
Abstract
Introduction:
Puerperal sepsis is a leading cause of maternal morbidity and mortality in low-income countries, which can affect sustainable development goals. Even though it is a preventable problem through maternal self-care practices, maternal-reported self-care practices regarding puerperal sepsis were under-researched in Ethiopia. Therefore, this study aimed to assess the maternal reported self-care practice and associated factors among postnatal mothers for the prevention of puerperal sepsis.
Objective:
The study aimed to assess the reported self-care practice of postnatal mothers in Arba Minch town toward the prevention of puerperal sepsis and its associated factors.
Methods:
A community-based cross-sectional study was employed from 1st to 30th May 2022. Study participants were selected using a simple random sampling technique. Data was collected by the Open Data Kit tool and exported to SPSS version 26 for further analysis. Both crude and adjusted odds ratios with a 95% CI were calculated, and a p-value of less than 0.05 was used to declare statistically significant factors.
Results:
Of a total of 423 postpartum mothers, 417 participated, making a response rate of 98.5%. The study revealed that 45.6% (95% CI: 41.2%, 50.1%) of postnatal mothers had good reported self-care practices toward the prevention of puerperal sepsis. Tertiary educational level (AOR: 2.56; 95% CI: 1.43, 4.59), multiparity (AOR: 0.44; 95% CI: 0.26, 0.74), and having a good awareness of puerperal sepsis prevention (AOR: 2.17; 95% CI: 1.40, 3.37) were significantly associated at a p-value less than 0.05.
Conclusion:
This study revealed that less than half of postnatal mothers reported good self-care practices. Healthcare providers and all stakeholders should focus on strategies to improve self-care practice during antenatal and postnatal care and at a community level, with a special focus on postnatal mothers with no formal education and multiparous mothers.
Introduction
The World Health Organization (WHO) defined puerperal sepsis as an infection of the genital tract that occurs from rupture of membranes or labor to 42 days postpartum with at least two of the following conditions: pelvic pain, fever (oral temperature equal to or greater than 38.5°C), purulent, cloudy, or offensive vaginal discharge, or delayed uterine involution. 1 During the postnatal period, maternal immunity will be impacted as a result of hormonal and physiological changes related to pregnancy and childbirth. 2 This immune status is of paramount importance to maintain maternal health and enhance the recovery of mothers from childbirth trauma. 3
Beyond the care provided by healthcare providers, maternal self-care practices play a crucial role in influencing maternal health during the postnatal period. Maternal self-care is the mother’s ability to take care of herself physically, which includes proper nutrition, taking time to herself when necessary, hygiene, and physical appearance.4,5
The first year after childbirth is a period of profound transition for mothers. She experiences several physiological changes during the postnatal period. The prevention, identification, and management of postpartum complications are critical components of maternal perinatal well-being. 6
Currently, puerperal sepsis is a major source of worry 7 and if not recognized and treated early, it can cause long-term health problems such as pelvic inflammatory disease (PID) and infertility, in addition to maternal morbidity and mortality.8–10 This health problem has a multi-dimensional impact, increasing early neonatal mortality as the mother is unable to care for the infant as a result of puerperal sepsis. 11 Puerperal sepsis not only endangers the mother’s health but also imposes financial strain on the family due to the associated treatment costs, including hospital stays and medications. 12
Globally, out of a total of 6 million cases, 77,000 mothers die each year, 13 and the majority of these deaths occurred in low-income countries.14,15 In low-income countries, puerperal sepsis is the leading cause of maternal death, accounting for 15% of all maternal deaths. In Ethiopia, 13% of maternal mortality is caused by puerperal sepsis.8,16,17 Despite the fact that puerperal sepsis is a challenge to maternal health, a pocket of studies conducted in Africa revealed the lowest magnitude of good reported self-care practice during the postpartum period, which ranges from 11.4% to 40.8%.18,19
Scholars identified educational level, number of antenatal cares, and knowledge level as significantly associated factors with reported self-care practices regarding puerperal sepsis.18,20,21 In addition, lack of awareness, ignorance, customs, and social behaviors were significantly associated factors with reported self-care practices. 22
Individual awareness, effective prevention, early detection, and appropriate therapy for sepsis can reduce the burden of infections as a cause of morbidity and mortality.6,23 Furthermore, education and awareness of puerperal sepsis prevention are critical in preventing puerperal sepsis in women in the postnatal period. 24
Even though puerperal sepsis ranks among the top causes of maternal death, 13 it has gotten less attention in Ethiopia. This indicates postnatal mothers neglect to take self-care measures to prevent puerperal sepsis. The postnatal mother’s knowledge and reported self-care practices should be known to overcome problems related to puerperal sepsis and intervene based on the gap.
