (Table 1).
Sociodemographic characteristics of study participants among postpartum women in Gurage zone public hospitals, Central Ethiopia, 2024.

Welayita, Kembata, Oromo.
Adventist, Catholic.
Obstetrics characteristics of study participants
More than half of the study participants were primiparous in parity 236 (56.6%), three-fifths had ANC contact of eight or more 250 (60%), with a mean ANC contacts of 6.4 (6.4 ± 2.0 SD), and more than three-fourths started their ANC follow-up during the first trimester 320 (76.7%). Most of the study participants had received counseling after delivery (Table 2).
Obstetrics characteristics of study participants among postpartum women in Gurage zone public hospitals, Central Ethiopia, 2024.
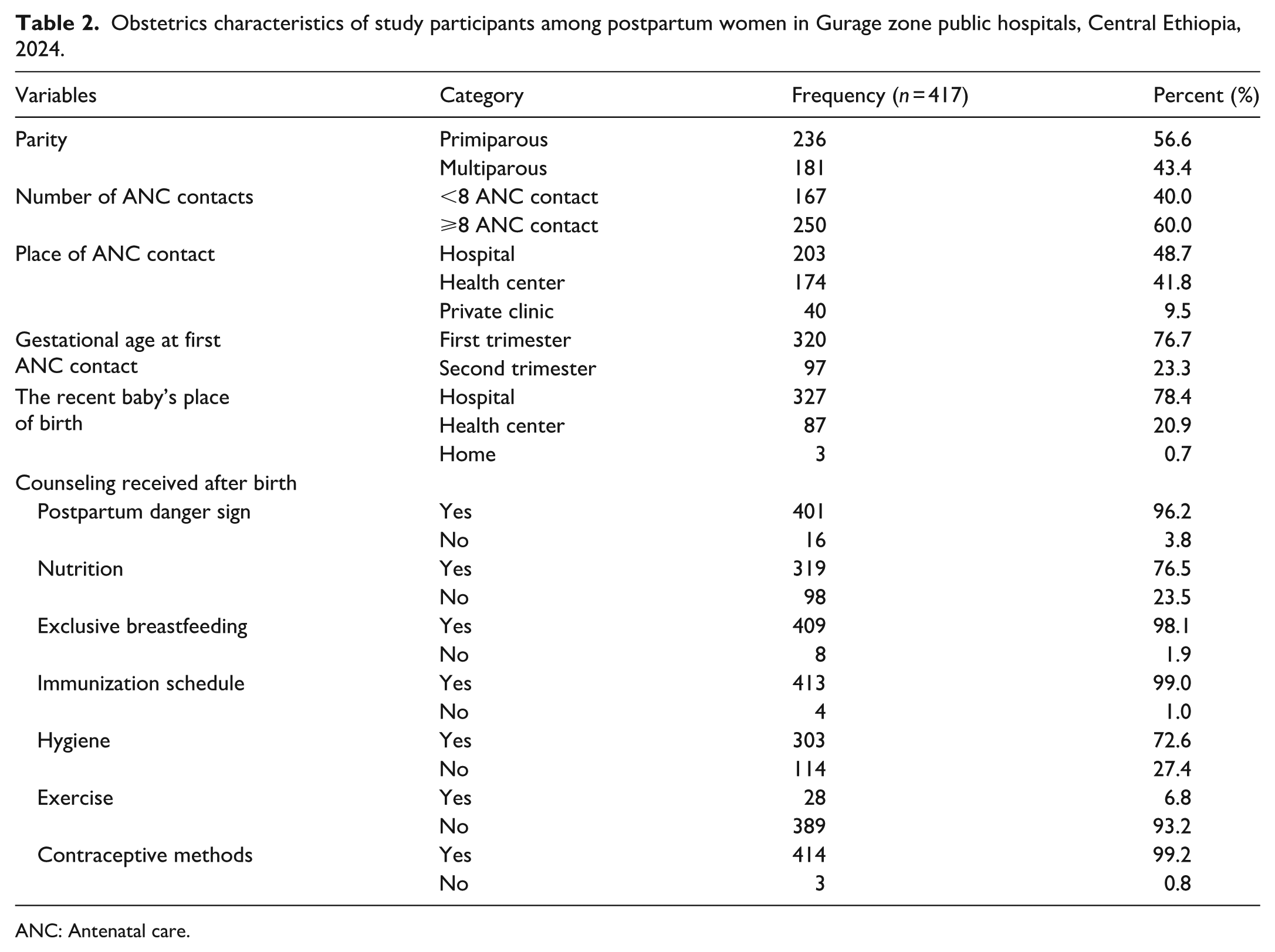
ANC: Antenatal care.
