
Abstract
Objectives:
This retrospective cohort study investigated the impact of COVID-19 on altered sodium and potassium in older adults with delirium compared to a non-COVID pneumonia control group.
Methods:
Electronic Medical Records (EMRs) from a university hospital database were reviewed for electrolyte abnormalities and delirium. We identified 319 patients with COVID-19, of which 108 (33.8%) had an episode of delirium during COVID. In a second cohort of 306 older adults with non-COVID pneumonias, we identified 106 (34.6%) with delirium during pneumonia.
Results:
Electrolyte disturbances were more commonly present in non-COVID pneumonias versus in those with COVID (p < 0.001). Hypokalemia was more frequent in the non-COVID group (p < 0.006), while hypernatremia was more often identified in the COVID group (p < 0.0321). Delirium in COVID patients was more commonly associated with hypernatremia than with other electrolyte abnormalities.
Conclusions:
Because hypernatremia can be associated with seizures and cerebral hemorrhage, our findings highlight the need for careful monitoring and management of hypernatremia in hospitalized COVID patients, especially in light of its observed association with delirium.
Introduction
The Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) or COVID-19 pandemic led to significant changes in current public health practice, hospital management, and epidemiological theory. 1 Efforts to elucidate the pathophysiology of COVID-19 are ongoing, and much progress has been made.
It has been determined that the mechanism of SARS-CoV-2 infection involves binding of angiotensin I-converting enzyme 2 (ACE2) This enzyme has important implications for the proper functioning of the renin-angiotensin-aldosterone system (RAAS). 2 Specifically, ACE2 acts as a regulator to prevent ACE from generating angiotensin II, which can cause pulmonary damage and edema at excessive levels. 3 Inhibition of ACE2 by SARS-CoV-2 increases the activity of angiotensin II, leading to greater levels of aldosterone secretion and increased sodium reabsorption. 4
Based on current research, likely routes of SARS-CoV-2 interaction with ACE2 are through lung and small intestine tissue. 5 The reach of ACE2 expression extends far beyond these previously mentioned tissues; ACE2 can also be found within the epithelium of the vasculature, the heart, and the kidneys. 6 The widespread expression of ACE2 in multiple organ systems and subsequent disruption of RAAS in COVID-19 suggests that infection can lead to significant and wide-ranging electrolyte disturbances.
It has been shown that there is an association between sodium imbalances and worsened clinical outcomes in COVID patients. 7 For example, hypernatremia has been associated with ICU stays over three times longer than those of patients who did not develop hypernatremia. 4
Altered electrolyte levels have well-established implications for brain function, which may be especially relevant in older adults who also have COVID. Sodium perturbations are the electrolyte disturbances that most often lead to changes in neurologic function as sodium concentrations affect fluid shifting, leading to swelling or shrinkage of brain tissue. 8 Some have reported that one manifestation of COVID-19 appears to be marked and difficult-to-treat hypernatremia, 4 with overly rapid electrolyte correction possibly precipitating osmotic demyelination syndrome.
In a postoperative setting, electrolyte disorders have been positively correlated with risk of developing delirium. 9 Similar similar changes in electrolytes due to COVID-19 may also lead to this outcome. Furthermore, we note that increasing age is relevant to this clinical picture because age is already associated with a higher risk of developing delirium. 10 In this retrospective study, we focused on the interaction between electrolyte abnormalities during the course of COVID infection and incidence of delirium in geriatric subjects.
Methods
For this retrospective cohort study, we performed a review of EMRs of deidentified patients with cognitive impairments and gathered data on instances of COVID and non-COVID pneumonias. Cognitive impairment was defined as documentation in the electronic medical record of a pre-existing diagnosis of dementia, mild cognitive impairment, or other chronic neurocognitive disorder, or as evidenced by a Mini-Mental State Examination (MMSE) score <24, when available. 11 COVID-19 pneumonia was defined as a positive SARS-CoV-2 RT-PCR test result in conjunction with clinical and radiographic evidence of pneumonia. Non-COVID pneumonia was defined as negative SARS-CoV-2 testing and a clinical diagnosis of pneumonia supported by radiographic and laboratory findings EMRs of hospital admissions excluding hospice, comfort care, and ICU populations were accessed from a university hospital database dating from January 7, 2018 to January 5, 2021 (Figure 1). The data were further analyzed for presence of electrolyte imbalances measured via basic metabolic panels and entries of delirium recorded in the EMR. Inclusion criteria were age 65 years, all races and ethnicities, all genders, and presence of COVID or non-COVID pneumonias during a one-year period. The threshold for the term “geriatric” aligns with common clinical usage and the United States Census Bureau definition of “older adult.” Subjects were excluded if electrolyte values were not recorded or records were otherwise incomplete. The IRB number for the study is 262052.

