
Abstract
Background:
The objective of this study was to evaluate the risk of femur intertrochanteric fracture associated with femur trochanter major fractures in patients over 65 years of age with magnetic resonance examination for better diagnosis and treatment.
Methods:
Thirty-one patients who had incomplete femur intertrochanteric fracture diagnosed were included in the study. Patients were classified according to the length of the fracture line crossing the intertrochanteric border. Fracture patterns were described on magnetic resonance imaging coronal views. Group A, pattern 1, greater trochanteric fracture extends to intertrochanteric region with both cortices; Group B, pattern 2, fracture has characteristics of pattern 1 fracture including diametaphysis fracture line; Group C, pattern 3, greater trochanteric fracture only has extending superolateral cortex fracture line of intertrochanteric region; and Group D, pattern 4, fracture has characteristics of pattern 1 fracture and including superior extension to the baso-cervical line. Surgical treatment with dynamic hip screw was applied to all patients with intertrochanteric extension after magnetic resonance examination.
Results:
This study included 16 women (80.3 ± 6.7 years) and 15 men (76.9 ± 10.94 years). Group A had 11 patients, group B had 8 patients, group C had 6 patients, and group D had 6 patients. Ambulation was initially prescribed for these patients 1 day after the surgery. The average surgery durations of the A, B, C, and D patterns were 44.54 ± 7.56, 49.37 ± 12.65, 49.16 ± 3.76, and 44.16 ± 5.84 min, respectively. No statistically significant differences were observed among the four patterns (P = 0.404).
Conclusion:
Surgical treatment of the greater trochanteric fracture which is considered an indicator of occult intertrochanteric fracture is a good choice for the treatment because of the procedure safety and early mobilization after the surgery
Introduction
Hip fractures are still major public health problem in elderly. They have also medical, social, and psychological side effects. 1 Acute hip fractures are most often visualized initially on radiographs at the emergency department. Magnetic resonance imaging (MRI), due to its reliability, is the first choice to diagnose the acute hip fractures that are not seen on the X-ray views.2–4
The intertrochanteric fracture (ITF) is one most seen in the elderly hip fractures, and its incidence has been gradually seen in recent years with an increase in the elderly population.5,6 Hip pain and limitation of the range of motion of the hip in elderly population after falls should be suspected for an occult hip fracture even though fractures are not observed on plain radiographs. Since the intertrochanteric region is more prone to fracture displacement during walking, the detection of occult fractures is very important in terms of preventing complicated fractures. 7
Our study aimed to evaluate the risk of ITF associated with femur greater trochanteric (GT) fractures in patients over 65 years of age with MRI examination for better diagnosis and treatment. To characterize the frequency of occult ITF in patients with preexisting radiographic evidence of isolated GT fracture.
Materials and methods
This retrospective research study was approved by institutional review board. Written informed constant to participate was obtained from all patients in the study. The medical records of patients older than 65 years who presented with an isolated GT fracture between January 2015 and June 2018 were evaluated retrospectively in a single-center orthopedic center. Patients who had GT fracture with occult ITF fractures were included in the study.
The inclusion criteria were isolated GT fracture diagnosed on plain radiograph, computer tomography (CT), and MRI evaluation of the hip. The exclusion criteria were absent GT fracture on the radiograph (isolated fracture GT on MRI), visible GT fracture with an associated femoral neck fracture, poor quality radiographs, younger than 65 years of age, pathologic fractures, intertrochanteric femoral fractures on plain radiographs, lesser trochanteric fractures on plain radiographs, and <6 months of follow-up. This study was approved by the Institutional Review Board/Ethics Committee with the number 2019/17073117-050.06.
In the 31 hips that were performed surgical treatment with dynamic hip screw (DHS) after the diagnose of the occult ITF.
All radiographs were evaluated by a musculoskeletal radiologist and a senior orthopedic surgeon. The subsequent MRI and CT scans were assessed to diagnose true intertrochanteric extension.
Patients were classified according to the length of the fracture line crossing the intertrochanteric border. Fracture patterns were described on MRI pictures regarding to the describe of the previous authors (Figures 1–4). 8

Group A, pattern 1, GT fracture extends to intertrochanteric region and its lateral and medial cortices.

Group B, pattern 2 fracture has characteristics of pattern 1 fracture plus extension of fracture to diametaphysis.

