
Abstract
Background:
The purpose of the described exploratory study was to test proactive strategies for enhancing engagement and cognitive ability while diminishing dementia-related disordered behaviors of those diagnosed with Alzheimer’s disease and other dementias. Study participants resided in an Memory Care unit of an assisted living community.
Method:
The researchers measured the effects of exposure to music and nature images on engagement using the Individualized Dementia Engagement and Activities Scale tool, on cognitive ability using the Montreal Cognitive Assessment, and on agitation using the Cohen-Mansfield Agitation Inventory.
Result:
The within-subject study design revealed that use of both music and nature images hold promise for reducing undesirable behaviors and improving engagement of residents.
Conclusion:
The authors suggest caregivers for those with Alzheimer’s disease and other dementias can effectively use nature images and music to improve engagement and reduce disordered behaviors, thus potentially enhancing quality of life for the care recipient as well as the caregiver while possibly reducing the costs of medications used to control dementia-related undesirable behaviors.
Introduction
Upon entering a unit where elders with dementia disorders reside, non-caregivers are frequently met at the entrance by sleeping residents slumped in their wheel chairs, elders exhibiting repetitive behavior without known cause or effect, and perhaps ranges in behavior from happy and cheerful with sudden change to screaming or sobbing. Elders with Alzheimer’s disease and other dementias (ADOD) have a decline in cognitive functioning, which can result in an inability to process and receive information from their environment. 1 This reduced ability to interpret and react to stimuli can result in individuals with ADOD becoming disengaged with their environment or exhibiting problem behaviors such as agitation. Currently, the primary approaches to reduce undesirable behaviors are pharmacological even though these approaches have shown only a moderate effect on patient outcomes.2,3 Another limitation of pharmacological approaches is that they do not address some of the underlying reasons for undesirable behaviors, such as social isolation, depression, boredom, or sensory deprivation, leading to lack of engagement. 4 Recent concerns about adverse side effects and drug interactions of pharmacological approaches, in addition to the safety issues of wandering elders, have led to an increased interest in the use of non-pharmacological approaches.1,5
Research using non-pharmacological therapies, such as light therapy, physical exercise, music therapy, and preferred music listening, has shown promising results indicating a viable and cost-effective method for managing the behavioral problems associated with ADOD.1,6,7,8 Music listening has been specifically associated with decreased levels of agitation and improved mood. Researchers found that when making comparisons between an experimental and control group, recorded, personally preferred music decreased 12 of 15 occurrences of identified aggressive behaviors by individuals with Alzheimer’s disease during bathing,9,10 and another study revealed that preferred music improved mood and reduced agitation during bathing. 11 Nature views also have promise for reducing undesirable behaviors as they have been shown to reduce stress, anxiety, and pain,12–19 which can manifest in undesirable behaviors of those with ADOD.
Increasing engagement can reduce incidence of undesirable behaviors. For this study, engagement was defined as interested, connected, and willing to live in a world with activities the elder enjoys and for which they receive satisfaction. Researchers have found that engagement contributes to the relative well-being of those with ADOD.20,21 Music activities have proven effectiveness as a method of engagement for those with ADOD11,22 and viewing nature images has been shown to improve executive function attention in older adults, 23 suggesting promise for those with ADOD.
The overall purpose of the exploratory study described in this article was to explore how exposure to preferred music and nature images affected engagement, cognitive ability, and dementia-related disordered behavior such as agitation for those diagnosed with ADOD. The project supports comparative effectiveness research (CER) and outcomes research by identifying the benefits and harms of alternative methods (music and nature images) to treat dementia-related undesirable behaviors, thus improving the delivery of care and possibly delaying and/or reducing costs of psychotropic medications used in hospital and nursing home settings for reducing such behaviors. Using standardized sorting protocols, study participants first indicated preferred nature images and music recordings, which were then used in interventions during which their cognition, engagement, and agitation were measured by various tools that were previously assessed for their appropriateness and feasibility for use with ADOD patients.
