
Abstract
Objectives:
Early exercise is beneficial for mechanically ventilated intensive care unit patients. However, there remains a paucity of research data on the pattern of early assisted exercise delivery and the role of active and passive exercise modalities.
Methods:
Herein, we collected 349 mechanically ventilated patients admitted to the intensive care unit of Tianjin First Central Hospital from April 2020 to 2022 and divided them into a control group (176 patients) and an exercise intervention group (173 patients) according to whether or not early rehabilitative exercise was performed.
Results:
The results showed that the maximum negative inspiratory pressure, rapid shallow breathing index, limb muscle strength, swelling index, some clinical physicochemical indexes, the number of days of endotracheal intubation, the use of sedative and analgesic drugs, the duration of delirium, and the final prognosis of patients in the intervention group were all improved to different degrees. Subgroup analyses showed that compound and active movement patterns were more conducive to the recovery of limb muscle strength than single assisted movement patterns, but faced higher consumption of sedative and analgesic drugs.
Conclusion:
Our results suggest that early bedside-assisted exercise is beneficial, but still needs to be matched appropriately to the patient’s condition in order to maximize the patient’s prognosis. Our study provides valuable data to support subsequent clinical practice of early bedside-assisted training and the establishment of relevant guidelines.
Keywords
Introduction
Critical illness appears to be associated with a decline in the functional status and prognosis of the patient’s quality of life. It has become a global adult critical care burden.1,2 Since the development and expansion of the intensive care unit (ICU) began in the 1950s, there has been a significant increase in survival rates for many critically ill and complex patients, accompanied by an increase in the number of acutely ill patients receiving mechanical ventilation (MV).3,4 Approximately 5–6 million patients per year require ICU-level care preceding the SARS-CoV-2 pandemic, just in theUnited States. 5 However, patients mechanically ventilated for more than 48 h in the ICU have rapid skeletal muscle weakness. 6 Consequently, induced complications include malnutrition, increased rates of hospital-acquired infections, altered sleep quality, prolonged hospital stays, and reduced independence in activities of daily living.7,8 Besides, MV intubation leads to communication challenges for quality of care and even negative emotions. 9 Therefore, it is critical to implement early interventions to reduce machine ventilation time in mechanically ventilated patients to promote recovery and improve prognosis.
Early activities are defined as passive or active activities in the early stages of critical care treatment aimed at supporting and maintaining the patient’s mobility. Compared to late activity, there is growing evidence that early physical intervention in the ICU increases ventilator-free days, improves peripheral and respiratory strength, reduces ICU time and length of hospital stay, and improves long-term physical status.10–13 A study by Nydahl et al. 14 showed that early activity reduced the prevalence and duration of ICU delirium, while in another study, they concluded that early activity combined with minimal sedation was safe and well tolerated. 15 However, despite these benefits, there is limited evidence on the role of bedside-assisted exercise and multiassisted exercise in the rehabilitation of mechanically ventilated patients. These interventions are particularly relevant as they can be customized to patient needs and aligned with standardized clinical care requirements. 16
In addition, a variety of factors may interfere with the intervention of early exercise in mechanically ventilated ICU patients, including medical and nonmedical factors. Clinical training programs and guidelines guided by theoretical or practical experience are still needed to implement and maintain early exercise in mechanically ventilated ICU patients.17,18 Ultimately, this demonstrates the ongoing need for prospective studies to supplement the gap between perceptions and actual clinical needs in order to increase the prevalence of ICU mechanically ventilated patients receiving early and appropriate bedside-assisted exercise care, both theoretically and in clinical interventions.
Therefore, in this study, we conducted a prospective randomized controlled trial (RCT) to systematically evaluate the effects of early rehabilitative activities and patterns of rehabilitative activities on the recovery and prognosis of mechanically ventilated ICU patients. The aim was to address these gaps by systematically analyzing the effects of early rehabilitative activities, particularly bedside-assisted exercise and multiassisted exercise, on the recovery and prognosis of mechanically ventilated ICU patients. Using a prospective RCT design, we will compare outcomes such as delirium duration, body function status, medication use, duration of MV, and overall prognosis between intervention and control groups. As a prospective study, the results of this study are expected to provide valuable data to support research on the ameliorative effects of bedside rehabilitation exercises on mechanically ventilated ICU patients.