Group C, pattern 3 GT fracture only extends to superolateral cortex of intertrochanteric region.

Group D, pattern 4 fracture has characteristics of pattern A fracture plus superior extension of fracture to base of femoral neck.
We classified patients into four groups as follows: Group A, pattern 1, GT fracture extends to IT region with both cortices (11 patients) (Figure 1); Group B, pattern 2, fracture has characteristics of pattern 1 fracture including diametaphysis fracture line (8 patients) (Figure 2); Group C, pattern 3, GT fracture only has extending superolateral cortex fracture line of IT region (6 patients) (Figure 3); and Group D, pattern 4, fracture has characteristics of pattern 1 fracture and including superior extension to the baso-cervical line (6 patients) (Figure 4).
Surgical treatment with DHS was applied to all patients with intertrochanteric extension after MR examination (Figure 5). Ambulation was initially prescribed for these patients 1 day after the surgery.

Operated intertrochanteric fracture with dynamic hip screw.
Statistical analysis
The data distribution of each group was tested for normality with the Kolmogorov–Smirnov test. Continuous data are expressed as the mean ± standard deviation when the normality of the data was assessed. Comparisons between the groups were performed with the Mann–Whitney U test. For all the continuous variables, differences were considered to be significant for P values of < 0.05. A post hoc power analysis was provided according to the primary outcome of the study.
Results
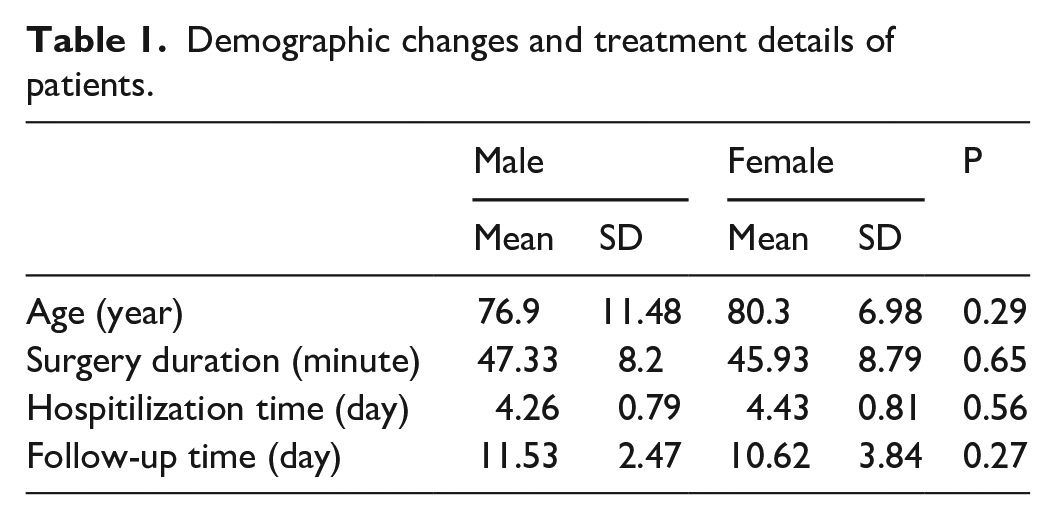
Four-hundred thirteen patients with hip fracture were evaluated in our emergency department. Overall, 40 patients had isolated GT fractures on direct X-ray and CT evaluation. Of these, 31 patients were older than 65 years of age. Overall, 31 patients were diagnosed with incomplete ITF by using MRI (Figure 3). This study included 16 women (80.3 ± 6.7 years) and 15 men (76.9 ± 10.94 years) (Table 1).
Demographic changes and treatment details of patients.
There were no complications after the surgery, and earlier fully weight-bearing ambulation was achieved.
The mean surgery durations in men and women were 47.33 ± 8.20 min and 45.93 ± 8.79 min, respectively.
The average surgery durations of the A, B, C, and D patterns were 44.54 ± 7.56, 49.37 ± 12.65, 49.16 ± 3.76, and 44.16 ± 5.84 min, respectively. No statistically significant differences were observed among the four patterns (P = 0.404) (Table 2). No surgical complications occurred in the operated patients, and no blood transfusion was required. Advantages and disadvantages of the both treatment options were described in the Table 3.
Comparison of surgical time in four different patterns.