Moreover, there is limited data regarding maternal self-care toward the prevention of puerperal sepsis in Ethiopia. Therefore, this study aimed to assess reported self-care practices toward prevention of puerperal sepsis and determine factors associated with self-care practice among postnatal mothers in Arba Minch town in 2022.
Methods and materials
Study design, area, and period
A community-based cross-sectional study was employed in Arba Minch town, southern Ethiopia, from 1–30 May 2022. Arba Minch town is located 505 km south of Addis Ababa, the capital city of Ethiopia. This town has a total population of 112,724 in 24,090 households. The total number of reproductive-age women in this town is 56,137, and the expected delivery is 4272. 25 In Arba Minch town, there are two governmental hospitals, two health centers, 11 health posts, 33 private clinics, and 13 drug stores. The town has 12 kebeles, the smallest administrative part of the town.
Population of the study
Source population
All postnatal mothers in Arba Minch town.
Study population
All postnatal mothers in Arba Minch town who were in the first 6 weeks after childbirth during the data collection period were the study population.
Inclusion and exclusion criteria
All postpartum mothers in the first 6 weeks and who lived in the town at least for 6 months during the data collection period were included in the study. Critically ill mothers during data collection and those who are greater than 6 weeks postpartum were excluded from the study.
Sample size determination
The sample size was determined using a single population proportion formula with a 95% confidence level, 50% proportion of good self-care practice with a 5% margin of error. By substituting in the formula;
Sampling procedures
Initially, we obtained the total number of deliveries in each Kebele, which amounted to 807, within the first 6 weeks after childbirth, from the logbooks of health extension workers. Subsequently, we conducted proportional allocations for each kebele based on this data to determine the final sample size. Using the family folder codes of each mother’s house, we created a table of random numbers. Then, employing a computer-generated simple random sampling method, we selected mothers proportionally from this table of random numbers. Two weeks before data collection, selected houses were coded with the assistance of each Kebele’s health extension worker to facilitate the process (Figure 1).

Schematic presentation of sampling procedure to assess reported self-care practice and associated factors among postnatal women in Arba Minch town, Southwest Ethiopia, 2022.
Operational definitions
Reported self-care practice: Reported self-care practice was assessed based on eight practice-related yes-or-no questions. The mean was calculated based on these eleven questions, and the overall mean was calculated and dichotomized as mothers who scored above the mean were considered to have good reported self-care practices that were coded as “1” and those who scored below the mean were coded as “0” and considered to have poor reported self-care practices.18,19
Awareness of puerperal sepsis: The maternal awareness of puerperal sepsis was assessed by 11 awareness-related “yes/no” questions. Then the overall mean was calculated and dichotomized as follows: the mother had good awareness if the score was above the mean, which was coded as “1,” and those mothers who scored below the mean were considered to have poor awareness, which was coded as “0.” 19
Wealth index: The wealth index is assessed by 38 items developed to assess the selected ownership of assets and properties owned by households. Then principal component analysis was done and divided into three equal parts: poor, which was coded as “1,” medium, which was coded as “2,” and rich, which was coded as “3,” depending on previous studies. 26
Data collection tool and procedures
Data were collected through face-to-face interviews using a structured questionnaire developed from related literature.18,19 The tool comprised socio-demographic characteristics, obstetric history, awareness of puerperal sepsis prevention, sources of information, reported self-care practices for postnatal mothers, prevention of puerperal sepsis, and household wealth index. The self-care practice assessment tool included 11 questions derived from literature, demonstrating good internal consistency (Cronbach’s alpha = 0.78) and content validity confirmed by experts. Six BSc midwifery students conducted data collection under the supervision of three public health officers, who ensured daily checks for data completeness.
Data quality control
The questions were initially written in the English language, then translated to the Amharic language and re-translated back to check their consistency. A pre-test was done on 10% of the sample size in Sodo town, Fana Kebele, 1 week before actual data collection. Training was given to data collectors and supervisors to make them familiar with data collection tools, including ODK data collection techniques, ethical issues, and the objectives of the study.