Methods
Research design and setting
Patients admitted to the ICU of Tianjin First Central Hospital between April 2020 and April 2022 were prospectively recruited into the study within 24 h of ICU admission. Medical records were systematically reviewed during the study period to ensure adherence to inclusion criteria and to collect relevant clinical data. The collection was carried out for inclusion according to the following criteria:
(1) Inclusion criteria:
✓ Age 18–80 years;
✓ MV for more than 2 days (assisted controlled ventilation);
✓ Primary disease-causing respiratory failure was largely controlled (oxygenation index ⩾ 150 (FiO2 ⩽ 0.5, positive end-expiratory pressure ⩽ 8 cm H2O));
✓ Hemodynamic stability was achieved (heart rate ⩽ 140 beats/min, mean arterial pressure ⩾ 65 mmHg, norepinephrine < 0.5 μg/kg-min, and no other vasopressors in use);
✓ Richmond Agitation-Sedation Scale (RASS) ⩾ −2.
(2) Exclusion criteria:
✓ Body mass index > 45;
✓ Preexisting neuromuscular diseases (e.g., myasthenia gravis, motor neuron disease, Parkinson’s);
✓ Rhabdomyolysis, epilepsy, tumors, deep vein thrombosis, open skin, soft tissue injuries, limb fracture;
✓ Currently receiving inotropic medications or vasopressors other than norepinephrine;
✓ Pregnancy;
✓ End-stage of the disease;
✓ Ejection fraction < 30%;
✓ Duration of MV > 90 days;
✓ Patients who had to discontinue the training program because they were intolerant;
✓ Incomplete follow-up information on prognosis (survival) within 660 days.
Thereupon, they were divided into a conventional treatment group (control) and a bedside-assisted exercise intervention group based on a random number table. Due to the exclusion of patients who were unable to tolerate the training, the final sample sizes were 180 and 173 patients, respectively. Despite not receiving early rehabilitation, the control group received standard ICU care, including passive range of motion exercises and postural interventions to prevent complications. Decisions to suspend normal clinical interventions were based on the clinical judgment of the treatment team and were consistent with the current standard of care in the ICU at the time the study was conducted. This approach was approved by the institutional ethics committee as ethically sound and scientifically necessary to assess the impact of early assisted movement.
This study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines, 19 and all methods were performed in strict accordance with the relevant guidelines and regulations, and were approved by the Ethics Committee of Tianjin First Central Hospital (No. 2023DZX11). Verbal informed consent was obtained from all subjects before the study.
Early bedside-assisted exercise protocol
Intervention group
The intervention group underwent different levels of assisted and active rehabilitation training based on the patients’ tolerance, which was defined as the ability to perform the rehabilitation activities without experiencing hemodynamic or respiratory instability, agitation, or impaired consciousness. Patients were assigned to one of three levels (Levels 0, 1, or 2) based on their clinical condition and tolerance, as assessed by the rehabilitation team (Supporting information (SI) Appendix, Figure S1). Once patients improved or became intolerant to the training program, adjustments were made according to the procedure (SI Appendix, Figure S2). The rehabilitation sessions were conducted five times per week during the ICU period. Each session lasted 30 min, with continuous monitoring of vital signs and patient tolerance. The interventions were standardized by using predefined protocols for each level, ensuring consistency across all patients. These protocols included specific settings for electrical stimulation, pedaling intensity, and joint mobilization techniques.
✓ Level 0: diaphragm electrical stimulation + neuromuscular electrical stimulation + joint mobilization. This level was designed for patients with the lowest tolerance, focusing on passive interventions to maintain muscle activity and joint mobility.
✓ Level 1: diaphragm electrical stimulation + neuromuscular electrical stimulation + joint mobilization + passive pedaling. This level introduced passive pedaling for patients with moderate tolerance to enhance lower limb circulation and muscle engagement.