Comparison of the methods between two treatment choices.

Discussion
Patients with an isolated fracture of GT can have a broader fracture extending into the intertrochanteric region than that diagnosed by standard radiographs. We recommend that all patients presenting with an isolated GT fracture on the plain radiographs should undergo MRI examination. And the patients who have intertrochanteric extension require surgery.
The pattern of isolated fractures of the GT differs according to the age. In the emergency department, hip fractures are diagnosed with clinical history, patient evaluation, and radiological examination with X-ray views. If the diagnose is an isolated GT fracture of the femur, the pain may be minimal or may have no pain. However, if the patient has severe symptoms then additional radiological examinations may be needed. Occult ITFs increase the likelihood of fracture displacement, thereby increasing the proportion of surgical treatments and significantly decreasing the patient’s activity. Failure to diagnose the fracture with X-ray examination can result in the displacement of previously non-diagnosed fracture; hence, this situation can need complicated surgery, longer hospital stay, and delayed ambulation. 9
Some studies researched that whether fracture line propagations abutted or extended beyond one or both intertrochanteric cortexes. They reported that displaced or non-displaced fractures did not affect the decision to perform surgery.10–12
Failure to diagnose extension of GT fractures into the femoral neck can cause displacement of a previously non-displaced fracture, leading to more complicated surgery, delayed rehabilitation, and prolonged hospitalization. 13
In particular, the top of the GT is not resistant to the forces against.14–16 Although primary muscles are known as abductors and abductors for displacement of this region, external or lateral rotators are also very effective.17,18 In addition, the expected displacement patterns are based on the location of the muscles on the bone structure. 15 Some authors reported that from the external rotator muscles, the gluteus minimus avulses the anterosuperior part of the trochanter, and the gluteus maximus avulse the posteroinferior part of trochanter. 17 In addition, some authors reported that the gluteus medius avulses the entire trochanter alone or in combination with other gluteal muscles.15,16 Since the gluteus medius stands directly on the fracture line formed in the intertrochanteric region, it is thought to be against displacement rather than contributing to the displacement of fracture fragments by contraction. However, the theories reported so far do not consistently overlap in routine radiographs. Because displaced fragments in all age groups are similarly displaced upward, backward, and inward. 12
Ecchymosis may not be observed in patients. Radiologically suspected but lack of leg length mismatch on examination may result in incorrect interpretation of GT fractures as coccytis or pertrochanteric bursitis. Moreover, the absence of expected acute physical findings, coupled with the underestimation of the degree of fracture detected on radiographs, significantly affects the treatment protocol of patients and restricts mobilization.12,19
In a previously reported study, it was reported that ITF was only diagnosed precisely in MRI and that only 50% of fractures crossing the midline in the coronal plane were operated. 9 Since MRI findings are very important in the diagnosis phase, they can change the protocols and treatment costs in the treatment of these fracture types. In addition, it can reduce delayed treatments by taking a very important role in the treatment of fractures not diagnosed in the elderly population. MRI is a solution to the questions regarding the safety of the treatment since plain radiographs cannot show the geographic extent of the lesion in femoral GT fractures.9,12 MRI examination is more expensive than plain radiographs. However, it provides a rapid and anatomically accurate diagnosis of occult hip fracture normally detected on plain radiographs. 20 Studies focused on the importance of MRI in the diagnosis of hip fractures that have not yet been diagnosed.21,22 A study reported that the occult ITF can only be confirmed with MRI, and other radiological methods have failed in this regard. 9
Clinical history, physical examination, and radiographic evaluation are a classic approach in the diagnosis of proximal femur fractures. Severe hip pain detected in patient evaluation leads to additional examinations such as CT or MRI in patients with isolated GT farctures. MRI is a very sensitive radiological examination to diagnose the bone marrow edema. However, we believe that some patients with isolated GT fractures undergo unnecessary radiological scans in terms of radiation exposure and cost. As a result of some studies, it was reported that all patients diagnosed with isolated GT fracture should be treated with surgical intervention regardless of fracture pattern. 23 They stated that in undiagnosed GT fractures, hip joint motion and weight bearing caused the fractures to extend into the intertrochanteric region. They reported that, with the loss of fracture hematoma, typically after fracture displacement, this patient group was subjected to more difficult surgical interventions and even could be treated with hemiarthroplasty.