Women who received counseling on symptoms of puerperal sepsis
Nearly half of the participants were counseled on fever (49.6%), more than half on foul-smelling vaginal discharge (51.1%), and only one-fifth on abdominal tenderness; all of these are symptoms of puerperal sepsis that require treatment at a health facility (Figure 1).
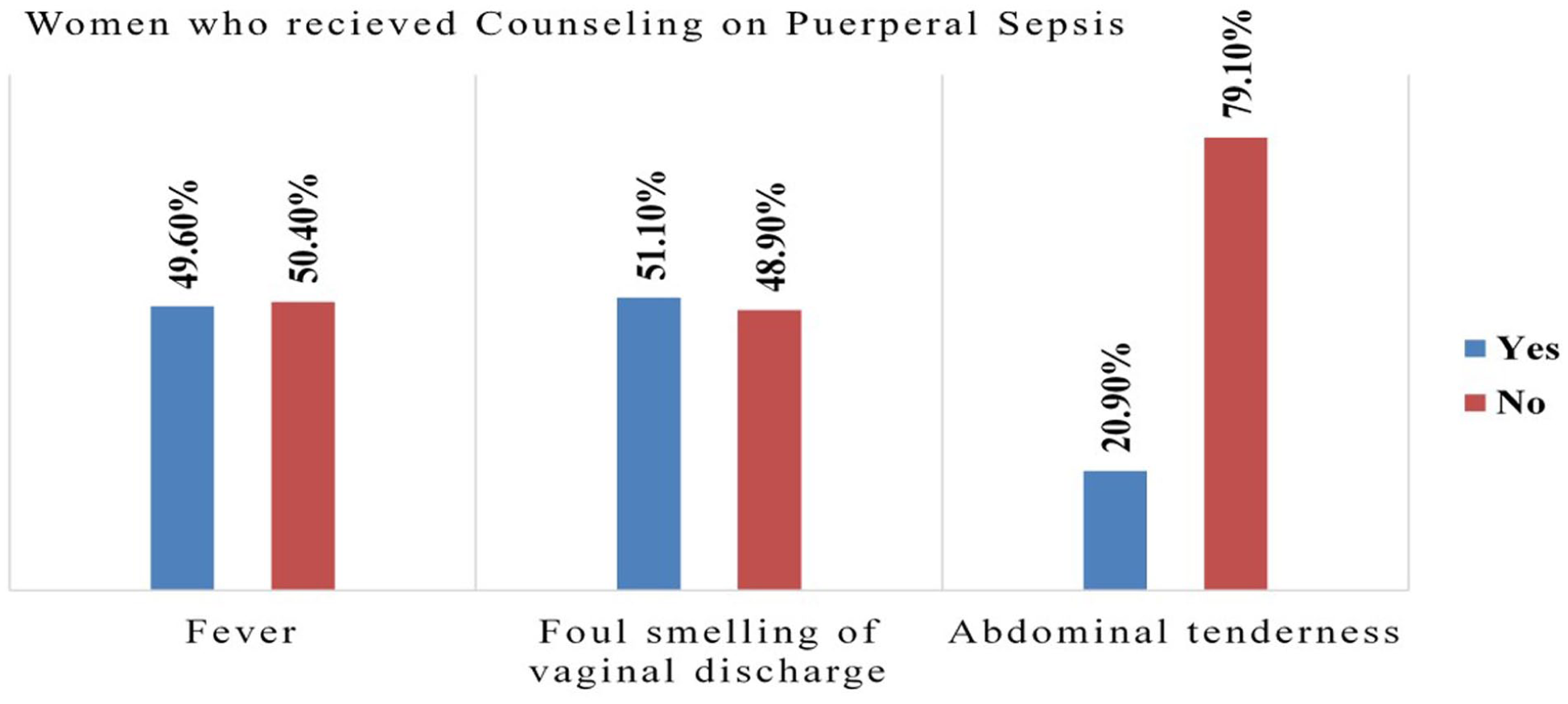
Women who received counseling on symptoms of puerperal sepsis from health care providers in Gurage zone public hospitals, Central Ethiopia, 2024.