✓ Level 2: diaphragm electrical stimulation + neuromuscular electrical stimulation + active pedaling. This level was for patients with the highest tolerance, incorporating active pedaling to promote motor function and cardiovascular fitness.
Control group
The control group received standard care, which included routine nursing care, passive limb positioning, and occasional joint mobilization as clinically indicated. No structured rehabilitation program was provided to the control group.
Criteria for stopping rehabilitation training
During the rehabilitation period, patients stopped training if any of the following endpoints occurred: hemodynamic instability, respiratory instability, and agitation or impaired consciousness. Details of the criterion are given in SI Appendix, Text S1.
Sedation management
Initial dose determination: The initial dose of sedative drugs was individualized for each patient according to factors such as age, physical condition, and underlying diseases. Generally, the initial infusion rate of propofol was 0.5–1.0 mg/(kg h), and that of dexmedetomidine was 0.2–0.5 μg/(kg h).
Dose adjustment: During the early-exercise period, medical staff continuously monitored the RASS score. If the RASS score was above the target range (e.g., >+2, indicating obvious agitation), the infusion rate of sedative drugs was appropriately increased. If the RASS score was below the target range (e.g., <−2, indicating excessive sedation), the drug dose was reduced accordingly. The adjustment amplitude was usually 0.2–0.5 mg/(kg h) for propofol and 0.1–0.2 μg/(kg h) for dexmedetomidine to keep the RASS score within the target range.
Data collection
Basic information on admission; Acute Physiology and Chronic Health Evaluation II (APACHE-II), RASS, Sequential Organ Failure Assessment (SOFA), and Glasgow Coma Scale (GCS) are critical scoring systems used in the ICU to assess patient severity, guide treatment, and predict outcomes (SI Appendix, Text S2); blood biochemistry test results during hospitalization; negative maximal inspiratory pressure and shallow fast breathing index (SI Appendix, Text S3); use of sedative and analgesic medication; limb muscle strength (SI Appendix, Text S4) and edema index (SI Appendix, Text S5); days of endotracheal intubation and duration of delirium; days of hospitalization; and patient outcomes over 700 days of follow-up were collected. Liver function tests, including procalcitonin (PCT), C-reactive protein (CRP), white blood cell (WBC), aspartate aminotransferase (AST), albumin, prealbumin, lactate dehydrogenase (LDH), alanine aminotransferase (ALT), were included to provide a comprehensive assessment of metabolic and organ function in critically ill patients (SI Appendix, Text S6).
Outcomes
Primary outcomes: duration of MV, length of hospital stay (d), and 660-day mortality. Secondary outcomes: change in maximal inspiratory pressure, change in shallow fast breathing index, incidence of delirium, days to delirium, total sedative and analgesic medication use, limb muscle strength, and swelling index. Details are given in SI Appendix, Text S7.
Statistical analysis
Prior to recruitment, sample size calculations were performed to ensure that the study was adequately powered. Based on previous studies 20 and prestatistical results, the estimated duration of MV in the ICU for patients in the progressive activity group and the control group was (8.00 ± 3.12) and (10.00 ± 4.51) days, respectively; the mortality rate, as the primary endpoint, was 4.4% and 10.1% for the two groups, respectively. The level of significance (α) was 0.05, power (1 − β) was 80%, allocation ratio was 1:1, and the sample size was calculated using the two independent samples mean method of PASS 15.0 software. The final calculated sample size was 350 patients that is, 175 in each group.
All continuous variables are expressed as mean ± SD, while categorical variables are expressed as n (%). The χ2 test and independent samples t-test were used to compare the differences between the control and intervention groups. Survival of mechanically ventilated ICU patients in the control and intervention groups was assessed using Kaplan–Meier survival curves. 21 In addition, subgroup analyses were performed to explore whether there were differences in the treatment and prognosis of mechanically ventilated ICU patients between the different rehabilitation exercise modalities. All data analyses were performed using SPSS (27.0 version) statistical software, and p-values less than 0.05 (*) were considered statistically significant.