Methods
This study used a within-subject design and was conducted in an assisted living community with 300 residents including a maximum of 48 individuals in assisted living, 24 in Memory Care, a designated care unit for persons diagnosed with ADOD (12 in one area and 12 in the second area), and 44 receiving short-term rehabilitation and long-term care. For this exploratory study, all residents were assigned to either Groups 1 or 2 based on their Memory Care living area. Because of the ADOD diagnosis for these residents, the researchers wanted to limit introduction of variables, so the participants remained divided into two groups of persons with whom they saw and/or interacted everyday.
All of the 24 residents of the Memory Care unit with consent from their legally appointed representatives (LAR) were eligible for the study. Approval was received from the Institutional Review Board of Greenville Health System and endorsed by Clemson University Institutional Review Board for the study to be conducted. All potential participants had a Folstein mini-mental status exam (MMSE) score less than 10, indicating severe dementia, prior to study participation. The participants’ designated dementia phase was not specified in the medical record available to the researchers. The LAR of the 24 individuals living in the Memory Care unit were invited, via letters and follow-up phone calls from Memory Care staff, to attend one-hour educational meetings that included description of the research activities and review of the consent form with time available for questions and answers. In total, 14 LARs consented for their family member to participate in the research, and each designated participant was assented prior to each intervention/activity. One resident passed away prior to initiation of the study, and of the remaining 13 individuals, 11 assented to participate in a sorting process to choose preferred nature images while 6 assented to participate in the process to select preferred music. Two of the participants assented to choose their preferred music, but did not participate in the pre-intervention activity. Later, they also dissented to participate in the post-intervention activity, but desired to meet with the study coordinator to receive assessment post-intervention. In order to reduce possible anxiety for the study participants from interacting with more than one unfamiliar person, the study coordinator implemented all study activities, including data collection. A geriatric nurse practitioner (GNP) was available during both the nature and music sorting procedures and discussed