Women’s knowledge regarding puerperal sepsis
The overall women’s knowledge level toward puerperal sepsis was 40.8% (36%, 46%). Less than half of the study participants were knowledgeable about puerperal sepsis (Figure 2).
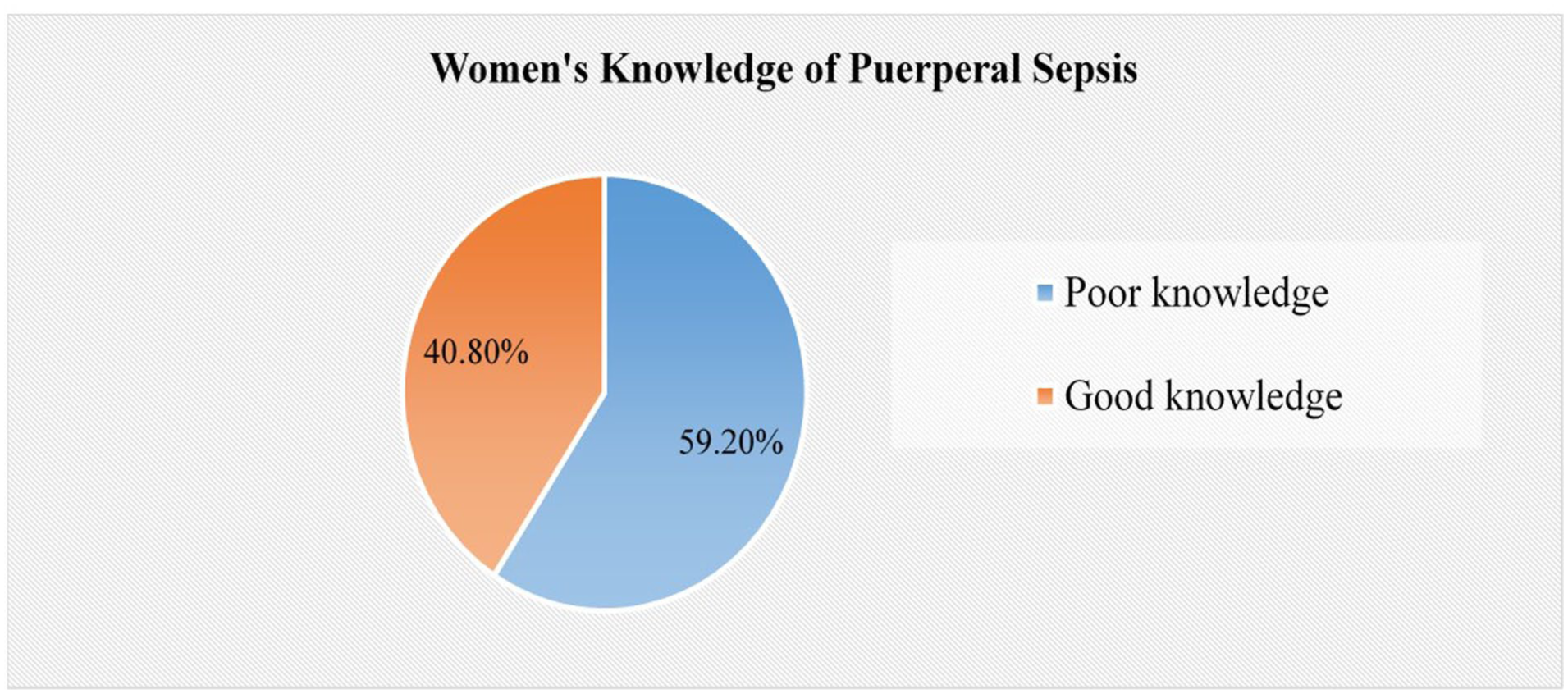
Women’s knowledge toward puerperal sepsis in Gurage zone public hospitals, Central Ethiopia, 2024.