Results
Basic characteristics of enrolled patients
During the research period from April 2020 to 2022, 568 consecutive patients were screened, 219 patients who did not meet the enrolment requirements were excluded, and 349 mechanically ventilated ICU patients were finally included. Among them, 176 cases were in the control group and 173 cases in the bedside assistance training intervention group. The baseline characteristics of the patients enrolled in the control and intervention groups are shown in Table 1. There were no significant differences between the enrolled patients in terms of gender and age (p > 0.05), as shown in SI Appendix, Figure S3. The main reasons for patients’ admission to the ICU and the underlying diseases and complications are shown in SI Appendix, Figure S4. In addition, there were similarly no significant differences in APACHE-II, RASS, SOFA, and GCS scores between the two groups of patients (p > 0.05). Among them, even though the p-value of 0.052 for the GCS analysis is close to the traditional threshold of significance (0.05), it still suggests that the difference in GCS scores between the two groups was not statistically significant. Thus, we are inclined to believe that this result reflects random fluctuations rather than real differences between groups. Therefore, these data are applicable for subsequent analyses.
Basic information on enrolled mechanically ventilated ICU patients.

APACHE-II: acute physiology and chronic health evaluation II; RASS: Richmond Agitation-Sedation Scale; SOFA: sequential organ failure assessment; GCS: Glasgow Coma Scale.
Effect of bedside-assisted exercise on negative inspiratory pressure and rapid shallow breathing index in mechanically ventilated ICU patients
The effect of bedside-assisted exercise on maximum negative inspiratory force (NIF) and shallow rapid breathing index (RSBI) in mechanically ventilated ICU patients is shown in Figure 1. Our results showed that the intubation time in the bedside-assisted exercise intervention group was significantly less than that in the control group (p < 0.001), with remarkable reduction of 3.75 days, as shown in Table 2. Furthermore, the investigation results showed that both NIF and RSBI were significantly changed in the bedside-assisted exercise group (p < 0.001), specifically increasing the NIF value and decreasing the RSBI, as shown in Figure 1(a) and (b). This result further confirms that bedside-assisted exercise improves respiratory function and reduces ventilator duration in mechanically ventilated ICU patients. However, investigation of different exercise modes showed that exercise modes had almost no significant effect on NIF and RSBI (p > 0.05), as shown in Figure 1(c) and (d).

Effects of (a, b) bedside-assisted exercise and (c, d) exercise mode on NIF and RSBI in mechanically ventilated ICU patients.
ICU interventions and prognostic information for enrolled mechanically ventilated patients.

ICU: intensive care unit.
Note. Sedatives and analgesics were grouped together to evaluate the total pharmacological burden on patients, as both classes of medications are commonly used in the ICU to manage pain, anxiety, and agitation.
Effect of bedside exercise on limb muscular strength and edema index
Herein, our results showed that the edema index was significantly smaller in the bedside-assisted exercise intervention group compared to the control group (p < 0.001), as shown in Figure 2(a). In addition, the investigation showed that bedside-assisted exercise significantly enhanced limb muscle strength in the intervention group (p < 0.001), as shown in Figure 2(b). Investigations of different exercise modes showed no significant difference in the change in edema index, indicating that early exercise can improve the edema index of mechanically ventilated ICU patients (p < 0.001), as shown in Figure 2(c). On the other hand, the investigation of limb muscle strength showed that composite-assisted exercise modes (Level 1) or active exercise (Level 2) modes were more beneficial (p < 0.001), as shown in Figure 2(d).