During data collection, the supervisors reviewed the completed questionnaires for critical information before uploading them from an Android mobile phone to the ODK Toolbox server. The device was used to capture all the data on-site, and it was uploaded every week to the ODK server. After data collection, each questionnaire was given a unique code by the principal investigator and exported to SPSS version 26. Frequencies were used to check for missing values and outliers.
Data analysis
After data was collected through ODK, the data was downloaded as an excel file and exported to SPSS version 26. Then after it was checked for completeness, cleaned, and coded. Descriptive statistical analysis was used to describe the characteristics of the study participants. Finally, it was presented by frequencies, summary measures, tables, and figures.
Bivariate analysis, COR with 95% CI, was used to see the association between the independent variable and the dependent variable by using binary logistic regression. Independent variables with a p-value of < 0.25 in bivariate analysis were entered into a multivariable logistic regression model to adjust for the effects of possible confounders on the outcome variable. 27
The model’s goodness of fit was tested by the Hosmer-Lemeshow goodness of fit test, and multi-collinearity was checked by the tolerance and variance inflation factors. An adjusted odds ratio with a 95% CI was calculated to identify factors significantly associated with the reported self-care practices in a multivariable logistic regression analysis. The level of statistical significance was declared at a p-value < 0.05.
Ethics approval and consent to participate
Ethical approval for this study was obtained from Arba Minch University, College of Medicine and Health Sciences Institutional Review Board (Reference Number: IRB/1273/2022).
Written informed consent was obtained from each study participant, and each study participant was also informed about the objectives of the study and the confidentiality of the information she was giving. In addition, written informed consent was also obtained from those who were less than 18 years old because they could decide about themselves after they were married. 28 All procedures adhered to the principles outlined in the Helsinki Declaration and participants were assured of the voluntary nature of their participation.
Results
Socio-demographic and economic characteristics of the study participants
A total of 417 postnatal mothers participated in the study, yielding a response rate of 98.5%. From this, 193 (46.3%) were in the age group of 25–29 years old, with a mean age of 28.6 ± 5.1 years. This study revealed that 178 (42.7%) of the study participants were orthodox religion followers, and 385 (92.5%) were married (Table 1).