Factors associated with women’s knowledge of puerperal sepsis
Binary logistic regression analysis was performed to identify candidate variables for multivariable logistic regression at a p-value of 0.25. Variables such as residence, family wealth index, educational level, occupation, parity, and ANC contact were identified as candidate variables for multivariable logistic analysis. All candidate variables were entered simultaneously into a multivariable logistic regression using the enter method to identify the final predictors of women’s knowledge of puerperal sepsis while controlling for potential confounders.
In multivariable analysis, three variables, educational level, occupation, and ANC contact, were found to be statistically significantly associated with women’s knowledge of puerperal sepsis after adjusting for confounders in the final model.
Women who attended secondary school and those with a diploma or higher education were 1.13 and 2.1 times (AOR = 1.13; 95% CI: 1.10, 2.85 and AOR = 2.1; 95% CI: 1.64, 5.43) more likely, respectively, to have good knowledge of puerperal sepsis compared to women with no formal education.
The odds of having a good knowledge of puerperal sepsis were twice (AOR = 2.01; 95% CI: 1.2, 3.4) as high in employed women compared to unemployed women. Women who had ⩾8 ANC contacts were 1.3 times (AOR = 1.3; 95% CI: 1.23, 2.97) more likely to have good knowledge of puerperal sepsis compared to their counterparts (Table 3).
Factors associated with women’s knowledge of puerperal sepsis in Gurage zone public hospitals, Central Ethiopia, 2024 (n = 417).

COR: Crude odds ratio; AOR: Adjusted odds ratio; ANC: antenatal care; CI: Confidence interval.
(p < 0.25) in bivariate, 1 = Reference group.
statically significant in multivariable analysis.
Women’s self-care practice of puerperal sepsis prevention
The overall level of self-care practices for puerperal sepsis prevention was 29.3% (25%, 34%). More than two-thirds (70.7%) of women lacked good self-care practices for the prevention of puerperal sepsis (Figure 3).

Women’s self-care practice toward prevention of puerperal sepsis in Gurage zone public hospitals, Central Ethiopia, 2024.
Factors associated with self-care practices for puerperal sepsis prevention
Binary logistic regression analysis was performed to identify candidate variables for multivariable logistic regression at a p-value of 0.25, and variables such as educational level, occupation, family wealth index, parity, ANC contact, and women’s knowledge of puerperal sepsis was identified as a candidate variable for multivariable logistic analysis. All candidate variables were entered together into a multivariable logistic regression using the enter method to identify the final predictors of women’s self-care practices for puerperal sepsis prevention while controlling for potential confounders.
In multivariable analysis, three variables, multiparous, ⩾8 ANC contacts, and women’s knowledge of puerperal sepsis, were found to be statistically significantly associated with women’s self-care practices for puerperal sepsis prevention after adjusting for confounders in the final model.
Multiparous women were 1.2 times (AOR = 1.2; 95% CI: 1.04, 3.14) more likely to have good self-care practices for puerperal sepsis prevention compared to primiparous women. Women who attended ⩾8 ANC contacts were 1.27 times (AOR = 1.27; 95% CI: 1.15, 2.81) more likely to have good self-care practices for puerperal sepsis prevention compared to their counterparts.