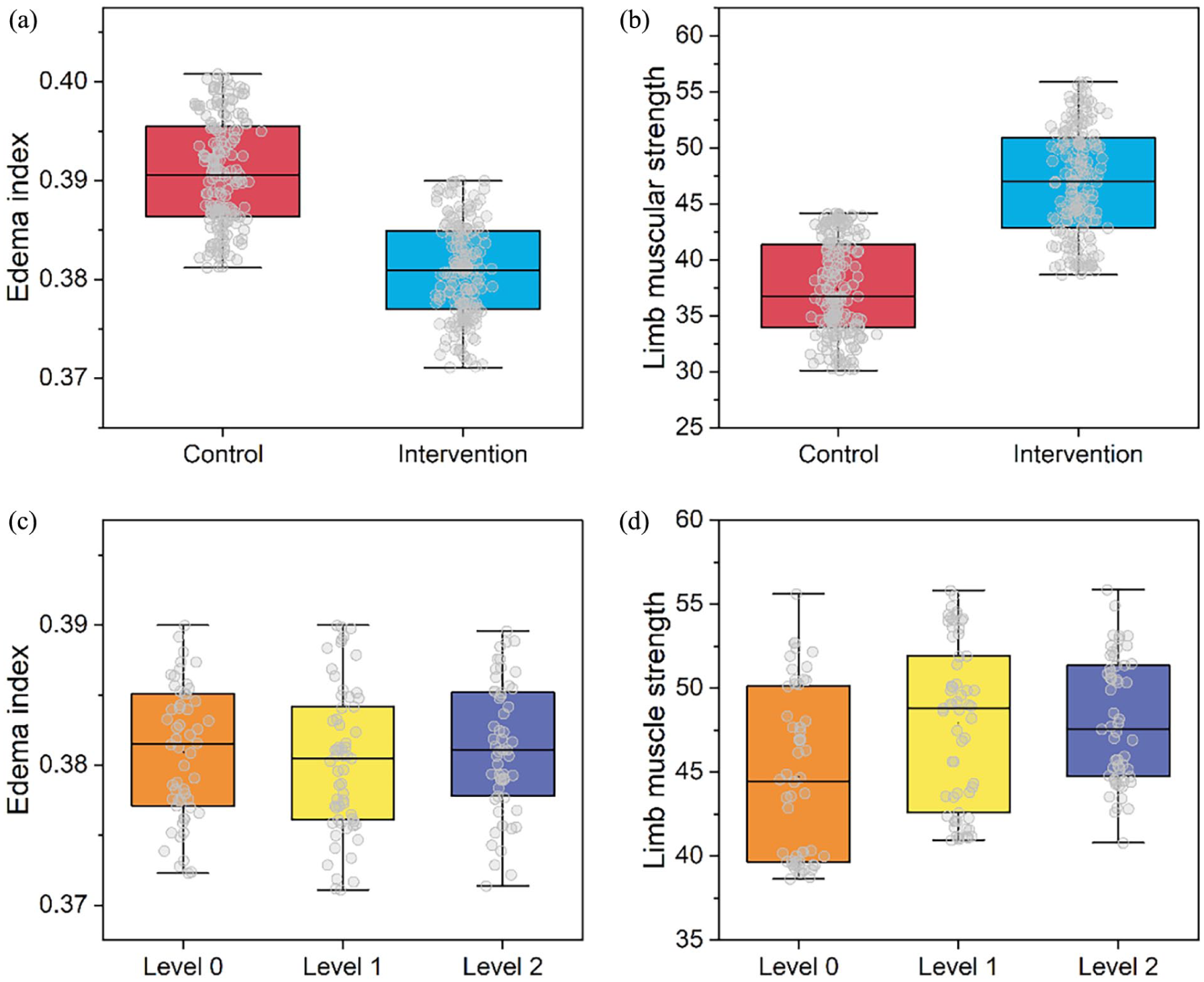
Effects of (a, b) bedside-assisted exercise as well as (c, d) exercise patterns on limb muscle strength and edema index in mechanically ventilated ICU patients.
Effect of rehabilitation training on biochemical parameters during hospitalization
Moreover, the effect of bedside-assisted exercise intervention on biochemical test indices of mechanically ventilated ICU patients during their stay in hospital was investigated (Table 3). The results showed that assisted exercise significantly improved the PCT, AST, albumin, LDH, and ALT indices of the patients compared to the control group (p < 0.001), while CRP, WBC, and prealbumin had no significant effect. Among them, higher LDH levels in the intervention group did not imply injury, but rather reflected physiologic adaptations to exercise.