approaches to maintain a calm and comforting environment during data collection. The study coordinator had previous experience with mental health patients and discussed with the GNP any verbal or non-verbal communications by participants indicating opposition to participation in study activities. These oppositions were interpreted as dissents and resulted in a reduced number of participants during the music phase of the study (Figure 1).
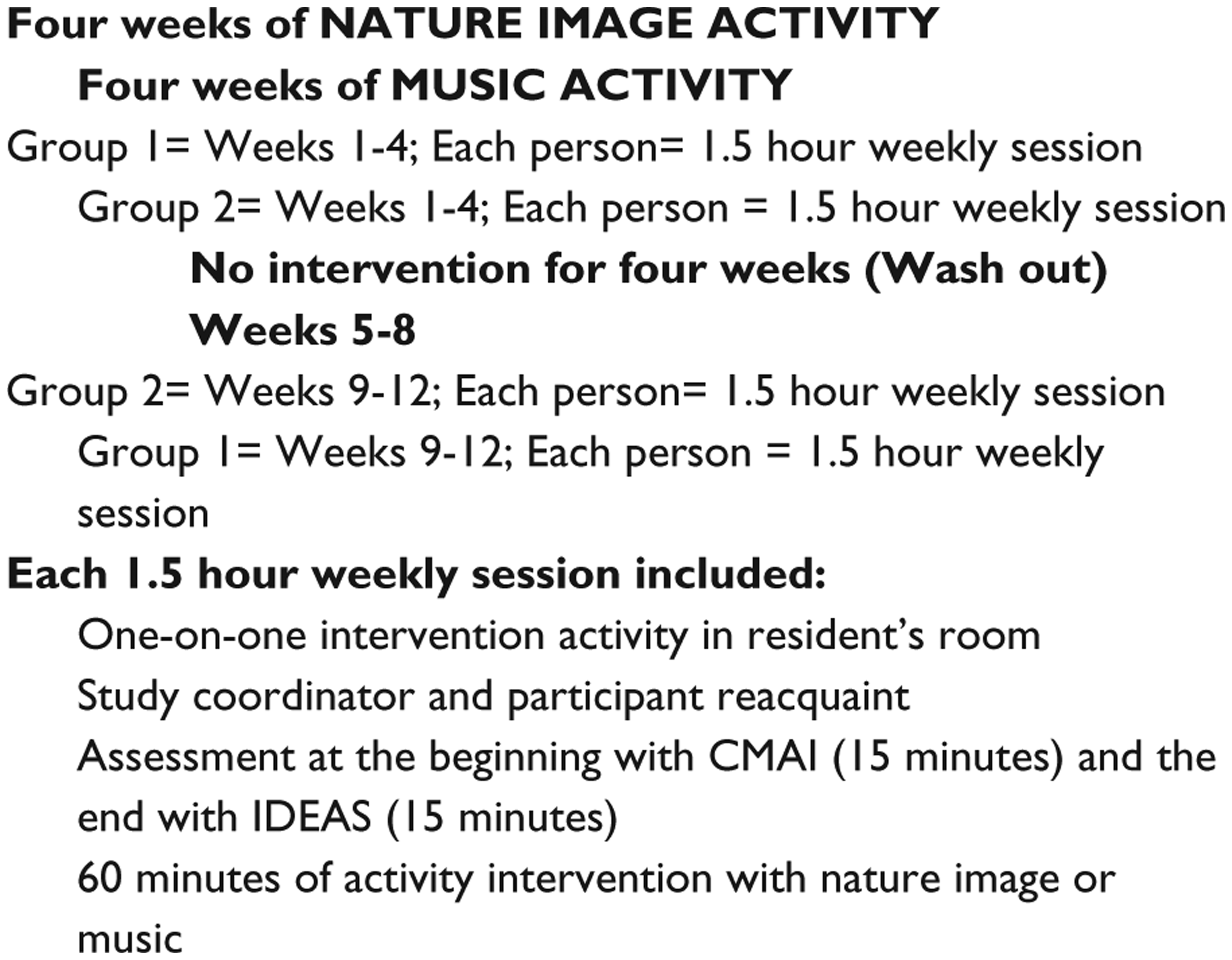
Protocol for measuring effects of nature images and music on elders with ADOD.
Nature image sorting
Nature images were selected using a sort and rank task based on Appleton’s prospect refuge theory of landscape preference. 24 This is an evolutionary theory that sorts landscapes into categories of prospect (real or symbolic access to a view), refuge (real or symbolic access to shelter from threats), and mixed prospect refuge (elements of both prospect and refuge are present in the scene). Images identified to category from a previous study on effects of nature images on pain 12 were used in this study.
The study coordinator used a standardized script to conduct the sorting task in a resident-familiar multi-activity room in the Memory Care unit. Four tables and chairs were arranged along the walls with four 8.5 × 11″ nature images lying flat on the surface of each of three tables. Each table contained one image representing prospect, refuge, and mixed categories, while one category was represented twice on each table. The order of images (by category) was randomized for each table. Staff members assisted the study coordinator in identifying and transporting the members to the sorting room. Upon entering the sorting task room, participants were first asked whether they wanted to sit or stand at the first table with the nature images. As they were escorted from table to table, participants were then asked to pick their favorite image out of the four displayed on each table in response to the question, “Which image do you like the best?” If participants did not respond, they were asked “Which image makes you feel happy?” Verbal and non-verbal cues were noted based on the participant’s ability to communicate. An exploratory aspect of this study involved asking the participant whether their preferred image reminded them of a specific place from their past and if so, to describe that memory. This was done because Alzheimer’s patients often retain long-term memory rather than short-term memory, and if a positive correlation was found, it could potentially guide future customized image selection for patients.