How the study population was obtained from an initial set of EMRs of deidentified patients seen in the period dating from January 7, 2018 to January 5, 2021.
Statistical analysis
A total of 625 patients were identified, of which n = 319 had COVID pneumonia and n = 306 had non-COVID pneumonia. Patient populations were chosen from EMRs from a total of 3410 subjects. Counts were performed for instances of delirium and/or hypernatremia before, during, or after a diagnosis of either COVID pneumonia or non-COVID pneumonia. The non-COVID pneumonia group was used as a control group. Timeline of disease presence was determined by date of diagnosis in the EMR. Data analysis and generation of p-values were performed using a Chi-Squared test with categorical data comparing subsets within COVID and non-COVID groups. Comparisons were made within and between groups to evaluate differences in the frequency of outcomes. A p-value <0.05 was considered statistically significant. Crude risk ratios were calculated directly from 2 × 2 contingency tables comparing the frequency of delirium in patients with and without specific electrolyte abnormalities. No regression or multivariable analyses were performed.
Results
Delirium and specific electrolyte disturbances
There was no statistically significant difference in the frequency of delirium between COVID versus non-COVID patients. It was only when hypernatremia was observed during COVID pneumonia or non-COVID pneumonia that delirium was more likely to occur during the illness as well. In the patients with both COVID and delirium, 20/128 had concurrent hypernatremia (Figure 2(B)). In contrast, in the patients with non-COVID pneumonia and delirium, 9/106 had concurrent hypernatremia (Figure 2(E)). Figure 2(A), 2(C), 2(D), 2(F) did not reveal significant findings. Differences between these patient populations are shown in Figure 3.

Number of patients with delirium either before, during, or after COVID (A, B, C) or non-COVID pneumonia (D, E, F), and when they experienced hypernatremia in relation to either COVID or non-COVID pneumonia.

Schematic of electrolyte imbalance counts during COVID and non-COVID delirium.
We found that older adults with COVID pneumonia had an increased propensity for hypernatremia during acute delirium as compared to adults with non-COVID pneumonia. There was a greater frequency of hypernatremia overall (with or without delirium) in COVID groups (p < 0.0321).
General electrolyte disturbances
A higher percentage of patients with non-COVID pneumonias suffered from electrolyte imbalances overall (such as hyper- and hypokalemia) versus those with COVID pneumonia (p < 0.001). 173/306 subjects with non-COVID pneumonias had electrolyte disorders at some point, compared to 127/319 (39.8%) patients in the COVID group.
Hypokalemia was the single most represented electrolyte disorder in both groups. Hypokalemia was also more frequently identified in non-COVID patients versus COVID patients: 56/306 (18.3%) versus 34/319 (10.6%) (p < 0.006), respectively. In the COVID group, 58 of the aforementioned 127 (45.7%) had experienced hypokalemia at some point (Figure 4). In the non-COVID group, 75 of the aforementioned 173 had hypokalemia at some point (Figure 5).

Schematic of electrolyte abnormalities in the COVID patient subjects.