Information on physicochemical examination of enrolled mechanically ventilated ICU patients.

ICU: intensive care unit.
Bedside-assisted exercise reduces medication use and duration of delirium in patients
Herein, our results showed that the duration of delirium was significantly reduced by 1.22 h in the bedside-assisted exercise intervention group compared to the control group (p < 0.001), as shown in Table 2. In addition, the investigation showed that the dose and duration of medication use were significantly lower in the bedside-assisted exercise group (p < 0.001), as shown in Table 2 and Figure 3(a) and (d). Investigations of the different exercise modes showed that the composite-assisted exercise modes on the contrary had a slight enhancement on the time and dose of medication use (p < 0.05), as shown in Figure 3(b) and (e). On the other hand, the investigation of assisted and active movement patterns showed that active movement patterns decreased the duration of drug use (p < 0.05, Figure 3(c)) and had no significant effect on the dose of drug use (p > 0.05, Figure 3(f)).

Effects of bedside-assisted exercise and movement patterns on (a–c) dose and (d–f) duration of drug administration in mechanically ventilated ICU patients.
Impact of rehabilitation training on final outcome
Patient survival was the most relevant core endpoint in all clinical analyses. Herein, the effect on ICU patients’ survival with MV with and without bedside exercise intervention and with different intervention modalities was examined by Kaplan–Meier curves.
First, our investigation showed that the duration of hospital stay was significantly shorter in the bedside-assisted exercise intervention group (p < 0.001, Table 2 and Figure 4(a)), with a reduction of 2.91 days compared with the control group. However, comparison of single- and compound-assisted exercise modes and assisted and active exercise modes showed that the exercise modes had a lesser effect on the days in hospital (Figure 4(b) and (c)). This suggests that early bedside-assisted exercise can reduce the length of hospital stay in patients.

The effect of bedside-assisted exercise intervention on the length of stay of mechanically ventilated ICU patients. (a) Overall comparison, (b) Comparison of single- and compound-assisted exercise modes, and (c) Comparison of assisted and active exercise patterns.
Comparing the mortality rates of patients in the control and intervention groups showed that patients in the control group had a higher mortality rate than those in the intervention group (SI Appendix, Figure S5 and Table 1). In addition, different modes of intervention had a slight effect on patient mortality as shown by the mortality rate: assisted exercise (Level 0) > active exercise (Level 2), and composite exercise mode (Level 1) > single assisted exercise (Level 0; SI Appendix, Figure S6). The possible explanation is that the patients in the active exercise group were in a better condition on their own than the patients in the group unable to exercise actively. However, it can still be argued that the composite-assisted movement pattern is superior to the single-assisted movement pattern.
Next, Kaplan–Meier curve analysis showed that the mean survival times of the intervention and control groups were 527.50 ± 26.54 and 461.79 ± 33.91 (d), and the median survival times were 644 and 487, respectively, as shown in Figure 5(a) and Table 4. In addition, Kaplan–Meier survival curves were explored for mechanically ventilated ICU patients with different modes of intervention, as shown in Figure 5(b). The results showed that although no evidence of regularity could be drawn for the effect of intervention modes on survival time, the curves were higher in all intervention modes than in the control group, still demonstrating the improvement of mortality outcomes by early rehabilitation exercises. The inability to draw conclusions consistent with the results of the percentage analyses may have been caused by the small number of patients. In conclusion, the intervention of bedside exercise significantly increased the survival time of mechanically ventilated ICU patients (p = 0.006), and improved the survival rate (p < 0.001).

The Kaplan–Meier curves for survival of mechanically ventilated ICU patients (a) with and without bedside exercise intervention and (b) with different intervention modalities.
Mean cumulative survival time of the enrolled mechanically ventilated ICU patients.