To maintain consistency for the demented elders, the selection process was repeated at the second and third tables containing nature images, and then, the preferred images from each of the three tables were placed on a fourth table. Participants were asked to choose their favorite of the three preferred nature images and whether they would like to take that image to their room with them. This favorite image was then used throughout the nature image intervention phase of the study.
Music sorting
In order to maintain consistency for the elders with dementia, the music sorting task took place in the same multi-activity room on the Memory Care unit using a standardized script similar to the one used for nature image sorting. The room was set up with one square card table that held a CD player and a folder which contained images related to four music genres, each with two associated song selections for a total of eight songs. The genres included “Popular,” “Broadway,” “Big Band,” and “Religious” music. The music therapist for the assisted living community recommended the genres and song selections based on published research regarding music preferences of elders 25 and direct knowledge of common music preferences within the community. Participants entered the room and were invited to sit or stand at the table, and then listen to small sections (usually the chorus) of each song. Verbal and non-verbal cues were noted by the study coordinator; these included singing along to the song, tapping hands or feet, and nodding head along to music. After listening to the two songs from a particular genre, participants were asked which song they liked best and given some time to respond. If there was no response, participants were asked which song made them feel happy. Participants were then asked whether the song reminded them of a specific time from their past. The process was repeated for each of the four genres. After a song was selected from the four genres, participants would listen to short segments of the four chosen songs. Participants were then asked to select a favorite song and were provided with a CD containing the complete song to take back to their room.
Intervention activities using preferred nature images and music
Intervention activities were conducted one-on-one in the resident’s room. In total, 90 min was allowed for each session to provide ample time for participants to become reacquainted and comfortable with the study coordinator at the beginning of each session and to provide time for saying good-bye. Part of the session time was used to collect data using the Cohen-Mansfield Agitation Inventory (CMAI) and the Individualized Dementia Engagement and Activities Scale (IDEAS) at the beginning and end of each session which accounted for about 30 min of the 90 min. During the approximate 60 min remaining in the intervention session, the researcher encouraged the participant to look at and discuss the preferred nature image or listen to and/or sing along with the preferred musical selection. Examples of how the study participants interacted with the nature image include the participant showing and describing the image to a doll she usually carried, showing the image to a staff person stopping by and saying things such as “Come look at this picture, isn’t it pretty?,” discussing aspects of the image with the study coordinator such as the “long road” or a “large field ideal for a horse,” telling stories of climbing the tree in an image or of how the tree was in the person’s backyard when she was a child, counting the trees in an image, and how the image reminded them of the state where they once lived. Sometimes participants described items they were seeing in the picture, such as alligators, a snake, or a girl, which were not actually there.
Measures
CMAI
Agitation was measured using the CMAI short form, which is a 14 question instrument that uses a 5-point Likert scale ranging from 1 (never) to 5 (a few times an hour or continuous for half an hour or more). 26 For the short version of the CMAI, inter-rater reliability for three sets of raters in three units of a nursing home was as follows: exact agreement = .82; 0–1 point discrepancy = .93. 27 Inter-rater agreement rates (using 0–1 point discrepancy as agreement) averaged .92 among independent ratings of activity leaders observing elders in community adult day care centers. Analysis of CMAI data can relate to specific behaviors of interest, or on four factors of agitation: Factor 1—physically non-aggressive behaviors, Factor 2—physically aggressive behaviors, Factor 3—verbally non-aggressive behaviors, or Factor 4—verbally aggressive behaviors. 28 For our research, Factor 3 behaviors (aggregate of question 9—constant request for attention or help, and question 10—repetitive sentences, calls, questions, or words) were most common (Table 4). Scores for Factor 3 could range from 2 to 10 with higher scores indicating more frequent observations of the verbally non-aggressive behaviors.