Postpartum women who have good knowledge 4.3 times (AOR = 4.3; 95% CI: 2.14, 9.31) are more likely to have good self-care practices for puerperal sepsis prevention compared to those who have poor knowledge of puerperal sepsis (Table 4).
Factors associated with women’s self-care practices for puerperal sepsis prevention in Gurage zone public hospitals, Central Ethiopia, 2024 (n = 417).

COR: Crude odds ratio; AOR: Adjusted odds ratio; ANC: antenatal care; CI: Confidence interval.
(p < 0.25) in bivariate analysis, 1 = Reference group.
statistically significant in multivariate analysis.
Discussion
Self-care practices for puerperal sepsis prevention are critical for postnatal women’s health. Poor self-care practices are a root cause of major postpartum complications, which contribute to maternal morbidity and mortality. This institution-based cross-sectional study identifies factors associated with women’s knowledge of puerperal sepsis and their self-care practices for its prevention. In this study, women’s educational status, ANC contact, and occupation were associated with knowledge of puerperal sepsis. Furthermore, parity, ANC contact, and women’s knowledge of puerperal sepsis were associated with self-care practices for its prevention.
In this study, the overall proportion of women with good knowledge of puerperal sepsis and self-care practices for puerperal sepsis prevention was 40.8% (95% CI: 36, 46) and 29.3% (95% CI: 25, 34), respectively. This means that 59.2% and 70.7% lacked knowledge of puerperal sepsis and self-care practices, respectively.
Regarding self-care practices for puerperal sepsis prevention, this finding is higher than studies conducted in Tanzania (11.4%) and Egypt (25.3%).20,23 The possible reason for this might be variation in sample size, study period, sampling techniques, and educational attainment of the study subjects, as both studies had small sample sizes. Another explanation might be differences in counseling about the symptoms of puerperal sepsis and its prevention. On the other hand, this result is lower than the study conducted in Arba Minch, Ethiopia (45.6%). 26 The discrepancy might be due to the study setting, educational status of the study subjects, and level of awareness regarding puerperal sepsis prevention. The study in Arba Minch reported higher educational status and awareness among participants compared to this study. Moreover, the study in Arba Minch included only urban postpartum women, whereas this study included both urban and rural (48.2%) postpartum women.
Regarding the knowledge of puerperal sepsis, in this study, 59.2% lacked good knowledge of puerperal sepsis. This finding is higher than the study conducted in Minia University Hospitals, Egypt (12.6%). 20 The discrepancy might be due to variation in sample size, study setting, study year interval, sociodemographic background of the participants, and counseling about symptoms of puerperal sepsis and its prevention.
Women who attended secondary school and those with a diploma or higher education were 1.13 and 2.1 times more likely, respectively, to have good knowledge of puerperal sepsis compared to women with no formal education. These findings are consistent with studies conducted in Bangladesh, Tanzania, Arba Minch Town, and Minia University Hospital, Egypt.20,22,23,26 The evidence showed that women’s knowledge increased as the level of their education increased.22,23 Therefore, higher educational attainment may help postpartum mothers become more aware of puerperal sepsis and its prevention during the puerperal period.
Study participants who were employed had 1.3 times higher odds of having good knowledge of puerperal sepsis compared to the unemployed. The possible explanation is that employed women who are have greater access to information about puerperal sepsis and to quality healthcare compared to unemployed women. 34 Women who had ⩾8 ANC contacts had 1.3 times higher odds of good knowledge of puerperal sepsis compared to their counterparts. This may be because as ANC contacts increase, the chance to receive information from healthcare personnel also increases, thereby enhancing knowledge of puerperal sepsis. This finding is supported by studies conducted in Hadiya Zone and Uganda.19,35
Regarding the self-care practice for puerperal sepsis prevention, 70.7% lacked self-care practices of puerperal sepsis prevention. Multiparous women were 1.2 times more likely to have good self-care practices for puerperal sepsis prevention compared to primiparous women. This is inconsistent with the study conducted in Arba Minch Town. 26 The possible explanation for this discrepancy is that women who have more labor and delivery experience can self-care regarding their well-being and their children. The evidence showed that women’s experience and confidence often enhance better self-care practices, both during pregnancy and after childbirth. 36 Furthermore, primiparous women feel less prepared for the realities of postpartum life and routine self-care due to fear, anxiety, depression, and less self-efficacy after birth compared to multiparous women,37,38 which might lead to poor self-care practices for puerperal sepsis prevention.