Discussion
As an important therapeutic measure extensively used in ICUs, MV plays a critical role in rendering respiratory support to critically ill patients. 10 For these patients with critical illnesses, MV support is frequently required for an extended period of time due to the complexity of their condition, which not only increases their bedtime but also increases the frequency of the use of protective restraints and pain medications.22,23 Studies have shown that by implementing early rehabilitation, sedation dependency effectively can be reduced while significantly shortening the duration of delirium.24,25 This approach not only helps to optimize the patient’s physiological state but also provides support at the psychological level, thereby enhancing the prognosis of mechanically ventilated ICU patients. However, there remain many barriers to early exercise in ICU patients, despite some data suggesting that early exercise can shorten hospital stay and improve function at discharge.26,27 Early mobilization may not be sufficient to prevent ICU-acquired frailty from affecting important patient outcomes and may be associated with risk. In addition, although the Guidelines for Pain, Agitation Sedation, Delirium, Inactivity, and Sleep Disruption in Adult Patients in the ICU recommend mobilization in critically ill adult patients, it does not provide recommendations for appropriate timing or protocols. 28 Therefore, there is a necessity to explore the role of different exercise modalities, including assisted and active exercise, and single and combined exercise, in influencing mechanically ventilated ICU patients, to provide data to support the design of subsequent guidelines.
In this study, we investigated the effects of several different types of bedside-assisted rehabilitation exercises on mechanically ventilated ICU patients, evaluating a number of indicators such as maximal NIF, rapid shallow breathing index (RSBI), limb muscular strength, edema index, physicochemical indices during the hospitalization period, duration of delirium, use of sedative and analgesic medication, length of hospital stay, and final prognosis.
Our results showed that early bedside-assisted exercise significantly elevated NIF and RSBI in mechanically ventilated ICU patients (p < 0.001), while significantly reducing edema and boosting limb muscle strength (p < 0.001). In addition, different early rehabilitation exercise modes had differential effects on limb muscle strength, specifically active assisted exercise mode (Level 2) was superior to passive assisted exercise mode (Level 0), and compound assisted exercise mode (Level 1) was superior to single assisted exercise mode (Level 0; p < 0.001). Although the effects of different exercise modes on NIF, RSBI, and swelling index were less significant. Qie et al. 24 showed that progressive early rehabilitation training model is beneficial for ICU mechanically ventilated patients, and this unique rehabilitation training model can effectively stimulate muscle neurons, inhibit muscle catabolism, promote axon growth in the compensatory cycle, and help to shorten the time of muscle unconsciousness and restore neuromuscular function. Another study suggested that the earlier the rehabilitation exercise, the more effective it is in improving the prognosis of mechanically ventilated ICU patients, and proposed a “time is muscle” strategy. 29 This suggests that progressive bedside-assisted exercise helps to restore muscle function and enhance limb strength. 30 Therefore, not only should the differences in exercise patterns should be considered, but also exercise patterns need to be changed as the patient’s own physical condition changes.
Clinicians in the ICU typically focus on treating circulatory, respiratory, and renal function to ensure patient survival. As a result, most ICU patients undergoing MV are given sedative and analgesic medications to reduce pain and oxygen consumption; however, this approach may result in prolonged periods of unconsciousness and bed rest.31–33 Debilitation and neuropsychiatric dysfunction are a common complication in mechanically ventilated ICU patients on sedative and analgesic medications and are associated with severe disability and long-term recovery.30,34 ICU-acquired delirium is common in patients receiving MV during their ICU stay and is associated with increased mortality, prolonged ICU and hospital stays, and prolonged ventilation. 35 Herein, our study showed that the intervention of bedside-assisted exercise was effective in reducing the dose and duration of sedative and analgesic medication use in mechanically ventilated ICU patients (p < 0.001), and in reducing intubation time and delirium duration (Table 2 and Figure 3). This is consistent with previously reported results, which indicate that early exercise can reduce delirium duration. 36 Additionally, previous study findings suggest that early activity, as a nonpharmacological intervention, has been proven to be safe, feasible, and capable of reducing delirium duration by 50%. 31 However, compound- and active-assisted movement patterns instead increased the use of sedative analgesic drugs (p < 0.05). The above phenomenon suggests that although early rehabilitative exercise is generally beneficial to patients, the specific modes of implementation still require more thought to achieve the goal of reducing sedative analgesic use. 20
Many medications used in the ICU, such as sedatives, analgesics, and antibiotics, have potential hepatotoxic effects. Monitoring AST and ALT levels helps identify drug-induced liver injury, which can inform clinical decision-making and medication adjustments. The results of the study showed that early bedside-assisted exercise significantly reduced the concentrations of indicators such as AST and ALT in the patients’ blood samples (p < 0.001), demonstrating a beneficial effect on the reduction of hepatotoxicity. Consistent with the reduction in sedative and analgesic drug use associated with early exercise, early assisted exercise may improve liver function in patients and reduce organism damage caused by complex factors such as drug use during ICU hospitalization.