IDEAS
Engagement was measured using the IDEAS tool, which was developed by staff nurses in a long-term care unit and GNP-certified nursing faculty using items identified in the Dementia Care Mapping literature plus geriatric clinical practice experiences. Points are assigned ranging from 1 (no to little engagement) to 5 (high engagement) for eight behaviors including communication, group activities, individual activities, eating, attitude, passive behavior, aggressive behavior, and involvement in care. The number of points for each behavior is summed for a total score. Scores could range from 1 to 40, with higher scores indicating more frequent engagement. Face and content validity of the items was determined by registered nurses with multiple years of experience working with adults with dementia, two certified GNPs with positions in long-term settings, and two geriatric faculty with terminal degrees and nationally recognized expertise in engagement behaviors and/or care of geriatric individuals. This study was the first in which the IDEAS was used over a short interval of time versus an extended period of time, so no reliability is established.
Montreal Cognitive Assessment
The Montreal Cognitive Assessment (MoCA) has demonstrated high test–retest reliability (correlation coefficient = .92, p < .001) and good internal consistency (Cronbach’s alpha .83). Content validity was established via a close correlation between MoCA and MMSE scores.29,30 Participant cognitive functions were measured using the Visuospatial/Executive task (clock drawing) and a Memory task (five-word recall) from the MoCA inventory. Higher scores on each task indicate higher level functioning.
Data collection
Data were collected using two sections of the MoCA (clock drawing and five-word recall), 1 week before and 1 week after both the nature image and music interventions, each of which lasted 4 weeks. Of those 11 participants who completed the nature image sorting, 9 completed the MoCA tasks pre-intervention and 8 completed the tasks post-intervention. Of the six participants who completed the music sorting task, four completed the MoCA tasks pre-intervention and six completed the tasks post-intervention (two of the six participants did not want to complete the MoCA pre-intervention). However, they wanted to listen to the music during the intervention, and when the study coordinator was testing for post-intervention measurements, they approached her to be included in the test. In order to avoid undesirable behavior on the unit, they were allowed to be tested resulting in two more participants in post-intervention MoCA measures than in pre-intervention measures. Minor alterations to the MoCA included using a blank sheet of paper for the clock-drawing task to provide more space and to eliminate distraction of seeing other MoCA tasks.
Data collection with the CMAI and IDEAS occurred at the beginning and end of the 90-min weekly sessions held during the 4-week intervention periods using nature images and music.
Data analysis
Data analysis was completed using IBM SPSS Statistics Version 20 (IBM Corp. 31 ). Descriptive statistics were employed to analyze these data. Pre- to post-intervention results were examined for patterns.
Results
There were nine participants in the nature image 4-week intervention, eight of whom were female. The age of participants ranged from 71 to 93 years, with mean age equaling 83.18 years, standard deviation (SD) = 7.65 years. There were six participants in the music therapy 4-week intervention, five of whom were female. The age of participants ranged from 71 to 92 years, with mean age equaling 80.67 years, SD = 7.71 years.
Results for the MoCA clock-drawing and memory-recall tasks are presented in Tables 1 and 2, respectively. Following the nature image intervention, more individuals received a higher score of 2 points than 1 point on the clock-drawing task, and following the music intervention, more received a higher score of 1 point compared to 0 points. For the memory-recall task, three of nine (33%) scored 2 points or more before the nature image intervention as compared to four of eight (50%) after the intervention. Before the music intervention, none of the four participants scored 2 points or more as compared to two of six (33%) scoring in this range after the intervention.
MoCA clock-drawing results.

MoCA: Montreal Cognitive Assessment.
MoCA memory-recall results.