The current study found that postnatal women who attended ⩾8 ANC contacts were 1.27 times more likely to have good self-care practices for puerperal sepsis prevention compared to their counterparts. A possible explanation is that as ANC contacts increase, the chance to receive information regarding puerperal sepsis and self-care practices from healthcare personnel also increases, enhancing their self-care practices of puerperal sepsis prevention. The evidence showed that as ANC contacts increase, the level of self-care practice also increases.23,35 In addition, women who attend ANC during pregnancy and postnatal visits could be more aware of postpartum danger signs, which enhances postnatal self-care. 33
This study revealed that postpartum women who had good knowledge were 4.3 times more likely to have good self-care practices of puerperal sepsis prevention compared to those who had poor knowledge of puerperal sepsis. This is supported by studies conducted in Arba Minch, Tanzania, and Egypt.20,23,26 The possible explanation for this is that empowering women with knowledge can enhance informed decision-making and protect their health and well-being during the postpartum period, potentially preventing puerperal sepsis. 39 Furthermore, as women’s knowledge level increases, their ability for self-care also increases. 40 Therefore, these findings show important gaps in knowledge and self-care practices for preventing puerperal sepsis among postpartum women in the Gurage zone, Central Ethiopia. The results suggest that improving health education during ANC and postnatal visits is essential. Enhancing the quality of ANC contact, women’s educational status, and the provision of counseling and awareness-creating postpartum danger signs could significantly improve self-care practices, which have the potential to reduce postpartum complications, maternal morbidity, and mortality in the study area.
Strengths and limitations of the study
Strength of the study
Measurements of the women’s knowledge of puerperal sepsis and self-care practice for puerperal sepsis prevention included both multiparous and primiparous women.
To the investigator’s knowledge, no study has been conducted in the study setting. In this study, potential biases were minimized by using clear objectives, research questions, pretested questionnaires, training provided for data collectors and supervisors, a random sampling method, an ideal sample size, and statistical adjustments (multivariable regression) to account for confounding variables. Finally, ethical guidelines were implemented to ensure unbiased participants.
Limitations of the study
In this study, self-reported data on postpartum women’s self-care may have introduced recall bias, leading to possible over- or under-reporting. Additionally, as this was a cross-sectional study, it does not establish cause-and-effect relationships. Even so, the hospitals were selected using simple random sampling. However, since the study did not include all hospitals in the area, this may affect the generalizability of the findings.
Implications for practice
Even though puerperal sepsis can cause postpartum life-threatening complications, good self-care can reduce and prevent further complications. The findings of this research have many implications for enhancing the knowledge of puerperal sepsis and self-care practices. The study showed that 59.2% and 70.7% of women lacked knowledge of puerperal sepsis and self-care practices, respectively. Furthermore, the study revealed that the factors associated with self-care practices for puerperal sepsis prevention among postpartum women provide important information for Woreda and Zonal health offices, hospitals, and healthcare providers to improve women’s self-care practices. Health care personnel play a significant role in enhancing awareness among women regarding self-care.
This highlights the need for an ongoing plan to support postpartum women’s self-care practices and for effective health provider education at both institutional and community levels, enabling reproductive-age women to counsel postpartum women about complications and timely self-care. Additionally, researchers can use this study as a basis to explore other factors associated with self-care practices for puerperal sepsis prevention at different levels and to develop interventional projects targeting modifiable factors that affect postpartum women’s knowledge and self-care practices.