Frequency distribution of postpartum women by their socioeconomic and demographic characteristics in Arba Minch town, 2022 (N = 417).
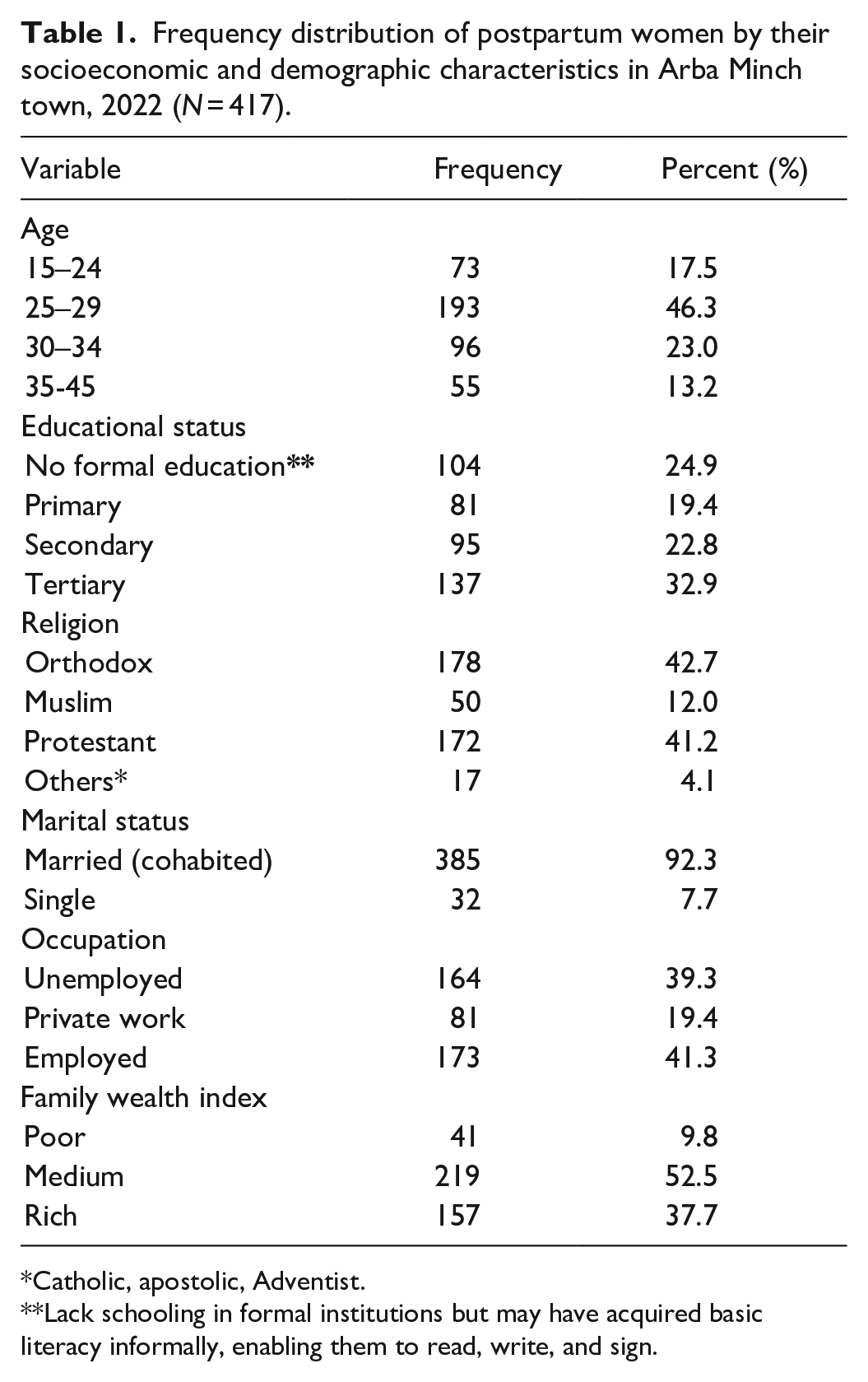
Catholic, apostolic, Adventist.
Lack schooling in formal institutions but may have acquired basic literacy informally, enabling them to read, write, and sign.
Reproductive characteristics of participants
A total of 399 (95.7%) of postnatal mothers had antenatal care (ANC) follow-up at least once. Among those who had ANC follow-up, only 132 (33.1%) respondents had counseled on nutrition, offensive vaginal discharge, leakage of liquor, and postpartum fever all together. The study revealed that 285 (63.1%) gave birth at public health institutions and 10 (2.4%) at home (Table 2).
Reproductive characteristics of study participants in Arba Minch town, Southern Ethiopia, 2022 (N = 417).

PS: puerperal sepsis; ANC: antenatal care.
Postnatal mother’s awareness on prevention of puerperal sepsis
Regarding the awareness of the participants, 56.4% (95% CI: 51.8, 60.9%) had good awareness, whereas the 43.6% of the participants had poor awareness toward the prevention of puerperal sepsis. Two-thirds of study participants, 276 (66.2%), had heard about puerperal sepsis, and 200 (72.5%) heard it from health professionals. One-quarter (24.6%) of participants defined puerperal sepsis correctly. Two hundred forty-four (88%) had identified the importance of ANC follow-up in the prevention of puerperal sepsis (Table 3).
Postnatal mother’s awareness on prevention of puerperal sepsis in Arba Minch town southern Ethiopia, 2022 (N = 417).

ANC: antenatal care; PS: puerperal sepsis.
Reported self-care practice of postpartum mothers toward prevention of puerperal sepsis
This study revealed that 45.6% (95% CI: 41.6%, 50.1%) of participants reported having good reported self-care practices toward the prevention of puerperal sepsis, whereas the rest of the participants had poor reported self-care practices toward the prevention of puerperal sepsis (Figure 2). Among respondents, 191 (45.8%) washed their hands prior to sanitary pad changing, 258 (61.9%) after toileting, 324 (77.7%), and only 134 (32.1%) reported that they were practicing all (Table 4).

Representing reported self-care practice of postnatal mothers in Arba Minch town, southern Ethiopia, 2022.
Reported self-care practice of postnatal mothers toward prevention puerperal sepsis in Arba Minch town, Southern Ethiopia, 2022 (N = 417).