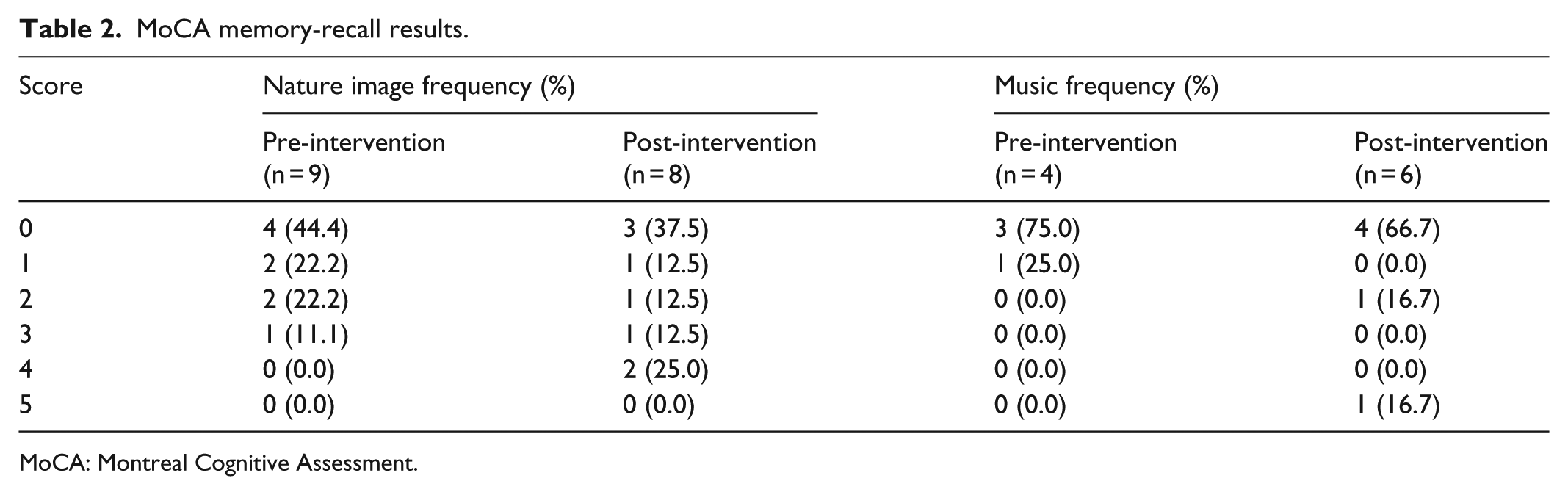
MoCA: Montreal Cognitive Assessment.
With the IDEAS tool, a higher score indicates that an individual is more engaged. When comparing average scores of participants before and after both the 90-min nature image and 90-min music interventions, we found improvements each of the 4-weeks (Table 3).
IDEAS scores: mean (standard deviation).

IDEAS: Individualized Dementia Engagement and Activities Scale.
Music sample sizes: weeks 1 and 2, n = 6; week 3, n = 4; week 4, n = 5.
High-CMAI scores indicate higher frequency of agitated behaviors. For this study, verbally non-aggressive behaviors, as assessed by questions 9 and 10, showed mixed results (Table 4). Scores declined (improved) from pre- to post-intervention in weeks 1 and 3 of the nature image intervention and improved in weeks 1 and 4 of the music intervention.
CMAI verbally non-aggressive behaviors (Q9 and Q10): mean (standard deviation).

CMAI: Cohen-Mansfield Agitation Inventory.
Music sample sizes: weeks 1 and 2, n = 6; week 3, n = 4; week 4, n = 5.