Nonetheless, we acknowledge that the current study did not control for or assess all the confounding variables you mentioned. We will explicitly address this limitation in the revised manuscript. We will clearly state that while our findings suggest a potential link between early exercise and reduced AST/ALT levels, the observed differences cannot be solely and confidently attributed to early exercise or the use of sedatives/analgesics due to the presence of these unaccounted confounding factors. We will reconsider the interpretation of these findings to ensure that our conclusions are appropriately cautious and reflect the limitations of the study.
Similar to the effects of most early rehabilitation on the final prognostic outcome of mechanically ventilated ICU patients,8,37,38 bedside-assisted rehabilitation significantly reduced the length of hospital stay and increased the survival time of patients. The benefits of assisted training were attributed to improved physicochemical markers during the hospital stay, facilitated disengagement from the ventilator and improved muscle strength, all of which were effective in the long term for the patient’s subsequent life after discharge. 8
Limitation
While this study provides valuable insights into the benefits of early bedside-assisted exercise for mechanically ventilated ICU patients, it is not without limitations. The main factors limiting this study are as follows: (1) Insufficient sample size, especially the sample size of patients in the different exercise pattern groups was too small to be analyzed for more consistent conclusions; (2) The effect of the type of patient’s disease was not compared; and (3) The effect of the length of bedside-assisted exercise was not explored. In the future, conducting the abovementioned studies may help to further understand the positive effects and potential risks of bedside-assisted exercise for mechanically ventilated ICU patients.
In the future, conducting the abovementioned studies may help to further understand the positive effects and potential risks of bedside-assisted exercise for mechanically ventilated ICU patients. By addressing these limitations, subsequent research can provide more refined and evidence-based guidelines for clinical practice, ultimately improving the quality of care and prognosis for these critically ill patients.
Conclusion
All in all, a systematic understanding of bedside-assisted exercise and the different exercise modalities is important for the performance of mechanically ventilated patients during hospitalization and prognosis. During early bedside-assisted exercise interventions in mechanically ventilated ICU patients, our results identified the advantages of assisted passive to active movement pattern shifts, and single to compound movement patterns. The potential role of progressive exercise protocols is discussed. With these foundational studies, this study is expected to provide data to support subsequent clinical practice and guideline development.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251377284 – Supplemental material for Ameliorative effects of multiple bedside-assisted exercise on the rehabilitation of mechanically ventilated patients
Supplemental material, sj-docx-1-smo-10.1177_20503121251377284 for Ameliorative effects of multiple bedside-assisted exercise on the rehabilitation of mechanically ventilated patients by Ning Luo, Xiaotong Feng, Zhu Lin, Hongjie Li, Xiubao Zhao, Hua Xu and Yin Li in SAGE Open Medicine
Footnotes
Ethical considerations
Ethical approval for this study was obtained from Ethics Committee of Tianjin First Central Hospital (No. 2023DZX11)*.
Consent to participate
Verbal informed consent was obtained from all subjects before the study.
Author contribution
NL and YL: Conceptualization, Data curation, Writing – Original draft preparation. XF, ZL, HL, XZ, and HX: Data analysis, Writing – Reviewing and Editing. YL: Supervision, Writing – Original draft preparation, Writing – Reviewing and Editing. All authors have read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Tianjin Health Science and Technology Project (TJWJ2022XK023).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will be made available on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.