Factors associated with reported self-care practice of postnatal mothers toward prevention puerperal sepsis
A multivariable logistic regression model was fitted to identify predictors of the reported self-care practices of postnatal mothers toward the prevention of puerperal sepsis. In the binary logistic regression analysis, variables with p-values less than 0.25 were considered candidate variables for the multivariable logistic regression model. Thus, age of mothers, occupation, educational level, parity, and awareness of puerperal sepsis prevention were entered into a multivariable logistic regression model.
The study revealed that those mothers who achieved tertiary educational levels were 2.56 times more likely to have good self-care practices than those who had no formal education (AOR = 2.56; 95% CI: 1.43, 4.59).
Reproductive characteristics, such as ANC visits and ANC counselling, did not show a significant association with self-care practices at a p-value less than 0.25. However, among the reproductive characteristics examined, only the parity of study participants notably impacted self-care practices. Consequently, we selectively included variables in the model that demonstrated an association with outcome variables below the 0.25 threshold. Furthermore, multiparous mothers exhibited 56% lower odds of good self-care practices compared to primiparous mothers (AOR = 0.44; 95% CI: 0.26, 0.74).
Additionally, mothers who have good awareness are 2.17 times more likely to have good self-care practices than those who have poor awareness (AOR = 2.17; 95% CI: 1.40, 3.37) (Table 5).
Factors associated with reported self-care practice of postnatal mothers toward prevention puerperal sepsis in Arba Minch town, Southern Ethiopia, 2022 (N = 417).

COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Significant at p < 0.05.
Discussion
This study attempted to assess reported self-care practices toward the prevention of puerperal sepsis and associated factors among postnatal mothers in Arba Minch town. The finding showed that 45.6% of postpartum mothers had had good self-care practices toward the prevention of puerperal sepsis. This finding is in line with a study done in Bangladesh 43.3%. 29 The similarity may be due to the similarity in the assessment scale used to assess postpartum women’s self-care practices for preventing puerperal sepsis.
However, this finding is higher than that of the study done in northwestern Ethiopia 40.8%, 19 in Tanzania 11.4%, 18 in Nepal 8.34%, 30 and in Minia University, Egypt 25.3%. 31 This disparity may be due to differences in the socio-demographic traits of study participants, the duration of time among studies, and shifts in postnatal mothers’ awareness over time due to changes in accessibility and use of maternal health care.
In addition, maternal health literacy might have increased when compared with previous studies, as health literacy increases the self-care practices toward the prevention of puerperal sepsis. Similarly, the discrepancy might be due to difference in the study setting as previous study was an institution-based study that might include both rural and urban residents, as rural residents are less likely to have good self-care practices. In addition, our study has only included urban residents, which will increase the magnitude of good self-care practices as a result of better access to maternal health services and health information than rural residents. 19
Conversely, the finding in this study is lower than that of the study conducted in Saudi Arabia 51%, 32 and in Chinakakani, India 51%. 33 The possible reason for the low self-care practice findings in this study could be influenced by differences in the study population’s demographic characteristics, health conditions, and socio-economic status. Additionally, there might be differences in healthcare infrastructure and health education systems for postpartum mothers.
This study found that educational level, parity, and awareness of puerperal sepsis as the significantly associated factors with reported self-care practices. It was revealed that having a tertiary educational level was a significantly associated factor with good self-care practices when compared with those who have no formal education. This finding is supported by the studies done in Tanzania, 18 northern Ethiopia, 19 and Uganda. 34
This association can be attributed to several factors. Firstly, individuals with higher educational levels often have better access to health information, which empowers them to adopt positive self-care practices. Additionally, education contributes to improved health literacy, enabling individuals to make informed decisions about their well-being. Higher educational attainment may also be linked to a greater awareness of the importance of preventive health measures and a better understanding of the benefits of good self-care practices. In addition, educated women can acquire health information to become aware of their health benefits, risk factors, and prevention strategies. 35
Furthermore, primipara mothers are more likely to have good self-care practices than multiparous mothers, which is supported by a study done in India. 36 Several factors could be contributed to this phenomenon. Firstly, multiparous mothers often face increased demands on their time and attention due to caring for multiple children, which might limit their ability to prioritize their own health and well-being. Additionally, past childbirth experiences may influence self-care practices, with primiparous mothers potentially placing more emphasis on preventive measures and health behaviors. Furthermore, social and cultural factors may play a role, as multiparous mothers might perceive themselves as more experienced and therefore less inclined to prioritize self-care.