On the other hand, some studies suggest that surgical treatment is necessary when a midline is drawn between large and small trochanter, when the fracture line crosses this midline on the MRI T1 coronal plane.9,11 In a study, the fracture line detected in MRI extends more than half of the longitudinal axis; surgical intervention is required for these patients because of the increased load on the inner layers of the cortical bone, as there will be a high risk of displacement in this fracture. 24 A study reported the importance of early surgical treatment and ambulation due to the risk of displacement in occult ITF. 12 A study reported that a patient who underwent surgical intervention after displacement of the displaced ITF was not applied MRI because of a pacemaker. 25
Chung et al. 7 reported that patients who were followed up conservatively had applied with displaced ITF on the 9th day of the treatment, and that patients who were followed up conservatively should be followed knowing this big risk. However, there is no consensus in the literature on the treatment of isolated GT fractures. Because these fractures are seen very rarely and sufficient studies on treatment selection are not yet available in the literature. Almost all hip fractures presenting to the emergency department are diagnosed by routine plain X-rays. 26 However, an undiagnosed occult ITF fracture can lead to risk of displacement, longer hospital stay, and delayed ambulation.27,28 Therefore, the necessity of surgical treatment may occur in a GT fracture that seems simple on plain radiography. 29
However, in our study, we showed that these fractures may have a larger fracture extending to the intertrochanteric region, and these cannot be diagnosed using standard plain radiographs. The decision to manage these fractures non-surgically should be carefully considered, as a trochanteric fracture with early weight bearing and the hip joint motion can lead to a fully displaced fracture. Recently, a simple displacement of the GT fracture and a displaced ITF have been reported after the initial diagnosis of delayed surgery. 8
All patients in our study had surgical treatment with DHS application. Proximal femoral nail (PFN), which is used more frequently in the surgery of ITFs in recent years, was not preferred. Although Occult ITF has PFN applied publications, it was seen that distal locking screws were used as a standard treatment.21,22 In stable ITFs, DHS and PFN have proven not to be superior to each other. 30 DHS was preferred in our study because compression in DHS was more pronounced than PFN and it was a cheaper implant for the treatment.
In our study, no postoperative complications were observed in any of the 31 patients who were operated on with the diagnosis of occult ITF. Patients were treated surgically, and ambulation was achieved by giving them an early or full of weigh-bearing. We believe that the use of MRI is very important in the diagnosis of these fracture types and that early ambulation with surgical treatment can prevent possible complications related to non-surgical treatment. At the same time, we believe that the failure to diagnose these types of fractures can lead to displacement of a fracture that has not been displaced before, resulting in more complex surgery, delayed rehabilitation, and long-term hospitalization. Moreover, no blood transfusion was required. This study revealed that shorter surgery duration and early rehabilitation in patients who underwent surgery. This study observed that the operative durations were short, and fully weight-bearing ambulation could be performed on the first postoperative day, especially in elderly patients. Nevertheless, in patients with GT fractures, older than 65 years of age, direct surgery without early MRI and early mobilization after surgery would be an appropriate approach.
The limitations of our study can be shown as the limited number of patients, there was no control group who had non-surgical treatment, and the retrospective design. However, the desired levels could not be achieved in the number of patients and in the control group due to the difficult to diagnose or skippable fracture pattern and patients who were recommended non-surgical treatment were out of follow-up. We believe that our numbers of the occult fracture are good enough despite the difficult diagnose of these fractures.
Conclusion
We concluded that particularly in elderly patients, surgical treatment of the GT fracture which is considered an indicator of occult ITF is a good choice for the treatment because of the procedure safety and early mobilization after the surgery.
Footnotes
Author contributions
All authors participated in the design, interpretation of the studies, analysis of the data, and review of the manuscript. B.E.K. and Y.O. did the design of the study and drafted the manuscript. A.V., O.A., S.A., and EAY reviewed the patients and analyzed the data. B.E.K. wrote the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional Review Board/Ethics Committee with the number 2019/17073117-050.06 according to the ethical principles stated in the Declaration of Helsinki.
Informed consent to participate
Written informed consent was obtained from all subjects before the study.
Informed consent for publication
The participants declare that they agree to publish the data described in the manuscript.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.