Conclusion and recommendations
Conclusion
This study showed that 59.2% and 70.7% of postpartum women lacked good knowledge and self-care practices for puerperal sepsis prevention. Women’s primary role in puerperal sepsis self-care is to improve their well-being and, indirectly, that of their fetus and families. The educational status, women’s occupation, and antenatal contact were significantly associated with the women’s knowledge of puerperal sepsis and parity, and antenatal contacts and knowledge of puerperal sepsis were significantly associated with self-care practices for puerperal sepsis prevention. As a result, the study concludes that by intervening in the modifiable factors, postpartum women’s awareness regarding self-care practices can be increased.
Recommendations
The following recommendations were given based on the findings to the concerned bodies:
To Gurage zone public hospitals and healthcare providers
It is encouraged to provide targeted health education on puerperal sepsis and its prevention during ANC contact and postnatal checkups using simple, culturally appropriate materials to improve women’s knowledge and self-care practices.
At the community level
It is recommended to design community-based awareness campaigns targeting women with lower educational status and those in less formal occupations. Additionally, health extension workers and community health volunteers should be encouraged to disseminate information at the household and community levels to improve postpartum women’s knowledge of puerperal sepsis and enhance their self-care practices for puerperal sepsis prevention.
To policymakers and the healthcare system
To strengthen the integration of puerperal sepsis prevention into maternal and child health programs at all levels of the healthcare system through policies that ensure universal access to maternal health education and improve ANC coverage and postnatal visits.
For the researcher
A longitudinal study and a qualitative study is needed to identify important factors and gain a better understanding of women’s self-care practices for puerperal sepsis. Additionally, the current study recommends further research to investigate unsafe postpartum practices related to puerperal sepsis during postpartum and their effect on maternal health.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251387974 – Supplemental material for Knowledge of puerperal sepsis, self-care practices of puerperal sepsis prevention and associated factors among postpartum women in the Gurage zone, Central Ethiopia: Multicenter study
Supplemental material, sj-docx-1-smo-10.1177_20503121251387974 for Knowledge of puerperal sepsis, self-care practices of puerperal sepsis prevention and associated factors among postpartum women in the Gurage zone, Central Ethiopia: Multicenter study by Mangistu Abera, Mesfin Difer Tetema, Fentahun Tamene Zeleke, Keyredin Nuriye Metebo, Aberash Beyene Derribow, Megertu Obsa Gelmesa, Ayana Benti Terefe, Tolesa Gemeda Gudeta, Obsa Dabala, Meskerem Alemayehu Weldeyohans, Melese Gabure Shukulo and Mebratu Demissie Senbeta in SAGE Open Medicine
Supplemental Material
sj-pdf-2-smo-10.1177_20503121251387974 – Supplemental material for Knowledge of puerperal sepsis, self-care practices of puerperal sepsis prevention and associated factors among postpartum women in the Gurage zone, Central Ethiopia: Multicenter study
Supplemental material, sj-pdf-2-smo-10.1177_20503121251387974 for Knowledge of puerperal sepsis, self-care practices of puerperal sepsis prevention and associated factors among postpartum women in the Gurage zone, Central Ethiopia: Multicenter study by Mangistu Abera, Mesfin Difer Tetema, Fentahun Tamene Zeleke, Keyredin Nuriye Metebo, Aberash Beyene Derribow, Megertu Obsa Gelmesa, Ayana Benti Terefe, Tolesa Gemeda Gudeta, Obsa Dabala, Meskerem Alemayehu Weldeyohans, Melese Gabure Shukulo and Mebratu Demissie Senbeta in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank Wolkite University for giving us the opportunity to conduct the research and for granting ethical approval. Authors also extend our gratitude to study participants, data collectors, and the supervisor for their unreserved efforts and willingness to participate in this research study.
ORCID iDs
Author contributions
MA, MDS, and ABD wrote the proposal, participated in data collection supervision, analyzed the data, and drafted the article. MA, KN, ABT, TGG, FTZ, and AS approved the proposal with some revisions, participated in data analysis, and revised subsequent article drafts. MA, ABD, and MDS commented on the final article. All authors read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data that support the findings are available from the corresponding author upon a reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.