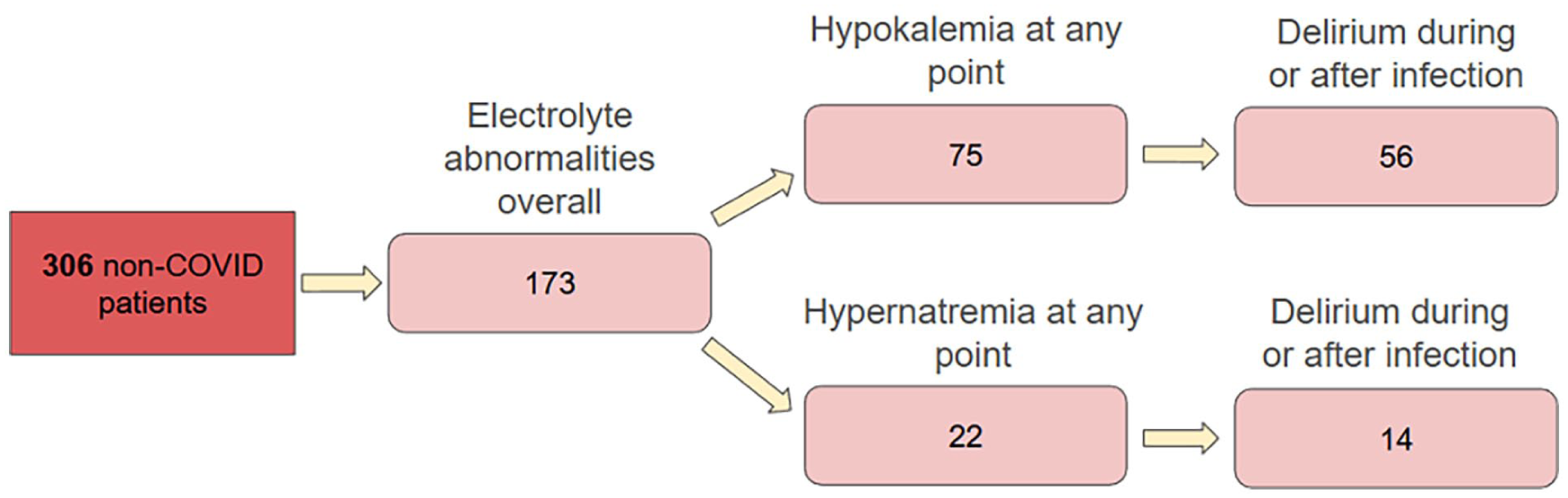
Schematic of electrolyte abnormalities in the non-COVID patient subjects.
Of the COVID patients who experienced hypokalemia at some point, 34/58 (58.6%) also had delirium during or after. Of the non-COVID patients who experienced hypokalemia at some point, 56/75 (74.7%) also had delirium during or after. We compared this 58.6% to an incidence of 36.7% for delirium without hypokalemia. The crude risk ratio for development of delirium with a history of or concurrent hypokalemia was 1.60. Patients who had hypernatremia at some point during COVID infection had an incidence of delirium during or after infection of 87.9% compared to an incidence 33.2% for delirium without hypernatremia. The risk ratio for development of delirium with a history of or current hypernatremia was 2.65.
The difference in risk ratios between development of delirium with hyperkalemia and hypokalemia during COVID infection suggests that hypernatremia poses a higher risk for progression to delirium in geriatric patients.
In total, 128/319 COVID patients had delirium during or after COVID, and 88 of these patients had heart disease. Another observation and possible source of future investigation was that delirium during COVID infection was more common in patients with heart disease compared to patients without (p < 0.00001). It is known that potassium has cardioprotective effects, 12 and the literature supports an association between COVID and electrolyte disorders; it may be interesting to further explore the relationship between these variables.
Information on other electrolytes
At some point before, during, or after COVID infection, 21 patients in the COVID group had hyponatremia, while 22 patients had hyperkalemia. 7 patients had hyponatremia during COVID. 9 patients of these 21 had an episode of delirium during the course of infection with hyponatremia either preceding or concurrent with the delirium. Of the 22 patients in the COVID group with hyperkalemia at some point, 13 had hyperkalemia during COVID. 13 of these 22 patients also had an episode of delirium during the course of infection with hyperkalemia either preceding or concurrent with the delirium.
Discussion
Electrolyte imbalances in general (such as hyper- and hypokalemia) were more common in the non-COVID versus COVID group. The higher frequency of hypernatremic episodes in COVID pneumonia patients as compared to non-COVID pneumonia patients suggests that COVID patients may be especially susceptible to hypernatremia. In a 2020 case series by Zimmer et al., it was reported that hypernatremia appeared to be a manifestation of COVID-19 in 6 of 12 critically ill infected patients and led to a poorer prognosis and longer ICU stay. It was also found that surviving patients with hypernatremia required prolonged mechanical ventilation, possibly as a result of the hypernatremia. 4 However, the underlying reasons for hypernatremia in COVID infection will need further evaluation.
Dehydration is a major cause of hypernatremia in general, as are high fever and bacterial sepsis. 13 As patients in this dataset had all been hospitalized, fluid management would likely have been adequate but may have been lacking for various reasons. To add to the context for this specific patient population, nursing home neglect can lead to or exacerbate electrolyte disturbances, as fluids may not be readily available and labs may not be performed or interpreted in a timely manner.14,15 Dehydration-induced hypernatremia is entirely avoidable; special care should be taken to maintain hydration status in older patients.