In our study, we found that self-care practices toward the prevention of puerperal sepsis were not affected by the number of ANC visits and counseling received during these visits. This unexpected finding may be attributed to several factors. Firstly, the content and quality of ANC counseling sessions may vary widely, with some sessions focusing more on general health education rather than specific guidance on postpartum self-care. Additionally, cultural or social factors could influence the uptake and implementation of recommended self-care practices, irrespective of the ANC services received. Furthermore, individual perceptions, beliefs, and access to resources may also play significant roles in shaping self-care behaviors independently of ANC attendance.
Having good awareness of the prevention of puerperal sepsis was a significantly associated factor with good self-care practices toward the prevention of puerperal sepsis. This is supported by a study done on the importance of awareness of puerperal sepsis prevention among postpartum mothers. 6 Mothers who have a higher level of awareness regarding the prevention of puerperal sepsis are likely to have good reported self-care practices due to the information they have regarding puerperal sepsis. This emphasizes the importance of targeted health education initiatives aimed at enhancing awareness among postnatal mothers regarding puerperal sepsis prevention.
Moreover our study underscores the significance of considering cultural influences on postpartum self-care practices, which have important clinical implications. Cultural norms and beliefs significantly impact a woman’s willingness and ability to adopt self-care behaviors, potentially affecting her health outcomes.37,38 By integrating cultural considerations into postpartum care strategies, healthcare providers can tailor interventions to better support women in adopting effective self-care practices while respecting their cultural beliefs and traditions. This patient-centered approach not only enhances the overall well-being of postpartum women but also contributes to the prevention of puerperal sepsis, ultimately improving clinical outcomes.
Conclusions and recommendations
This study revealed that less than half of postnatal mothers had good self-care practices toward the prevention of puerperal sepsis. As identified by the study, educational level, parity, and awareness regarding puerperal sepsis were significantly associated factors with reported self-care practices toward the prevention of puerperal sepsis.
Based on the findings of this study, it was recommended that health professionals who work in maternity and child health care work on identified factors. In addition, all stakeholders should be involved to raise awareness about how to practice prevention of puerperal sepsis during the ANC, delivery, and postnatal period. Furthermore, community health extension workers should visit every mother at their home to know their health status and prevent the problem. Finally, it was recommended that it be better supported by a strong study design by other scholars.
Limitations and strength
Due to the cross-sectional nature of the study, it does not identify a cause-and-effect relationship. It may be prone to recall bias and social desirability bias, leading to either over- or under-reporting depending on how they acted while reporting recent and past information. It is the first community-based study regarding the reported self-care practices among postpartum mothers in this study area.
Footnotes
Acknowledgements
The authors express their gratitude to Arba Minch University College of Medicine and Health Sciences Department of midwifery for providing a collaboration letter, to Arba Minch town Health administrative office, and Health extension workers for giving valuable information regarding the study area. In addition, the authors extend their sincere gratitude to the data collectors, supervisors, and study participants for being involved in the study.
Author contributions
All the authors have contributed equally from proposal development to final manuscript development. Sheleme Mengistu Teferi: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing. Bezabih Terefe: Conceptualization; Data curation; Formal analysis; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing. Gebremariam Temesgen: Conceptualization; Data curation; Formal analysis; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing. Kenbon Seyoum: Data curation; Formal analysis; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing. Neway Ejigu Debebe: Data curation; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing. Chala Kene: Data curation; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing. Girma Geta: Data curation; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing. Lema Fikadu Wedajo: Conceptualization, manuscript preparation and editing.
Availability of data and materials
The data used for this study is available upon reasonable request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Arba Minch University, College of Medicine and Health Sciences Institutional Review Board (Reference Number: IRB/1273/2022).
Informed consent
Written informed consent was obtained from each study participant, and each study participant was also informed about the objectives of the study and the confidentiality of the information that was being given. In addition, written informed consent was also obtained from those who were less than 18 years old because they could decide about themselves after they were married.
Consent for publication
It is not applicable.
Trial registration
Not applicable.