Discussion
Older adults with ADOD are characterized by several symptoms, most notably, memory impairment and cognitive decline, as well as disengagement or neurobehavioral problems (e.g. hyperactivity, inappropriate affect, and aggression). 32 Our exploratory study sought to develop a methodology for use of approaches with nature images and music that may be used with ADOD patients to increase engagement and reduce disordered behaviors such as agitation. Music and nature images are effective positive distractions for reducing anxiety or stress using environmental features or conditions 33 as nature images have proven effective in reducing stress in healthcare settings12,34 and controlled laboratory settings17,18 plus the use of preferred music has shown to be effective in reducing agitation and improving mood during bathing. 11
Our work with using approaches such as nature images and music has promise for increasing ADOD patient engagement and reducing disordered behaviors. For example, the nature image facilitated conversations with patients who referred to aspects of the image and recalled memories from their childhood or a region of the country. We hypothesize that the nature images and music listening improved engagement and provided environmental positive distractions 31 that alleviated some of the boredom, sensory deprivation, and disengagement found to be underlying determinants of disordered behavior. 4
Limitations
Limitations to the study included a small sample size, which reduced the ability to determine statistical significance as well as a lack of a control group or random assignment. In addition, approximately half of the participants were regularly involved in weekly music therapy sessions (some groups, some 1:1). A control group could have differentiated between the effect of the music listening and nature image interventions delivered by a graduate student from that of a graduate student simply engaging in conversation. Another limitation involved the sorting tasks. Although 11 of the 13 assented participants were able to successfully complete the nature image sorting task, 2 participants were unable to complete (dissented) because upon entering the sorting room they became visibly anxious and agitated with one stating, “What is this room?” Although these two participants had minimal verbal communication, both participants clearly indicated that they wanted to leave the room. Staff members differed on explanations for the participants’ distress including the images themselves created too much stimuli for the participants, the sorting task itself was too complicated, and the room was not a familiar place for the participants, even though it was used in the study, because it was frequently used by Memory Care residents for other activities. Possibly, the nature image sorting could have been conducted in the resident’s room, so the participant could stay in their familiar environment.
As with the nature image sorting, participants sorting musical selections appeared cautious of the room containing a single table and chairs with many stating, “What is this room?” Another barrier to the music sorting task was the amount of time required for the task which was 20–30 min, longer than the average time of 10–15 min to complete the nature image sorting task. Participants demonstrated difficulty with focusing on a task for this longer period of time by stating that they had to leave the room and becoming restless. They also appeared to have some trouble focusing on and remembering the specific songs played. This was particularly evident during the music selection task in which participants chose one of four songs within their initially preferred genre selection. Participant’s non-verbal cues, facial expressions, singing along, and tapping to music would show clear preference for one song, and yet the final selection might be another song. We recommend investing time in getting input from family and friends, or from social work, music therapy, or recreation staff, 11 to determine preferred music genres or songs in order to avoid using a sorting process.
Conclusion
Since both interventions showed promise for improving engagement and reducing disordered behaviors of residents with ADOD and require easily obtained and low-cost materials, these researchers believe that they could easily be implemented after minimal training in an institutional setting by formal caregivers as well as in a home setting by an informal caregiver. By improving engagement and reducing disordered behaviors, we believe that these types of interventions could potentially enhance the quality of life for the care recipient as well as the caregiver. In addition, there is potential to reduce the cost of medications used in institutional settings to attempt control of dementia-related undesirable behaviors. Clinical applications of the results could include the ability of healthcare providers to offer practical suggestions to caregivers on how they might better manage disordered behaviors of their care recipient with dementia. Sets of nature images could be provided to the caregiver with simple instructions on how to show each image to the care recipient as a way to prompt discussion and/or engagement. Caregivers might also be directed on how to access popular songs of the years when their care recipient was a young adult or a child as these often seem to stimulate long-term memory and engagement. One of our authors has found that Sunday school songs popular when care recipients were children were also effective in improving engagement. Since care recipient behavioral and psychiatric symptoms can reduce caregiver’s quality of life 35 and increase risk of institutionalization, 36 helping caregivers enhance engagement and reduce disordered behaviors of their care recipient can improve chances that the care recipient can stay in the home longer and reduce costs of institutional care. In summary, we agree with authors of a recent literature review of 18 studies that multisensory stimulation environments produce immediate positive effects on the behavior and mood of people with dementia 37 and support that more standardized methodological protocols are needed. 38
Footnotes
Acknowledgements
Questions regarding how research materials may be accessed can be directed to the first author (J.E.).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study described in this article was funded by the Institute for the Advancement of Health Care, a South Carolina collaboration between the Greenville Health System, Clemson University, and the University of South Carolina. The sponsor did not have any role in the study design, collection, analysis, and interpretation of data; writing of the report; or the decision to submit the article for publication.