Building upon a previous abstract on this topic, 16 we sought to expand our analysis and contextual understanding of electrolyte disturbances in older adults with COVID versus non-COVID pneumonias. Hypokalemia was the most commonly observed electrolyte imbalance overall. Hyponatremia and hyperkalemia were not as frequent as hypernatremia or hypokalemia in our dataset; it was difficult to extrapolate meaning from small numbers. Patients with COVID who had a history of hypernatremia were 2.65 times more likely to develop delirium, as opposed to 1.60 times as likely with hypokalemia. This suggests that incidence of hypernatremia leads to higher susceptibility to developing delirium compared to hypokalemia. However, it is important to note that the sample was limited to EMRs from one hospital system, and using more patients from multiple hospital systems would be beneficial for reducing sampling error and assessing actual significance of trends. Moreover, this was a retrospective study of deidentified patients, meaning that key information illuminating these complex relationships may have been lost. Finally, the sample size was not justified using a targeted power analysis or specific heuristic; data were collected only based on fulfillment of exclusion and inclusion criteria.
There are a multitude of future directions involving electrolyte imbalances in geriatric COVID patients. Our findings of increased hypernatremia during the course of COVID may impact guidelines for electrolyte supplement protocols and general management of electrolyte imbalances. In addition, the geriatric patient population has a higher prevalence of chronic comorbidities, and further investigation of how electrolytes are affected by kidney diseases, diabetes, and congestive heart failure, for instance, could benefit recovery in future COVID cases. Our findings aid the investigation of COVID’s effects on electrolyte balance in patients taking electrolyte-altering medications such as diuretics or laxatives. Other avenues for further investigation include the interaction of electrolyte imbalances with COVID vascular inflammation as well as innovations in predictive biomarkers for future risk in these patients. There has been much headway in unraveling the implications of the pandemic, and these efforts continue for the betterment of clinical practice and improvement of patient outcomes.
Conclusion
This retrospective cohort study highlights a pattern of electrolyte disturbances in older adults with COVID-19, in particular the increased incidence of hypernatremia. While hypokalemia was more frequent overall, especially in non-COVID pneumonias, hypernatremia in COVID-19 patients posed a greater risk for developing delirium, with a 2.65-fold increased likelihood. These findings underscore the importance of close monitoring of sodium and other electrolytes in hospitalized older adults with COVID-19, as doing so may help reduce the risk of neurologic complications such as delirium.
Footnotes
Acknowledgements
Thank you to Dr. Gohar Azhar, Amanda Pangle, Dr. Jeanne Wei, and the Wei Lab at the University of Arkansas for Medical Sciences. We greatly appreciate your guidance and contributions. The project described was supported by the Translational Research Institute (TRI), grant UL1 TR003107 through the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Ethical considerations
This study was reviewed by the Institutional Review Board and determined to be exempt under 45 CFR 46.101, category 4c on January 27, 2021 (IRB# 262052). Per this exempt determination, written informed consent was not required because the study involved secondary analysis of deidentified data. The IRB permitted limited access to protected health information (PHI) for data abstraction prior to deidentification. For participants identified with a diagnosis of dementia, the following PHI could be recorded if available: medical examination data, cognitive testing and depression scales, hospitalizations, falls, problem list, and medication list. All the data used for analysis were fully deidentified before inclusion in the study dataset. This study was reviewed and determined exempt by the IRB under 45 CFR 46.101, category 4c.
Consent to participate
Per the IRB’s exempt determination, written informed consent was not required, as the study involved secondary analysis of deidentified data.
Author contributions
Milenko Petrovic and Esther Park contributed equally as co-first authors. Both were involved in study conceptualization, methodology, data collection, analysis, and drafting of the article. Azhar Gohar and Jeanne Wei contributed to data interpretation and critical revision of the article. Azhar Gohar provided supervision, guidance, and final approval of the version to be published. All the authors read and approved the final article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Statement of Waiver
This study was reviewed by the Institutional Review Board (IRB# 262052) and classified as exempt, category 4c, on January 27, 2021, in accordance with 45 CFR 46.101. The IRB allowed limited access to protected health information (PHI) for the purposes of data abstraction prior to deidentification. For participants with a dementia diagnosis, the following data could be recorded if available: medical examination data, cognitive testing and depression scales, hospitalizations, falls, problem list, and medication list. All the analytic data were deidentified prior to use in this study. The Institutional Review Board name is Jennifer Conley.